

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With the promulgation of the National Health Promotion Act in 1995, the Korea National Health and Nutrition Examination Survey (KNHANES) evolved out of the National Nutrition Survey (NNS) and the Health Interview Survey (HIS). Based on the issues and problems indicated through past several NNSs and HISs, KNHANES was devised allowing individual level data collection for diet, health behavior, and health examination. In 1998, KNHANES was conducted for the first time and the analysis on factors interrelating individual dietary intake, health status, and health behavior became possible since then.
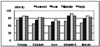
The 2nd KNHANES was conducted in 2001 and an in-depth analysis of the result was performed in 2003. A poor nutritional intake status of preschool children from low socio-economic households was noted (Fig. 1) and further analysis revealed a worsening of that problem from 1998 through 2001 as shown in Tables 1 and 2 (KHIDI & MOHW, 2003b). In the meantime, exceptionally low total fertility rate (1.08 in 2005) came to the fore (KNSO, 2009) as shown in Fig. 2, and the government was forced to devise every possible measure, short-term and long-term, to alleviate this problem. With continually decreasing number of newborns, maintaining and/or improving the health status of young children became even more important with the concept of investing in health, and the necessity to develop and implement a nationwide supplemental nutrition care program was underscored.
In this paper, we report the development of the NutriPlus+ program, and its implementation and remarkable effect on the nutritional status of the beneficiaries through 3 year pilot study and 1st year nationwide program will be reported seperately.
Development of a Supplemental Nutrition Care Program for Women, Infants, and Children, NutriPlus+
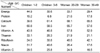
Based on the aforementioned urgent needs, a study was undertaken to develop a national scale supplemental nutrition care program for women, infants, and children adopting US WIC program as a benchmark (KHIDI, 2005). Data from 1998 KNHANES and 2001 KNHANES was used to look into a detailed nutrition and/or health problem of young children and women of child-bearing age in relation to their socio-economic status. In the midst of this process, a moderately high prevalence of iron-deficiency anemia among women in 20s thorough 40s drew a keen attention especially for the health of babies, both prenatal and postnatal. The anemia prevalence of women at 20s, 30s and 40s were 13.7%, 17.4% and 17.7% respectively in 2001 (KIHASA & MOHW, 2002). Compared to the anemia prevalence of 6.9% among US women of 20-49 years in 1999-2002 (Cusick et al., 2008), it was overwhelmingly high.
In addition to that, several studies reported much higher anemia prevalence of 33-56% among pregnant women who visits public health centers (Park & Yoon, 2001; Yu & Yoon, 1999). And the prevalence was even higher with more parity, with lower pre-pregnancy BMI, with more household members, and among small eaters and home makers. Dietary quality score and nutrition knowledge of pregnant women was poorer among women with lower blood hemoglobin values than women with normal values also (Kim & Lee, 1998; Yim & Kim, 1998). Altogether, these warranted the necessity of proper nutrition education along with supplemental foods for nutritionally vulnerable anemic pregnant women.
Supplemental food packages
Dietary intake data analysis revealed some target nutrients to be considered in the supplemental nutrition care program for economically and/or nutritionally deprived children and women (KHIDI, 2005). They were calcium, iron, vitamin A, riboflavin, and niacin (Tables 1-3). The differences in mean nutrient intake of young children among 4 income classes were remarkably obvious and several fold larger than the difference seen in similar children in the United States (ARS/USDA, 2008). Vitamin C was included in target nutrients also due to a large variability in intake by season (KHIDI & MOHW, 2003a) and the fact that the 1st and 2nd quartile intakes of women of 19-25 years corresponded to 49.4% and 104.6% of RDA (KHIDI, 2005; KNS, 2000) even in winter season with the highest vitamin C intake. Having been recognized that a single set of values could not be considered reflective of the specific nutrient requirements of each consumer (Yates, 2007), the Korean Nutrition Society had established our own DRIs in 2005 for the first time (KNS, 2005). Hence, only a set of RDA (KNS, 2000) for each sex by age group of Korean population was available in 2004, and it was used as a basis for nutrition assessment in the process of food package development. Onto this aforementioned nutrient list, energy and protein were added to ensure a proper growth of children.
Based on the list, candidates for supplemental foods were listed according to their target nutrient density and frequency of use in the Korean usual diet (KHIDI & MOHW, 2002). Another points considered in selecting supplemental foods were shelf-life and storability to maintain freshness and quality during home delivery which was under consideration as a manner of presenting service. In anddition to that, the unit cost of each food items was surely an important factor especially with a limited budget (KHIDI, 2005).
