

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The obesity epidemic in America has been observed in all age, gender and racial groups [1]. Data from the Centers for Disease Control and Prevention [2] show that in the years 2005-2006 more than 34% (about 72 millions) of Americans 20 years or older were obese [1,2]. This rate is more than twice as high as the 15% rate set by the Healthy People 2010 objective for obesity prevalence [3]. This figure is also considerably higher than the Healthy People 2010 baseline figure of 23% for the years 1988-94 [3]. Higher obesity rates are reported for minority groups including African Americans and Hispanics [4]. The rate of obesity is highest among middle age Americans, and it is lowest among adults between 20 and 39 years of age [1]. At the same time, even in this age category (20-39 years), close to 30% of the population is reported to be obese [1].
Obesity-related co-morbidities include cardiovascular disease, some cancers, diabetes, and hypertension [1]. The epidemic of obesity in U.S. and worldwide is associated with environmental factors including sedentary lifestyle and higher than recommended intake of calories. The increase in rates of obesity among children, adolescents and young adults should be of special concern in view of the fact that being overweight during any of these time periods will likely result in being overweight or obese throughout adulthood. Furthermore, [5] demonstrated that 42% of Caucasian, 47% of Hispanic, and 66% of African American women with a body mass index of 24 to 25 in their early 20s were obese by the ages 35 to 37. Authors also found that fewer than 15% of those who were obese at ages 20 to 22 were non-obese at ages 35 to 37 years [5]. These findings indicate that even those young adults who are in a healthy weight category may become obese within a relatively short period of time, and that although obesity can be reversed, such reversal is not very commonly seen.
North Carolina has the 17th highest rate of obesity in the nation among adults and the 5th highest among teens. North Carolina also places high on a list of obesity-related co-morbidities including diabetes (9th) and hypertension (10th) [6]. According to the Behavioral Risk Factor Surveillance System (BRFSS, CDC) 2007 report, the rate of people with BMI≥25 in North Carolina ranges from 50% among those between 18 and 24 years of age to 74.7% among adults 55 to 64 years old [7].
At the same time, previous research has demonstrated that African-Americans are less concerned with weight, body shape, dieting, or being thin [8]. In fact, recent findings have indicated that people of African American and Mexican American origin consider larger body sizes as ideal and consequently report greater body satisfaction [8-10]. Black women are less likely to diet, less fearful of weight gain, have fewer negative perceptions associated with overeating, and have more favorable body images than white women [8,11]. Those ethnic groups also have a greater risk of development secondary to obesity complications such as diabetes, hypertension, etc.
While high BMI can lead to negative self-esteem and low self evaluation, triggering risky behaviors such as uncontrollable dieting and/or overeating (e.g. anorexia or bulimia), and other weight reduction methods (e.g., excessive physical exercise, diet pills, synthetic supplements) [12,13], being overweight is linked to anxiety and depression and also can adversely affects one's quality of life [14,15]. To be proactive in preventing obesity epidemic, to promote culturally appropriate healthy attitudes and behaviors, and to understand trends in weight control strategies in different ethnicities, it is essential to investigate rates of overweight and obesity across different ethnic backgrounds.
Thus, the purpose of this cross-sectional study was: 1) to assess weight status by BMI category (underweight, normal weight, overweight, and obese); 2) assess the rate of overweight and obesity (BMI≥25) by gender and ethnic background; 3) assess whether there was a statistically significant difference in the rate of overweight and obesity by gender and ethnic background; 4) assess dieting attitudes among college students by gender and ethnicity; and 5) assess whether there was a statistically significant difference in dieting behavior by gender and ethnic background among college students attending a large public university located in the eastern part of North Carolina.
Subjects and Methods
This cross-sectional study was conducted after the University Institutional Review Board approved the research protocol.
Sample and data collection
Data were collected in large southeastern university in North Carolina. Participants of the study were undergraduate students (ages 18-25) enrolled in classes during the fall 2007 and/or spring 2008 semesters. The estimated enrollment for the spring 2008 semester was more than 25,000. In 2007, the student population at the university consisted of 40.9% male and 59.1% female students. Most students enrolled were White (75%), with Black students comprising 15.5% [16]. nder and ethnic background distribution was consistent with other universities within the University of North Carolina system [16,17].
