

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Korea is the one of rapidly aging countries. There are 678 million elderly people in Korea, accounting for 13.6% of its total population in 2016 [1]. Dementia causes health and social problems. It decreases quality of life of patients and their family. Cognitive impairment is a pre-stage of dementia. The conversion rate of mild cognitive impairment to dementia is approximately 10% [2]. According to a nationwide study in 2008, patients with dementia and mild cognitive impairment may increase from 13.2 million to 26.6 million by 2050 [3]. Hence, enhancing cognitive function and preventing cognitive impairment might have positive effect in reducing dementia.
Vitamins A, C, and E are involved to prevent aging, and other chronic diseases [456]. These vitamins are abundant in fruits and vegetables which have been reported to have associations with cognitive function or the risk of ischemic stroke [78]. Higher intake levels of vitamins A, C, and E have been suggested to play a role in defense against oxidative stress associated with age-related neuronal decline [91011]. However direct mechanisms how these vitamins affect the cognitive function are not clarified. Associations between levels of vitamins A, C, and E and the risk of cognitive impairment have been investigated by several previous studies [1213141516]. It has been suggested that vitamins A, C, and E have beneficial effects on the risk of cognitive impairment or cognitive function [121416]. On the contrary, several studies have found no associations between cognitive impairment or cognitive function and levels of vitamins A, C, and E [1315]. Therefore, the aim of the present study was to examine associations of serum levels of vitamins A, C, and E with the risk of cognitive impairment among elderly Koreans.
SUBJECTS AND METHODS
Study population
The Yangpyeong cohort was established to investigate risk factors of cardiovascular diseases in 2004. The present study primarily included 430 participants aged 60–79 years who were recruited for Yangpyeong cohort in 2014. A total 230 participants were finally included after excluding participants who did not respond to the Korean version of Mini-Mental State Examination for Dementia Screening (MMSE-DS) or did not provide blood specimens. This study was approved by the Institutional Review Board of Hanyang University (HYI-12-038-revision2). All participants provided written informed consent.
Anthropometric measurement and general characteristics
Height (cm) and weight (kg) of participants were measured using a stadiometer and a digital electronic weighing scale, respectively. Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Information on socio-demographic status and lifestyles of participants was collected using interviewer-administered questionnaires.
Biochemical examination
After overnight fasting, participants provided blood specimens. After blood collection, blood samples were placed in vacutainer tubes with anticoagulant. They were wrapped immediately in aluminum foil and were kept in a box to block out light. Serum levels of vitamins A, C, and E were measured by High-Performance Liquid Chromatography (HPLC, 1260 series, Agilent Technologies, USA). Serum vitamin E level was measured as alpha tocopherol, beta tocopherol, and gamma tocopherol. Beta-gamma tocopherol was calculated by adding beta tocopherol to gamma tocopherol.
For serum vitamin A levels, participants with less than 0.35 mg/L, 0.35–0.70 mg/L, and more than 0.70 mg/L were classified as severely deficient, deficient, and normal, respectively [17]. For serum vitamin C levels, participants with less than 2 µg/mL, 2–4 µg/mL, and more than 4 µg/mL were classified as deficient, insufficient, and normal, respectively [18]. For serum alpha tocopherol levels, participants with less than 5.7 mg/L and 5.7–20 mg/L were classified as deficient and normal, respectively. For serum beta-gamma tocopherol levels, participants with less than 4.3 mg/L were classified as normal range [19].
Cognitive functional examination
In the current study, cognitive function of participants was accessed by MMSE-DS. The highest score of this screening tool was 30 points, with lower score indicating decreased cognitive function. Cognitive impairment was considered when participant's score of MMSE-DS was less than mean minus 1.5 times of standard deviation (SD). Value of SD was calculated from the mean of MMSE-DS score among 1,008 healthy volunteers aged more than 60 years who had no dementia, cognitive impairment, physical diseases, or psychoneurotic disease [20].
