

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The prevalence of diabetes mellitus (DM) is increasing worldwide, and it will be a major health problem in the 21st century. Worldwide prevalence of DM was estimated to be 177 million cases in 2000 and is projected to increase to 366 million by 2030, largely owing to an aging population, increased urbanization, and more sedentary lifestyles (Wild et al., 2004).
The metabolic characteristics of diabetes patients are abnormally high concentrations of glucose in the blood and lipid metabolic abnormality (Coulston & Hollenbeck, 1988). The serum lipid abnormalities in type 2 DM are characterized by decreased HDL-C level and hypertriglyceridemia, whereas total cholesterol and LDL-C levels are similar to those in nondiabetic subjects (Kjeld et al., 2001). The important goal of DM treatment is to keep blood glucose, lipid and lipoprotein levels close to normal resulting in a reduction of coronary artery disease, a delay in onset and a major slowing in the progression of complications (Venkateswaran & Pari, 2002).
Type 2 DM is associated with increased oxidation stress (McColl et al., 1997). Free radicals, lipid peroxides and oxidation of low-density lipoproteins (LDL) have been suggested to have a role in the increased risk of cardiovascular disease (CVD) associated with type 2 DM. In diabetes, impaired glucose metabolism may lead to an increase in hydroxyl radical production. Some complications of DM are associated with increased activity of free radical-induced lipid peroxidation and accumulation of lipid peroxidation products (Palanduz et al., 2001). Mechanisms that contribute to increased lipid peroxide formation in diabetic patients include : hyperglycemic-induced glucose auto-oxidation, non-enzymatic glycation of proteins and lipids, increased sorbitol pathway activity, oxidation of advanced glycation end-products (AGEs) and cyclooxygenase dependent formation of prostaglandin H2 (PGH2) (Kesavulu et al., 2001). A variety of natural antioxidants exist to scavenge oxygen free radicals and prevent oxidative damage to biological membranes.
Soybean contains complex carbohydrates, protein, dietary fiber, oligosaccharides, phytosterol, saponin, lecithin, isoflavone, phytic acid, trypsin inhibitor, and minerals. Complex carbohydrates and dietary fiber contents contribute to low glycemic indexes, which benefit diabetic individuals (Jenkins et al., 1981) and reduce the risk of developing diabetes. Also, soybean reduces cholesterol levels (Slameron et al., 1997). When diabetic patients were fed diets rich in leguminous seeds, in addition to improved blood glucose control, lower serum TG levels were seen than when other carbohydrate sources were used, especially for individuals with raised serum TG levels (Simpson et al., 1981). It appears from several studies that soy-based diets may provide benefits in conditions associated with impaired glucose tolerance, hyperlipidemia and reduced insulin sensitivity (Hermansen et al., 2001; Kang et al., 2006; Lee, 2006). A meta-analysis of 38-controlled clinical trials indicated that consumption of 25-50 g soy protein was effective in lowering serum T-C (Anderson et al., 1995). Polichetti et al. (1996) indicated that the administration of soybean lecithin (phosphatidylcholine) to animals with experimentally induced hypercholesterolemia decreased the level of plasma T-C, LDL-C and increased that of HDL-C when compared to a similar supply of polyunsaturated fatty acid. It is reported that polyunsaturated soybean phospholipids induce a significant reduction in plasma cholesterol levels in hypercholesterolemic patients (Kurowska et al., 1997). In prospective randomized clinical trials, achieving near-normal glycemic control in patients with DM was associated with sustained, decreased rates of diabetic complications, including CVD (The diabetes control and complications trial research group, 1993). Thus, in the past two decades, investigators have focused on the blood glucose, lipid-lowering effects of soy-based foods (Tonstard et al., 2002). Accordingly, the purpose of this study was to investigate potential glucose-lowering and hypolipidemic effects of soybean in type 2 DM patients. We also examined the effects of soybean on lipid peroxidation and antioxidant enzymes activity in type 2 DM patients.