Additional analysis on the food intake of young children revealed that their milk and dairy product intake was too low not only to ensure a proper calcium intake but also for coping with the dietary guidelines set in 2003. As shown in Table 4, mean milk group intake of young children of 3-6 years from 2 lower income classes were less than one serving (200 g) although 2-3 servings are recommended in dietary guidelines for that age group (KHIDI & MOHW, 2003c). This finding prompted the inclusion of milk in the supplemental food packages in spite of rather higher unit cost.
A total of 6 different kinds of supplemental food packages (I through VI) were developed (KHIDI, 2005) for following 6 categories of beneficiaries: Infants 0-5 months, Infants 6-11 months, Young children 1-5 years, Pregnant/breastfeeding women, Non-breastfeeding postpartum women, Exclusively breastfeeding women. For each food package, major food sources for target nutrients are shown in Table 5. The amount of each supplemental food was determined based on the deficit in mean intake against recommended intake of target nutrients for each subject category and to give ideal combinations of selected items maximizing the amount of target nutrient provided while minimizing the total food cost (KHIDI, 2005). A preliminary work (KHIDI & KFDA, 2004) on portion size of Korean food was utilized in this process and the resulting numbers for food quantity per day per person by food packages are shown in Table 6. Then, the amount of target nutrients supplied by each food package was estimated accordingly as shown in Table 7 based on the Food Composition Table (RRDI, 2001). For most nutrients except iron, food packages supply more than 50% of RDA (KNS, 2000) up to 100%, and 22-45% for iron depending on the subject category.
Another point considered regarding food packages was how to provide supplemental foods to beneficiary. Because living environment in Korea is quite different from that of US, we were reluctant in adopting voucher system for benefit transfer. For most of households with income less than 100% MLE, private car was not available for grocery shopping, and for some remote areas, stores were rather distant from residence. And more than 90% of retail stores were too small in business to handle vouchers (KHIDI, 2005). Also, we were not able to find any volunteer grocer who was willing to participate in pilot study processing vouchers. Hence we proposed home delivery, either by agency or by grocers themselves. This proposal was well received by grocers and beneficiaries especially because physical inconvenience and/or incompetence of pregnant women to carry around large grocery bags.
Nutrition education
Although the supplemental food packages are important in improving nutritional status of beneficiaries, the importance of nutrition education as a core component of the NutriPlus+ should not be overlooked. From previous study (Lee et al., 2005), we have shown that relative risks of nutritional insufficiency for chronic conditions such as hypertension, hyperlipidemia and diabetes were varying from 1.25 to 1.56 for Korean adult population 40 years and older. And the cost of illness due to this nutritional insufficiency among Korean adult in 2005 was estimated to be at least 251.7 billion Won (@200 million USD) (Chung, 2007). This obviously tells us that contents of the nutrition education should include general principles, guidelines and action tips for a better dietary management of the women and children. Onto that, several points regarding the breastfeeding and complementary feeding for infants rose to the surface.
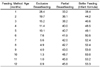
The exclusive breastfeeding rate of young children under 3 years in 1998 during their infancy was only 15.3% at 4 months (KHIDI & MOHW, 1999). And It was lowered further to 11.4% in 2001 as seen in Table 8 (KHIDI & MOHW, 2002). By the age of 12 months, the exclusive breastfeeding rate got lowered to less than 1.0% resulting in the mean duration of breastfeeding to be 19.4 weeks only (Table 9). These placed the breastfeeding promotion at the top of the priority for nutrition education for women.
Although WHO recommends to introduce complementary food to infants at 4-6 months of age, about 20% of young children under 3 years in 1998 had been given complementary food before 4 months of age (Table 10). And the mean age for complementary food introduction was lowered further from 6.3 months in 1998 to 5.9 months in 2001 (Tables 9 and 10) worsening the problem of premature and/or delayed introduction of complementary food to infants. Therefore, proper introduction of complementary food became another important part of nutrition education along with breastfeeding, dietary management and dietary behavior modification. Several modes of education implementation was proposed such as group lessons, individual counseling sessions and home visits.
Eligibility criteria
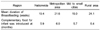
Even though we were not able to analyze dietary intake data for pregnant and/or lactating women from 1998 and 2001 survey (KNHANES) due to small numbers of corresponding subjects (KHIDI & MOHW, 1999 & 2002), it was possible to compare per capita food intake among different income classes as shown in Table 11. Other than sodium, every single nutrient intake of the lowest income class was much lower than any other classes. And the intake of the 2nd lower income class showed a very similar trend with the lowest. Together with the data in Tables 1 and 2, these justified the idea of including 2nd lower income classes also for the service provided by NutriPlus+. This, household income less than 200% of the Korean poverty guidelines (minimum monthly living expenses), became the second criterion for the eligibility to apply for the service following the residency within the district of each public health center's jurisdiction.