Statistical analysis
Participants were categorized into tertiles according to serum levels of vitamins A, C, and E. Their general characteristics were analyzed according to these tertile groups. Analysis of variance (ANOVA) was used for continuous variables, and Tukey's multiple comparison test was applied as post-hoc test. Chi-square test was used for categorical variables. Fisher's exact test was used only for smoking status because current smokers were less than five according to vitamins. Odds ratios (ORs) and two-sided 95% confidence intervals (CIs) were calculated. Multivariable logistic regression analysis was performed to investigate the association between serum levels of vitamins and the risk of cognitive impairment. Statistically significance was considered when p-value was less than 0.05. All statistical analyses were performed using SAS 9.4 statistical package (SAS Institute, Inc., Cary, NC, USA).
RESULTS
Nutritional assessment of serum vitamins A, C, and E
Table 1 shows the proportion of nutritional assessment status of serum vitamins A, C, and E. For serum vitamin A levels, 31.3% (n = 72) of participants were assessed to be deficient while 0.4% (n = 1) of participants were assessed to be severely deficient. For serum vitamin C levels, 13.1% (n = 30) of participants were deficient while 1.3% (n = 3) of participants were severe deficient. All participants were classified into normal group regarding their serum alpha tocopherol and serum beta-gamma tocopherol levels.
General characteristics according to serum vitamins A, C, and E
General characteristics of these study participants according to levels of serum vitamins are shown in Table 2. The 3rd tertile group of serum vitamin A levels had higher proportions of men and current drinkers compared to the 1st tertile group. The 3rd tertile group of serum vitamin C levels had lower proportions of men, current drinkers, and current smokers compared to 1st tertile group. The 3rd tertile group of serum alpha tocopherol levels was younger than the 1st tertile group while the 3rd tertile group of serum beta-gamma tocopherol levels had higher BMI levels than the 1st tertile group.
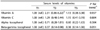
Associations between the risk of cognitive impairment and serum vitamins A, C, and E
Results of associations between the risk of cognitive impairment and serum levels of vitamin A, vitamin C, alpha tocopherol, and beta-gamma tocopherol are shown in Table 3. Serum levels of vitamin A, vitamin C, and alpha tocopherol were not significantly associated with the risk of cognitive impairment in the crude model or the multivariate model. However, the risk of cognitive impairment in the middle tertile group of beta-gamma tocopherol was 63% lower than that of the first tertile group (OR = 0.37, 95% CI = 0.14–0.98, P for trend = 0.051).
Associations between the risk of cognitive impairment and serum vitamins A, C, and E
Results of associations between serum levels of vitamins and the risk of cognitive impairment by sex, drinking status, and smoking status as subgroup analyses are shown in Table 4. The highest group with serum beta-gamma tocopherol had lower odds ratio for the risk of cognitive impairment compared to the lowest group in men (OR = 0.17, 95% CI = 0.03–0.87, P for trend = 0.028), non-drinkers or former drinkers (OR = 0.13, 95% CI = 0.02–0.66, P for trend = 0.025), and non-smokers or former smokers (OR = 0.27, 95% CI = 0.09–0.82, P for trend = 0.017).
DISCUSSION
The current study was performed to investigate associations between serum levels of vitamins (A, C, and E) and the risk of cognitive impairment in elderly Koreans. Serum levels of vitamin A and vitamin C were not associated with cognitive impairment. Serum alpha tocopherol and beta-gamma tocopherol levels were inversely associated with cognitive impairment, although associations between serum alpha tocopherol levels and cognitive impairment were not statistically significant. However, there were inverse associations between beta-gamma tocopherol levels and the risk of cognitive impairment in non-drinkers or former drinkers and non-smokers or former smokers.