Subjects and Methods
Study subjects
This study was approved by the Ethics Committee and the Institutional Review Board for Human Subjects Research at Hanyang University Hospital, Seoul, Korea and all patients signed an informed consent document. Twenty patients with type 2 DM participated in the study. Patients were selected based on the presence of chemistry profiles and OGTT (oral glucose tolerance test). All patients had DM with fasting plasma glucose levels of 150-300 mg/dl. Patients were randomized into either a control group or a soybean group. Exclusion criteria included the presence of active liver disease or hepatic and renal dysfunction, uncontrolled hypertension, hypo-hyperthyroidism, gastrointestinal disease, severe stress, and allergy response to soybean.
Study design
The soybean was washed and dried by hot-air, roasted and ground up. Then the soybean powder was made into pills. Pills were provided to the soybean supplementation group three times a day for 4 weeks. Total daily consumption of soybean equaled 69 g. Soybean supplement of 69 g provided 23.9 g of protein and 18 g of dietary fiber. Diets for DM patients provided 1,800 kcal and 18 g of dietary fiber daily. Accordingly, the amount of dietary fiber intake in the soybean group doubled in comparison with the control group. Twenty subjects were divided into two groups. Control group was provided a diabetes diet used in the hospital. Supplemented group was provided a similar diet with the exception of soybean supplementation. The subjects continued normal daily activities and exercise patterns.
General characteristics of age, sex, dietary patterns, lifestyle, family history, diabetes duration, alcohol intake, smoking and treatment type were collected by questionnaire. During the study, patients remained on usual medications, diets or lifestyles. Nutritional assessments were performed by 24 hour recall method at the beginning and end of the experiment. Daily nutrient intake was calculated using the Computer Aided Nutritional Analysis software (Can-pro, version 3.0, The Korean Nutrition Society) based on data from Korean food-composition tables. Other health foods or supplement intakes were restricted during the experimental period.
Biochemical analysis
Blood samples were obtained at the beginning and end of the 4-week experiment. We measured blood glucose, lipids (total cholesterol, triglyceride, HDL-cholesterol, LDL-cholesterol), HbA1C after fasting, and 2 hour postprandial blood glucose levels. Blood values were analyzed by standard methods at the biochemical laboratory of Hanyang University Hospital, a certified clinical laboratory.
Laboratory analysis
For erythrocyte lysates, blood was collected in tubes containing EDTA and then centrifuged at 1,500 g for 10 minutes at 4℃. The supernatant containing the plasma and buffy coat was discarded. The red blood cell pellet was washed three times with cold saline and frozen immediately at -70℃ until analysis. Hemoglobin was separated from the blood cells by precipitation with an ethanol/chloroform mixture, followed by continuous shaking for 5 min and centrifugation at 2,500 g for 20 min. The supernatants were used to determine enzyme activity.
The total amount of lipid peroxidation products was measured with the thiobarbituric acid method, which quantifies plasma thiobarbituric acid reactive substances (TBARS) at 532 nm. Erythrocyte superoxide dismutase (SOD, EC 1.15.1.1) activity was measured using pyrogallol (Marklund, 1984). Erythrocyte catalase (CAT, EC 1.11.1.6) activity was calculated by spectrophotometrically measuring the disappearance of H2O2 at 240 nm (Aebi, 1984). Erythrocyte glutathione peroxidase (GSH-Px, EC 1.4.1.9) activity was assayed according to the method of Flohe and Gunzler (1984).
The hemoglobin concentration of lysates was determined spectrophotometrically at 546 nm using the cyanomethaemoglobin method of Mahoney et al. (1993). All assays were carried out in triplicate using a spectrophotometer (Beckman-Coulter DU 400, Fullerton, CA, USA).
Statistical analysis
All data were reported as mean ± standard error of the mean. The results were statistically analyzed by the SPSS/PC computer program (Statistical Package for Social Science 11.0). Differences between the control group and the soybean group were assessed using an independent t-test. Significance was defined as p<0.05.