In addition to the women, pregnant and postpartum up to 1 year, young children's age for eligibility needed to be set. Since the Ministry of Education & Human Resources Development were responsible for school lunch program and any nutrition education within school premises, preschool children under 6 years were chosen to be cared for by NutriPlus+ under the Ministry of Health & Welfare. This proposition was especially convincing because preschool children was left almost in the blind spot for any nutritional care till then.
Once the aforementioned 3 criteria are met, they were eligible to apply for the screening process for nutritional vulnerability, the final criterion. Anemia, stunting, underweight, and inadequate nutrient intake comprised the nutritional risk factors, and anyone with one or more risk factors became eligible to participate.
Nutritional screening for eligibility
For nutritional screening, objective measures were devised especially because this step was the critical point in determining eligibility. More weights were given to biochemical and/or anthropometric parameters over simple nutrient intake insufficiency to avoid unnecessary dispute. Based on the Standard Growth Curve developed for Korean children (KPS, 1999) child with height or weight less than -2 z score was determined to be stunted or underweight. And children or women with blood hemoglobin value less than WHO cut off points (WHO, 1994) for each age/physiological categories were defined anemic.
For nutrient intake insufficiency, anyone with intake less than 75% of RDA (KNS, 2000) for any target nutrient was determined eligible by inadequate intake category.
Priority setting for program participation
Because the budget was limited and small compared to the estimated number of possible beneficiaries, a priority setting was necessary among various categories of women and children. Through an advisory committee, priority was set as follows (KHIDI, 2005), similar to that of US WIC program (FNS/USDA, 2009), grounded on the relative importance and urgency:
-
Priority I: Pregnant women, lactating women, and infants with anemia or anthropometric risk(s)
Priority II: Infants from women with clinical nutritional problems during pregnancyPriority III: Young children with anemia or anthropometric risk(s)Priority IV: Pregnant women, lactating women, and infants with inadequate nutrient intakePriority V: Young children with inadequate nutrient intakePriority VI: Non-breastfeeding postpartum women with one or more risk factor(s)
Program evaluation/assessment for the process and outcome
For the long-standing sustainability of the program we devised a protocol to evaluate and/or assess the process and outcome of the program. This was especially important for proving the program effect and securing the necessary budget (Health Promotion Fund) through convincing those responsible for compilation of government program budget.
The protocol was proposed in 2 parts, one for process and the other for outcome of the program along with establishing an agency or board to oversee the program management at public health center level and administer the protocol. For the outcome of the program, evaluation of the nutritional status change (enhancement in anthropometry and nutrition knowledge, improvement in dietary behavior and nutrient intake) was proposed for short-term measure and sample forms are shown in Fig. 3. In addition to that, decrease in anemia prevalence and change in under-weight births, infant deaths and total fertility rate were offered for long-term measures as was shown by others (Devaney, 1992; Devaney & Schirm, 1993; Yip et al., 1987) in US WIC program. Also, use of control group was advised in monitoring short-term and/or long-term measures during pilot study. On the other hand, participants' satisfaction, recordkeeping on participants' demography and service provided, and resource (personnel and budget) management were proposed as process evaluation measures.
Conclusion
A program, NutriPlus+ was developed to offer nutrition education and special supplementary foods to eligible participants, women and young children, using the WIC program of USDA as a benchmark. This was based on the result of in-depth analysis of population health and dietary intake status and nation's utmost important issue of low birth rate. We developed 6 kinds of different food packages to supplement the intake deficit in target nutrients (energy, protein, calcium, iron, vitamin A, riboflavin, niacin and vitamin C) depending on the characteristics of the beneficiaries. And, nutrition education, a critical part of this program, was customized to fit the needs of the participants in improving nutrition knowledge, attitude, and dietary behaviors. Along with this, breastfeeding was promoted for the health of both mother and baby.
The eligibility guidelines were set for residency, household income, age, pregnancy/breastfeeding and nutritional risk, which determined the priority in participation. A small-scale pilot study to examine the feasibility of the program implementation was run for the period of April through November 2005 in 3 public health centers, and 15 and 20 in following 2 years. The result of 3-year pilot study including some modification in program will be reported in a separate paper along with the ultimate nationwide implementation of the NutriPlus+ program in 2008.









 XML Download
XML Download