Questionnaires were administered in conveniently chosen introductory level classes. Introductory classes are offered to many majors, and typically comprise of majors in fashion and merchandize, interior design, social work, early childhood education, nursing, psychology, criminal justice, and nutrition. Participants were ensured that participation was voluntary and confidential. The questionnaire included demographic information and self-report on body weight and height. The last part of the survey included questions related to eating attitudes and behaviors (EAT 26, reported in this study) or healthy diet questions (perception, knowledge, benefits, and will be reported in another manuscript). Questionnaires were completed at the end of class session as permitted by instructor time. Some instructors offered an extra credit for students' participation.
Among a total of 582 college students (n=106 males and n=420 females) who participated in the study and self-reported weight and height, (to calculate BMI), 348 (60%) participants (49 males and 299 females) completed the eating attitude test, while the remaining 234 (40%) participants completed a questionnaire related to healthy dieting. Only data reported on weight, eating attitudes, gender, and ethnicity will be discussed in this study. About 56 (9.6%) participants did not report their gender and those surveys were removed from the analysis.
Measures
Body Mass Index (BMI) was calculated by the following formula adopted from the [18]: weight (lb) / [height (in)]2 × 703, using self-reported heights and weights. The CDC weight categories: underweight < 18.5, normal 18.5-24.9, overweight 25.0-29.9, and obese > 30.0 were used in assessment of participants' weight status [18].
The Eating Attitude Test - (EAT-26) is a 26-item measure that assesses a broad range of symptoms of anorexia/ bulimia nervosa, including dieting and food preoccupation [19]. It is an objective self-report measure where respondents were asked to rate the frequency of each behavior (e.g., "avoid foods with sugars in them", "vomit after I have eaten", "feel extremely guilty after eating", "engage in dieting behavior") on a 6-point scale ranging from "never" to "always." Responses "always", "usually", and "often" are considered symptomatic while responses "sometimes", "rarely" and "never," are non-symptomatic of eating preoccupation and/or dieting. Responses for each item were weighted from 0 to 3, with always=3, usually=2, often=1, sometimes=0, rarely=0, and never=0. The clinical cut-off point for eating disturbances is above 20, which is indicative of serious eating disturbances or weight concerns [19]. For this study, EAT-26 was used as a continuous measure with a high score indicating more eating disturbances. The total EAT-26 score (the sum of all items) was computed for each participant. Previously validated, EAT-26 has been found to have good reliability scores (alphas ranged from .79 to .94 across studies). The reliability coefficient alpha for EAT-26 in this study was .96.
Statistical analysis
Descriptive statistics including mean, range, frequencies, and percentages were conducted using SPSS 16.0 statistical software. Analyses of the mean BMI differences between gender, and ethnic background were assessed by one-way analysis of variance (one-way ANOVA). Tukey post hoc analysis was performed to determine statistical significance between groups. Chi-square is a family of distributions commonly used for significance testing. The Chi-square test is always testing the null hypothesis, which states that there is no significant difference between the expected and observed result. Thus, Chi-square test was performed to determine whether the rate of those with BMI≥25 between gender and ethnic background was statistically significant. T-test analyses were performed to assess gender and ethnicity differences in the EAT-26 mean scores. Chi-square tests were also performed to assess gender and ethnic differences in the rate of students with EAT-26 scores above 20. For all analyses α < 0.05 was used as statistically significant difference between groups.