Results
Table 1 shows the general characteristics of the subjects. The subjects included 8 males and 12 females. The mean age was 54.9 ± 2.4 years in the control group and 56.6 ± 2.9 years in the soybean group. Pharmacological therapy showed that 18 people used oral hypoglycemic agent and 2 people used insulin injection and oral hypoglycemic agent. The rate of alcohol intake was 40% in the control group and 20% in the soybean group. The rate of smoking was 10% in the control group and 40% in the soybean group. Height, weight, BMI, and blood pressure of both groups at the beginning were not statistically different. The mean BMI of subjects showed 24.3 kg/m2 in the control group and 25.2 kg/m2 in the soybean group. The blood pressure of two groups was in the normal range (130/80 mmHg or less).
Nutrient intake of subjects is given in Table 2. Intakes of macronutrients did not show significant differences between the control group and the soybean group with the exception of dietary fiber intake (p<0.001), which was higher in patients who were fed soybean supplement. Energy composition ratio of C:F:P was 65:19:16 in the control group, 64:20:16 in the soybean group. Mean protein intake of the soybean group was not different from that of the control group as determined by 24 hour recall including soybean supplement and the mean dietary fiber intake in patients who received soybean supplement was 31 g/d.
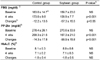
Table 3 shows the mean change in the blood glucose level of the subjects before and after the soybean supplementation. The level of fasting blood glucose (FBG), postprandial glucose (PP-2hr) and HbA1C of two groups showed no differences at the beginning. After soybean supplementation, compared to the control group, levels of FBG (p<0.001) and PP-2hr (p<0.001) were significantly lower in the soybean group, but the level of HbA1C between the control group and the soybean group showed no significant differences. The changes of FBG (p<0.05) and PP-2hr (p<0.001) in the soybean group after 4 weeks of treatment were significantly larger in comparison with the control group.
Table 4 shows the mean change in the blood lipids level of the subjects before and after 4 weeks of supplementation. The level of T-C, TG, LDL-C, HDL-C of two groups showed no differences at the beginning. After soybean supplementation, compared to the control group, levels of TG (p<0.05) were significantly lower in the soybean group. The differences in the lipid levels of the subjects before and after the supplementation were not significantly different from those of the control group,
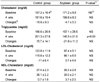
Table 5 shows the antioxidant enzyme activity of the control group and the soybean group during the soybean supplementation. TBARS levels of the soybean group were not significantly different from those of the control group. The levels of CAT (p<0.01) and GSH-Px (p<0.05) of the soybean group were significantly higher than those of the control group, while the level of SOD showed no difference between two groups.
Discussion
In this study, the mean BMI of subjects showed 24.3 kg/m2 in the control group and 25.2 kg/m2 in the soybean group. Unlike western countries where obese-type 2 diabetic patients were 70% or more, in Korea, obese-type 2 diabetic patients were 35% (Min & Huh, 1992).
The Korean Diabetes Association recommended energy composition ratio of carbohydrate 55-60%, protein 15-20%, and fat 20-25% (Kim et al., 1999). This study showed that carbohydrate intake was somewhat higher than the recommended CFP ratio. Lee et al. (1994) reported that the mean dietary fiber intake of diabetes patients was 17 g/d (10.5 g/1,000 kcal), this amount was lower than the DRI (12 g/1,000 kcal). Anderson et al. (2004) recommended dietary fiber intake of 25-50 g (15-25 g/1,000 kcal) for diabetes patients. In this study, the mean dietary fiber intake in patients who received soybean supplement was 31 g/d, which was 2.6 times higher than that in the control group and this amount was adequate for DRI.
