

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stroke has emerged as the dominant chronic disease in developed countries and is a significant cause of mortality. The World Health Organization (WHO) estimated that 17 million people died from cardiovascular diseases, particularly heart attack and stroke, in 2008 [1]. In 2012, cerebrovascular disease was responsible for 9.6% of all deaths in Korea [2]. Currently, the incidence of ischemic stroke is about four times higher than that of hemorrhagic stroke [3]. Although the majority of ischemic strokes are not fatal, long-term disability is a common consequence [4]. The prognosis and management of ischemic stroke are directly related to specific mechanisms of the ischemic lesions involved [5]. Moreover, atherosclerosis, particularly intracranial atherosclerosis, represents an important cause of morbidity and mortality for stroke patients [6]. Considering the association between ischemic strokes and cerebral atherosclerosis, it is important to examine dietary factors known to influence atherosclerosis in these patients.
Many risk factors, including fat intake and unfavorable dietary behaviors, have been linked to the development of heart disease and stroke [7]. In addition, oxidative stress appears to play a role in the etiology of stroke. Correspondingly, the intake of dietary antioxidants, including those contained in fruits and vegetables, has been associated with reduced risks of stroke and atherosclerosis [89]. For example, Joshipura et al. [10] demonstrated that intake of fruits and vegetables had a protective effect on ischemic stroke in a prospective cohort study. Antioxidants may also protect low-density lipoproteins (LDLs) from oxidation and delay atherosclerotic plaque formation and platelet aggregation [11].
Several studies have also reported the benefits of micronutrients, including B vitamins and antioxidants such as vitamin E and vitamin C, in reducing the risk of stroke and improving stroke-associated functional declines [12]. Increased serum levels of homocysteine have also been strongly associated with atherosclerotic vascular diseases such as stroke. Moreover, folate and vitamin B12 play roles in homocysteine metabolism [1314]. However, the identification of specific associations between individual antioxidants present in fruits and vegetables and the risk of stroke has been inconsistent. This may be due to the fact that many studies have not classified the cases of stroke that they have examined. This is an important consideration because the etiologies of stroke subtypes can differ. In the present study, relationships between the intake of fruits and vegetables, particularly with respect to specific antioxidant nutrients and B vitamins, and cerebral atherosclerosis and stroke subtypes were examined in acute ischemic stroke patients.
SUBJECTS AND METHODS
This study was approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (Seoul, Korea, IRB No. ECT 11-59-21). All participants provided informed consent.
Recruitment of ischemic stroke patients and controls
Between February 2011 and November 2012, 147 ischemic stroke patients aged > 18 years were consecutively enrolled in this case-control study. These patients had been admitted to the hospital within 7 days of experiencing stroke symptoms. Among these patients, two were excluded due to an absence of clinical data, two due to encephalitis, and two because their energy intake was outside the range of 500-5,000 kcal. Control subjects were recruited from two senior welfare centers in Gyeonggi Province (Dongducheon, Banghwa, Korea). Inclusion criteria were: age > 65 years, absence of cardiovascular or metabolic disease, normal neurological and cardiovascular examination (including peripheral artery examination and electrocardiogram) results, and no previous nutritional counseling or therapy. A total of 144 control subjects participated in the study. For analysis between groups, control subjects were frequency-matched to ischemic stroke patients according to age and sex to achieve an approximate 1:1 ratio in 5-year age groups. For this frequency matching, 87 case subjects and 84 control subjects were excluded. Thus, the case and control groups contained 60 subjects each.
Diagnosis of cerebral atherosclerosis
Ischemic stroke patients (147 cases) were included for diagnosis of cerebral atherosclerosis. All enrolled patients had undergone computerized tomography or MRI. Cerebral artery atherosclerosis was defined as the presence of one or more vessels with 0% stenosis according to the method of the North American Symptomatic Carotid Endarterectomy Trial [15] or Warfarin versus Aspirin for Symptomatic Intracranial Disease study [16]. An independent investigator who was blinded to clinical data evaluated vascular images. Overall, a total of 141 patients were included in the comparison of dietary factors according to the presence of cerebral atherosclerosis.