Results
Participant characteristics
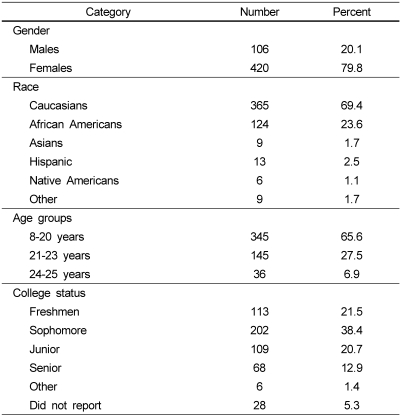
A total of 582 surveys were collected from students representing 29 different majors. Among 582 surveys collected for this study 56 participants (9.6%) did not report gender and were removed from the analysis. Most of the participants (mean [SD] age = 20.35 [2.66]) included in the analysis were females (n=420; 79.8%), Caucasian (n=365; 69.4%), and were between ages of 18 and 25. About 80.6% were freshmen, sophomores, or juniors and more than 90% did not live with parents. Detailed description of participants is presented in Table 1.
The range of BMI for the entire sample was between 14.99 to 61.40 (mean [SD]=24.4 [5.40]). Most students' BMI (n=258; 52.7%) were within the normal range category, 74 (15.1%) were underweight, 104 (21.3%) were overweight, and 53(10.8%) were obese. Table 2 introduces distribution of BMI categories (underweight, normal, overweight and obese) for Caucasians and African American participants in this study. Other ethnicities were excluded from the analysis.
Table 2 also reports on significant differences in BMI categories among genders in African American and Caucasian college students. Thus, males had significantly higher mean BMI then females (27.0 [5.86] vs. 23.8 [5.16]; F(df=520) = 3.68; P < 0.001). Males also had significantly higher rate of BMI ≥ 25 than females (48.1% vs. 28.9%) Chi-Square = 15.26 [df=1]; P < 0.001). The mean BMI among African American college students was significantly higher than the mean BMI of Caucasian students (26.2 [6.52] vs. 23.6 [6.52]; F(df=478)=14.96; P < 0.001). African American students were more likely than Caucasian students to have BMI ≥ 25 (54% vs. 24.6%; Likelihood ratio (df=1)=20.35; P < 0.001). Caucasian female students had significantly lower mean BMI than African American females (23.8[4.01] vs. 26.1 [6.91]; F(df=5)=8.301; P < 0.000). Male Caucasian students' BMI was not significantly different from male African American students' BMI (26.9 [6.13] vs. 27.0 [4.34]; F(df=3) = 0.784; P < 0.506).
Eating attitudes and behavior (EAT 26) was assessed for 348 college students as subsample (60% of the sample). Remaining 40% of the sample participated in healthy dieting survey that will be reported in future manuscript. Demographic data of this subsample is a reflection of the present sample and was comprised of 299 (85.9%) females and 49 (14.1%) males and was consisted of 294 (84.4%) Caucasians and 54 (15.6%) of African Americans. Using the formula adopted from the [18], 55.8 % of college-student females who participated in assessment of dieting behavior (n=299) were of normal weight (n=167), and 21.4% of females were overweight (n=64) and 7.3 % were severely obese (n=22) BMI > 30, with a mean BMI of 35.26. Among males (n=49) in this subsample 36.7 % (n=18) were of normal weight, and 24.5 % (n=12) were overweight with BMI > 25, while 30.6 % of males (n=15) in this subsample were severely obese (BMI > 30), with a mean BMI of 35.36. Please, refer to Table 3, which describes the BMI categories and mean EAT -26 (Eating Attitude score) for this sub-sample breaking down by gender and ethnicity.
The range of EAT-26 scores for the entire sample was from 0 to 51 with mean score of 10.58 (SD=10.32). Female respondents' mean EAT-26 score (n = 299) was 11.12 (SD=9.49), while males (n=49) mean score was 7.37 (SD=8.19). A t-test analysis showed that the difference in the mean EAT-26 scores between females and males was statistically significant (t (df=344)=5.21, P < .001). In other words, females reported more symptoms of dieting behaviors than did males in this sub-sample. Eating Attitudes scores (EAT 26) were used as a continuous measure in this study.
