

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Breast milk is considered to be the ideal nutritional source for infants and is the preferred choice of feeding newborn infants. When breast feeding is not possible or a mother wants to complement breast feeding, a nutritious alternative to breast milk is necessary. There are several commercially prepared infant formulas that provide a nutritious alternative to breast milk. These include cow milk-based, soybean-based, and goat-based formulas, which differ only in their source of protein or fat. The compositions of these formulas meet guidelines for the nutrition of newborn infants that are based on the composition of breast milk [1]. Formulas with goat milk as their source of protein instead of cow milk are becoming more readily accessible in many countries. The amino acid and fatty acid profile of goat infant formula has been published [2,3]. In one controlled clinical study in New Zealand, growth of healthy infants fed goat infant formula from birth to 168 days did not differ from infants fed cow infant formula [4]. This study suggested that goat formula is similar to cow formula for the growth requirements of infants and young children. However, there are no data comparing growth rates of infants fed goat formula with breast-fed infants or a combination of breast feeding and formula feeding as used in the general population.
The present study was designed to be an in-market surveillance of goat infant formula, which has only previously been studied in controlled clinical trials. The main outcome measurements were weight gain up to 12 months and stool characteristics of infants fed formulas based on goat or cow milk compared with those fed breast milk only or a mixture of breast milk and formula milk from birth to 4 months of age.
Materials and Methods
Study subjects
This was an in-market surveillance of infant feeding practices using a prospective, birth cohort study design. Participants who enrolled were women who attended prenatal information, public, and private health clinics at 34 weeks of gestation in Seoul, South Korea. Infants born at less than 37 weeks gestation, with birth weights less than 2.5 kg, or with any congenital abnormalities were excluded from the study. A total of 1,297 healthy full term infants delivered between June 2006 and 2008 were enrolled from the initial 1,731 that were contacted during pregnancy. The reasons for not continuing in the study after birth were lost connection (275), declined participation (103), prematurity (31), congenital abnormality or stillbirth (19), and low birth weight (6). Data from an additional 321 infants were excluded due to incomplete data at 4 months. Thus, the completed dataset contained 976 infants. Written informed consent was obtained from the parents of all enrolled infants, and ethical approval was obtained from the ethics committee of Samsung Medical Centre.
Classification of feeding types
The mothers chose the type of feeding to be given to their baby, i.e., breast milk or formula and then the type of formula. The goat infant formula used in the study was restricted to a formula manufactured in New Zealand (Dairy Goat Co-operative, N.Z., Ltd). This formula contained an 80 : 20 ratio of casein:whey and had 55% of total fat from milk, with the rest consisting of a mixture of high oleic sunflower, sunflower, coconut, and soy oils. The cow infant formulas were chosen by the mothers from a range of cow infant formulas available in Korea at the time of the study. They were all whey-enhanced and contained none or a negligible amount of milk fat.
The infants were retrospectively categorized into five feeding groups according to the proportion of breast milk or formula provided during the first 4 months of age: 1) breast milk, 2) goat infant formula, 3) cow infant formula, 4) mix of breast milk and goat infant formula, and 5) mix of breast milk and cow infant formula. Infants in the breast milk, goat infant formula, or cow infant formula groups received more than 80% of all feeding from birth to 4 months of age as either breast milk or formula. Infants fed a mix of breast milk and either cow or goat infant formula received less than 80% of breast milk or formula. After 4 months, the feeding mode was varied according to the mothers' discretion, including introduction of solids.
Outcome measurements
Data on birth weight and body height, gestational age, proportion of feeding either breast milk or formula, and type of milk formula provided were recorded at enrollment. Proportions of feeds that were breast or formula as well as the type of milk formula provided were recorded monthly. Data on infant weights and body heights at birth and at 4, 8, and 12 months were obtained from routine pediatric medical examination documentation.
Stool number and consistency were recorded between 0 and 4 months. The consistency of stools was graded by mothers, using an analogue scale composed of runny, soft or pasty, soft but well formed, firm, and hard as the categories.
Statistical analysis
Anthropometric data were expressed as the means ± standard deviations. The statistical significance between feeding groups was tested by ANOVA using SPSS. When any significant differences were detected, comparisons of growth between the feeding groups were made using unpaired t-tests. The frequency and consistency of bowel motions were expressed as percentages. Statistical significances of differences in percentages among the different feeding groups were tested using model z = (p1-p2)/sqrt (p × (1-p)/n1 + p × (1-p)/n2). P1 and p2 are the percentages and p = (p1 × n1 + p2 × n2)/(n1 + n2). An effect was considered statistically significant if P < 0.05.
Results
The characteristics of the infants in each of the feeding groups are listed in Table 1. There was no difference in the baseline characteristics of the infants among the different feeding groups at birth. They shared similar gestation heights, birth weights, and heights. There were slightly more male infants in the goat formula and breast milk with cow formula groups than the other feeding groups.