The present study revealed no significant association between serum vitamin A or vitamin C level and the risk of cognitive impairment. Hu et al. [12] have reported that high levels of plasma carotenoid concentrations are related to high cognitive scores in the Nurses' Health study. However, Kang et al. [13] also reported that there is no association between serum vitamin A level and cognitive function. Consistent with our results, Lindeman et al. [15] have shown that there is no association between serum concentration of vitamin C and cognitive function. Other studies have indicated that a high score of MMSE is positively associated with serum vitamin C level [14]. Possible mechanisms involved in the association between serum levels of vitamin A or vitamin C and cognitive function are bellows. All-trans retinoic acid in carboxylic form known as vitamin A has been suggested to have antioxidation, anti-inflammatory, anti-cholinesterase, and memory-restorative functions [21]. Retinoic acid is responsible for the neuroimmunological functions and has interactions with other nuclear receptor-mediated signalling pathways. Retinoic acid is related to regeneration and cognition [22]. Furthermore, vitamin A might be able to inhibit formation of beta-amyloid fibrins. It has been found that patients with Alzheimer diseases have lower serum vitamin A levels compared to healthy controls [23]. Vitamin C has antioxidant functions. It is required for the synthesis of noradrenalin from dopamine [24]. It is associated with better memory performance [25]. Thus, further research about the effects of serum vitamins A and C on cognitive function are required.
Compared to the first tertile group of beta-gamma tocopherol level, the middle tertile group showed 63% lower risk of cognitive impairment. In addition, there were inverse associations between serum beta-gamma tocopherol levels with the risk of cognitive impairment among non-drinkers or former drinkers and non-smokers or former smokers in sub-group analyses. Consistent with our results, a previous study has suggested that cognitive function is not associated with plasma levels of tocopherols [13]. On the other hand, the study on cardiovascular risk factors, aging, and dementia has found that participants with higher serum levels of beta-tocotrienol and gamma-tocopherol have lower risk of cognitive impairment, although the highest group of gamma tocopherol level is not related to cognitive impairment [16]. Vitamin E is composed of a group of tocopherols and tocotrienols. It might contribute to the lipid antioxidation and membrane stabilization [26]. Furthermore, it has been found that beta-gamma tocopherol levels in the group with healthy life style might have more preventive effects against the risk of cognitive impairment [272829]. Thus, in the present study, beta-gamma tocopherol levels were inversely associated with the risk of cognitive impairment among non-drinkers or former drinkers and non-smokers or former smokers.
The present study has several limitations. First, this study design was a cross-sectional study. Therefore, it was difficult to examine the causal effect of vitamins A, C, and E on the risk of cognitive impairment. Second, this study was conducted in a specific rural region. Occupations of participants were mainly housewives for women and farmers for men. Education levels of these participants were different from those of the group aged more than 60 years in Korea. The percent of elementary school graduated participants was higher and the percent of high school or higher graduated participants was lower compared to generalized Korean population among similar aged group [30]. Thus, our results may not represent the entire Korean population. However, biological relevance between this study's participants and the entire Korean population may not differ. Third, variance might be decreased because of its small sample size and few participants who were deficient in serum vitamins A, C, and E.
Nevertheless, our study had the following advantages. First, we conducted the first study investigating associations between the risk of cognitive impairment and serum levels of vitamin A, C, and E in Korea. Second, the present study used serum levels of vitamins A, C, and E reflecting both food consumption and supplement intake.
In conclusion, the present study revealed that there was no significant association between serum levels of vitamin A or vitamin C and the risk of cognitive impairment. However, compared to the group with low beta-gamma tocopherol levels, the group with middle levels of beta-gamma tocopherol showed 63% lower risk of cognitive impairment. In addition, with increasing beta-gamma tocopherol levels, the risk of cognitive impairment tended to be decreased. Results of sub-group analyses revealed that serum beta-gamma tocopherol levels were inversely associated with the risk of cognitive impairment among non-drinkers or former drinkers and non-smokers or former smokers. Thus, further replication studies are needed to investigate these associations in large-scales, especially the true association between beta-gamma tocopherol level and the risk of cognitive impairment.



 XML Download
XML Download