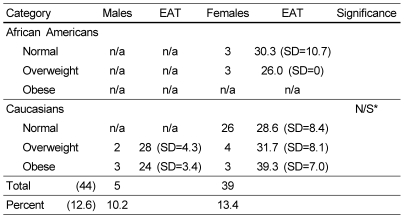
Forty-four (12.64 %) of the respondents had an EAT-26 score over 20, indicating disturbed eating tendencies and/or behavior (see Table 4). This included 39 females (13.04 %) and five males (10.2%). Among females in this group, 33 (84.6%) were Caucasian, and six (15.4%) were African Americans. All five of the males with EAT-26 score over 20 were Caucasian. Table 4 demonstrates the distribution of dieting attitudes of those students (n=44) who reported high eating attitudes scores (EAT 26 > 20) based on weight category and separated by gender and ethnicity. The rate of females with EAT-26 scores indicative of eating disturbances (score > 20) was not significantly higher than that of males (Likelihood ratio (df=1) = 0.137; P < 0.712). Similarly, no significant difference was found between the rate of Caucasian and African American students with EAT-26 scores above 20 (Likelihood ratio (df=5) = 5.207; P < 0.391).
There was no significant difference between the rate of overweight or obese students (BMI ≥ 25) and those with BMI < 25 with EAT-26 scores above 20 (14.66% vs.16.13%; Chi-square (df=1) = 0.367; P < 0.545). The percentage of students with EAT-26 above 20 by the four weight categories (BMI < 18.5; 18.5 ≤ BMI < 25; 25 ≤ BMI < 30; and BMI ≥ 30) were 5.3%, 13.5%, 11% and 23.5%, respectively. However, no significant differences between these groups were found (Chi-square (df=3) = 4.374; P < 0.224).
Discussion
According to the current report, about one third (29.8%) of college students are overweight or obese (BMI ≥ 25). At the same time, the rate of overweight and obesity in the current sample is lower than reported in previous studies on college students [20,21]. This rate is also lower than the rate reported by the NCSCHS [7]. This finding may be due to several factors. The majority of students in this sample were Caucasian. Caucasian young and older adults have a generally lower rate of BMI ≥ 25 [1,7]. Also, rates of obesity are lower among those with a higher level of education [1,4,7]. For example, according to BRFSS 2007, the rate of BMI≥25 among North Carolinians with higher level of education was between five to eight percent lower compared to the obesity rate among people with a lower level of education.
Rates of overweight or obesity among male students was higher than those seen among female students. This finding is consistent with recently reported data by [20,21]. Among adults living in North Carolina, the rate of BMI≥25 among males is close to 71% compared to 59% among female adults [7]. Other reports such as the Youth Risk Behavior Surveillance: National College Health Risk Behavior Survey have revealed that females had a higher rate of BMI≥25, However, that study was conducted approximately 15 years ago, and these and other reports' results may not be current [22]. The higher rate of overweight and obesity among males may be partially due to the fact that male students are usually satisfied with their weight and body image (e.g., broad shoulders and large torso); they want to bulk up and increase muscle and weight gain [23]. Social pressure to be thin is higher for females then males; thus, college females are more likely to perceive themselves to be overweight and will more often attempt to lose weight [14,24]. These factors may explain gender discrepancy in BMI rates, supporting previous research findings [13,15].
Consistent with recent research [1,19], rates of overweight and obesity in the current study were higher among African American than Caucasian students (54.0% vs. 24.6%). Research findings on African American students from other studies revealed the rate of overweight and obesity around 50%. For example, data from the 1995 National College Health Risk Behavior Survey showed a prevalence of overweight and obesity of 48.7% in African American students [22]. [21] reported the rate of BMI ≥ 25 among African American students was higher than 52%, based on data collected in 1999, which is congruent with the findings of current study. [20] also reported the rate of overweight and obesity in African American sample to be almost 49%.
The rate of overweight and obesity among Caucasian students (24.6%) in the current study is consistent with the rate of 26.5% reported by [24]. Data from BRFSS collected in North Carolina revealed that the overweight category (BMI≥25) among African Americans was close to 12% higher compared to Caucasians. However, current study indicates much higher rates of overweight and obesity among African American college students, which invites further investigation.