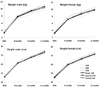
The weights and heights of the infants at 4, 8, and 12 months of age are shown in Table 2 and Fig. 1. The type of feeding, breast milk or formula or a combination of the two, had no significant influence on the weight of infants at any of the measurement time points.
Only data on the frequency and consistency of bowel motions of the infants between 0 and 4 months were analyzed. Beyond 4 months, the introduction of other foods would confound the effects of breast or formula feeding on gastrointestinal function.
The average number of stools in one day was 4.3 for the breast milk group, 4.3 for the goat formula group, 3.8 for the cow formula group, 3.9 for the breast milk with goat formula group, and 3.1 for the breast milk with cow formula group, and these were not significantly different. To understand the differences between breast milk and formula feeding more clearly, a frequency plot of the stool frequency data was generated by grouping the data according to the number of stools in one day (see Fig. 2).
The frequency of bowel motions of infants in the goat infant formula group was similar to that of infants in the breast milk group. In contrast, those in the cow infant formula group were more likely to have only 1-2 bowel motions per day and less likely to have more than > 7 bowel motions per day compared to infants in the breast milk group (P < 0.05).
The consistency of stools of infants in the cow infant formula group tended to be more formed or firm compared to those in either the breast milk or goat infant formula group (Fig. 3).
Discussion
The present study showed no influence of type of feeding during the first 4 months of life on infant growth up to 12 months. The infants were retrospectively categorized into feeding groups based on the types and amounts of formula provided to them by their mothers in the first 4 months. Infants fed goat infant formula or a combination of breast milk with goat infant formula had similar weight gains as breast-fed infants or infants fed either a mixture of breast milk and cow infant formula or cow infant formula only. This finding is consistent with a controlled study comparing exclusive feeding with goat and cow infant formula [4], confirming that the key outcomes of infant growth are being achieved when goat infant formula is used in the general population.
Although growth parameters were not significantly different between the feeding groups, there was a different pattern of more frequent bowel motions in infants fed goat infant formula compared to infants fed cow infant formula. This is consistent with data from the earlier clinical study [4]. In that study, the median number of bowel motions at day 14 was 1.5 times greater in infants fed goat infant formula compared to those fed cow infant formula, but there was no difference between the two formulas in the proportion of infants with runny or hard bowel motions. The present study extends these findings to show that the frequency and consistency of stools of infants fed goat infant formula were similar to those fed breast milk [5,6].
The frequency and consistency of stools observed in breast-fed infants in the present study are similar to the results of other studies [5,6]. These same studies report that formula-fed infants produce harder stools than breast-fed infants [5,6]. This has been attributed to the malabsorption of fat from the formula as well as formation of insoluble calcium fatty acid soaps in stools [5-8]. The goat formula used in this study contains 50% milk fat. Goat milk fat has been suggested to be more readily absorbed in animals than other milk fats [9,10]. Thus, the present results on stool formation would indicate that there is no malabsorption of goat milk fat by infants.
The differences in the number and consistency of bowel motions between the cow and goat formulas suggest that goat infant formula may behave differently in young infants' gastrointestinal tracts compared to cow infant formula. Goat milk proteins are also degraded more efficiently by adult human gastric and duodenal juices than cow milk proteins [11]. Goat milk, like breast-milk, contains a complex array of nucleotides and nucleosides, which are retained in infant formula made from goat milk [12]. Nucleotides added to cow based formulas improve the composition of the gut microbiota in formula-fed infants [13]. These combined properties of goat milk may contribute to the pattern of gastrointestinal function observed in the present study.
The present study is in contrast to previous studies that reported a slower rate of growth in infants who are exclusively breast-fed compared to formula-fed infants [14-17]. However, some studies reported no difference in weight or body height between formula or breast-fed infants [18,19]. A higher energy intake in formula-fed infants is associated with higher postnatal weight gain [16,20,21], and a recent study observed faster growth rates in infants fed formula with high protein content [18,22]. When protein content is reduced, the growth rates of formula-fed infants are also reduced similar to breast-fed infants [18,22]. Thus, it is likely that a part of the discrepancy with previous studies is related to the different energy and protein contents of the formulas used. Our results suggest that the types of formula in use in Korea do not lead to differences in weight and height between formula and breast-fed infants during the first year of life.
In conclusion, this in-market surveillance study shows that the feeding behavior of infants fed goat infant formula either alone or in combination with breast milk during first 4 months of life produces comparable growth rates over 12 months and gastrointestinal function as breast milk-fed Korean infants. Thus, there is every indication that goat infant formula, when properly formulated, is suitable for infants less than 12 months of age.




 XML Download
XML Download