The level of FBG and PP-2hr in the soybean group after supplementation was significantly decreased. The level of HbA1C was decreased in both groups but not statistically significant. Grace et al. (1986) had reported that soy fiber supplementation in the diets of patients with IGT (Impaired glucose tolerance) significantly reduced fasting blood glucose level and the level of insulin was significantly increased. Also, 10 g soy polysaccharide had relatively mild effects in reducing postprandial plasma glucose level (Alan et al., 1987), soybean fiber given to control rats decreased the plasma glucose at 60 min after the oral glucose test (Zacharia, 1983). The effect of improving glucose levels can be explained by the function of various components of soybean. The soybean fiber contains pectins, galactomannans and arabinogalactans with high viscosity. These substances delay gastric emptying and glucose absorption (Holf et al., 1979). The effect of soybean fiber may be attributed to reduced glucose absorption caused by slowing gastric emptying and by limiting the rate of intraluminal diffusion of glucose to the absorption surface (Zacharia, 1983). This study demonstrated the importance of soybean in the modulation of glucose metabolism.
After soybean supplementation, compared to the control group, levels of TG (p<0.05) were significantly lower in the soybean group. Alan et al. (1987) reported that soy polysaccharide significantly reduced the rise of postprandial plasma triglyceride levels. The study by Anderson et al. (1980) using high fiber diets aimed at improving diabetic control, where 20% of the fiber came from legumes, demonstrated lower serum triglyceride levels. The study of Zacharia (1983) observed that soybean fiber significantly decreased the level of triglycerides in diabetic rats. It appears that soybean fiber delayed the absorption of glucose and fatty acids from the upper small intestine, thus providing less substrate for triglycerides synthesis. In addition, a meta-analysis of 38 controlled human clinical trials indicated that significant decreases of 9% for T-C, 13% for LDL-C, and 11% for TG could be obtained from an average daily intake of around 47 g of soy protein (Anderson et al., 1995). The FDA recommends that 25 g soy protein/day may reduce CVD (Food and Drug Administration, 1999). 25 g soy protein/day is similar to the dose of our soybean supplement. This suggests that either the soy fiber component alone or a synergistic effect between soy fiber with the soy protein may be responsible for reducing the level of TG in our study.
Hyperglycemia generates reactive oxygen species which in turn cause lipid peroxidation and membrane damage (Hunt et al., 1988). In our study, soybean supplement didn't show a decreased rate of lipid peroxidation. Concerning to the increases in lipid peroxidation, the diabetic patients showed decreased activity of the antioxidant SOD, CAT, glutathione, GSH-Px, which play an important role in scavenging the toxic intermediate of incomplete oxidation. (Kumhhekar & Katyane, 1992). In this study, the levels of CAT and GSH-Px of the soybean group were significantly higher than those of the control group, while the level of SOD was similar in both groups. Soybean supplementation increased the activity of enzymes and may help to control free radicals. Lee (2006) showed that SOD and GSH-Px activities in livers of the STZ-induced diabetic rats were significantly decreased compared to the control rats. Also, administration of PPEt (Phaseolus vulgaris pod extract) significantly decreased the level of TBARS in rats with streptozotocin-induced diabetes and increased the activities of SOD, CAT and GSH-Px in diabetic rats (Subramanian & Leelavinothan, 2002). SOD is an important defense enzyme that catalyses the dismutation of superoxide radicals (McCord et al., 1971). CAT is a hemoprotein that catalyses the reduction of hydrogen peroxides and protects the tissues from highly reactive hydroxyl radicals (Chance et al., 1952). GSH-Px, an enzyme with selenium catalyzes the reduction of hydrogen peroxide and hydroperoxides to non-toxic products. These results suggest that soybean supplementation decreases oxidative stress due to a combination of improved antioxidant activities.
Results from this study suggest that supplementing the diet with soybean showed a beneficial effect on the improvement of blood glucose control, lipid metabolism and antioxidant enzyme activities in type 2 DM patients. Soybean thus may have potential use in the management of patients with DM. But, our study was limited to a comparison between the control group and the soybean group. Hence further randomized, double-blind, placebo-controlled studies should be carried out to ensure sufficient statistical power and beneficial effect of soybean.



 XML Download
XML Download