Analysis of dieting attitudes (EAT 26) demonstrated that more than 12% of students in this sample (higher rates recorded by females) reported to have disturbed eating attitudes. A study conducted by [21] reported that 20 percent of the surveyed college females had an EAT-26 score (above 20) indicative of anorexic symptomatology. Although the rate based on the current study is lower than reported by [21], these results support the generally held belief that disturbed eating attitudes and behaviors are common among college students, especially among the female college population.
Current results also suggest that disturbed eating attitudes (dieting behavior) are not just the domain of young females. Ten percent of males in this study reported disturbed eating attitudes, which is consistent with previous research [21]. Previous studies have indicated that disordered eating has been found to be most common among young, Caucasian women, and less present among African-Americans and males [4,13]. Caucasian young adults often appear to be more concerned about body weight and have more negative body cognitions than any other ethnic group [4,11]. Previous studies have also shown that individuals of differing ethnic groups hold different standards with regard to the ideal body image and attitudes toward weight [11,26]. Caucasian and African-American women hold very different definitions of beauty and body perception [11,26,27]. However, in the present study no significant difference was found between the rate of disturbed eating among Caucasian and African American students. This fact invites further investigation and could be explained by the specifics of college environment and peer pressure. This pressure, perhaps explained by social reinforcement and modeling, plays a decisive role in triggering negative self evaluation, weight control, unhealthy eating behavior, and the development of eating disorders among college females [12,21].
It is interesting to point out that the mean BMI of females who reported excessive dieting tendencies or behavior was within the normal range (BMI=24.56), and that as many as 64% of these females' BMI was within the normal range (18.5 to 24.9). In comparison, 80% of the BMIs of males who reported disturbed eating behavior were in the severely obese category with a BMI mean of 38.06. This fact supports the notion that females are more likely to diet due to a perception of being overweight, but males are more likely to diet because of their actual obese status (BMI>30) [28].
The findings of the current study should be interpreted in the light of some limitations. One of the limitations is the cross sectional design of the study, which makes causal interferences difficult. All analyses were based on self reported data. Using more precise measures of adiposity (e.g., skin fold test) can benefit future research. However, previous research with adolescents' using self-reports demonstrated high correlations between self-reported measures and actual measurements of weight and height, and is widely used in numerous studies [29]. While only 60% of participants participated in assessment of eating attitudes test, the power data specific results with regard to males of African American background was small due to small sample size. More studies are needed to explore dieting attitudes, BMIs, weight perception and weight control strategies among different ethnicities and genders.
Collected data from one university in North Carolina may limit the generalizability of the results; at the same time, the analysis revealed similarities with studies conducted on other university campuses [4,21,23]. In spite of the some limitations, presented results are important since data on the rate of overweight or obesity among college students are limited.
Data on overweight and obesity reported in this manuscript differ by gender and ethnicity, with males and African Americans having higher rates. The presented results are for the most part consistent with those published in the past [7,20]. While overweight and obesity are associated with elevated risk for a number of chronic diseases, such as heart disease, diabetes, and some types of cancer, the rate of obesity among college students should be a concern to health care professionals because obese young adults will likely remain obese throughout their adult life. This is why the findings of this study call for obesity prevention/intervention, lifestyle modification, and outreach programs among college students.
While more than 12% of students in this sample reported disordered eating attitudes or behavior, unhealthy strategies to reduce weight among college population should also not be ignored. Poor eating habits and weight control strategies among college students did not meet the recommended guidelines for dietary patterns, which may have long term health implications [12]. Weight gain and eating patterns during college years may contribute to overweight and obesity in adulthood [12]. Thus, for counselors and nutritionists working with students on weight management issues, it is crucial to educate college youth about healthy body attitudes, addressing the outcomes of obesity and dieting based on gender and ethnicity. This study highlights the importance of the college years as an excellent time for health promotion. Understanding weight attitudes and dieting tendencies based on gender and ethnicity may provide additional help to dietitians and counselors in the development of obesity prevention programs, including race and gender specific guidelines toward achievement of healthy body, healthy weight and improving quality of life.


 XML Download
XML Download