Classification of ischemic stroke patients
Association of dietary intake and blood homocysteine concentrations with the risk of stroke was examined according to different subtypes categorized based on the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification [17]. Briefly, large-artery atherosclerosis (TOAST 1) was diagnosed when significant (≥ 50%) stenosis of the large artery was relevant to the infarction site. Cardio-embolism (TOAST 2) was diagnosed when the patient had at least one potential cardiac source for embolism. Small-vessel occlusion (TOAST 3) was diagnosed when a patient exhibited classical lacunar syndrome, a relevant subcortical hemispheric or brain stem lesion with a diameter ≤ 15 mm was present, stenosis of the artery relevant to the lesion was normal or < 50%, or no potential cardiac source of embolism could be identified. Undetermined etiology due to negative evaluation (TOAST 4) was recorded when no likely etiology was found despite extensive patient evaluation. Alternatively, undetermined etiology (TOAST 5) or identification of more than one cause of stroke was recorded when two or more potential mechanisms of stroke could be detected. As a result, twenty patients were excluded because of negative diffusion-weighted brain magnetic resonance imaging (MRI) results, three were excluded due to stroke of other determined etiology (SOD), and one was excluded because of an absence of clinical data. Thus, a total of 117 patients were included in comparison of dietary intake and blood homocysteine concentration among different subtypes categorized according to TOAST.
Assessment of serum cholesterol, fasting blood glucose, and blood homocysteine levels
Serum total cholesterol levels were determined by the cholesterol oxidase-N-(3-sulfopropyl)-3-methoxy-5-methylaniline method using a kit purchased from Wako Pure Chemical Industries, Ltd. Osaka, Japan). High-density lipoprotein (HDL) cholesterol levels were measured by an enzymatic method using a kit from Sekizui Co., Osaka, Japan). Fasting blood glucose levels were determined colorimetrically using a kit purchased from Wako-Pure Chemical Industries, Ltd. Co. (Osaka, Japan) according to the manufacturer's instructions. Reagents and a standard for the enzymatic detection of blood homocysteine levels were purchased from IVD Lab. Co., Ltd. (Gyeonggi-do, Korea), and assays were performed according to the manufacturer's instructions. The Auto Lab Homocysteine Parameters of a Hitachi 7600 analyzer (IVD Lab. Co., Ltd., Gyeonggi-do, Korea) were used to analyze the results.
Dietary assessment
Dietary assessment was conducted during one-on-one interviews with participants using a previously validated 111-item food frequency questionnaire (FFQ) [18]. This FFQ consisted of a total of 15 categories. The vegetable category included 17 items (lettuce/cabbage, perilla leaf/pumpkin leaf, cucumber, carrot, green chili, garlic, onion, spinach, other green vegetables (curled mallow, chard, grown daisy), zucchini, eggplant, Chinese cabbage, been sprout, white radish, bracken/sweet potato vine, balloon flower, and mushroom. The fruit category had nine items (strawberry, apple, mandarin/orange, pear, banana, watermelon, oriental melon/melon, grape, peach/plum). Guardians provided responses for subjects with speech impediments. FFQ administration took approximately 30 min and was completed within 7 days of stroke onset. Subjects were divided into two groups based on Dietary Reference Intakes for Koreans (KDRIs) recommendations for fruit and vegetable intake and recommended nutrient intake (RNI) of vitamins C, B6, and B12, and adequate intake (AI) of vitamin E. RNI and AI were also based on KDRIs [19]. Nutrient intake was expressed as intake per 1,000 kcal [20] and assessed using a Computer-Aided Nutritional Analysis Program (CANPro version 4.0; The Korean Nutrition Society, Seoul, Korea).
Statistical analysis
Statistical analyses were performed using the SAS statistical software (ver.9.3; SAS Institute, Cary, NC, USA). The means ± standard deviations (SD) are reported for continuous variables, and numbers of patients and percentages are reported for categorical variables. Data from control subjects and stroke patients were compared using Student's t-tests for continuous variables and the chi-squared or Fisher's exact test for categorical variables. Subgroup analyses were performed to compare data from stroke patients with and without cerebral atherosclerosis. The statistical significance of differences identified among stroke subtype groups was examined using one-way analysis of variance (ANOVA). Logistic regression analyses were performed to examine associations of dietary intake of antioxidants and B vitamins with the risk of ischemic stroke, with estimation of odds ratios (ORs) and 95% confidence intervals (CIs). A multivariate model was adjusted for possible confounders [21222324], including age, sex, smoking (current, past, never smoked), total cholesterol level, HDL-cholesterol level, fasting blood glucose concentration, hypertension, and regular exercise (≥ 30 minutes physical activity more than five times per week). The statistical significance of the differences identified between patients with or without cerebral atherosclerosis was examined by one-way analysis of variance (ANOVA) after adjusting for age, sex, income, smoking, and regular exercise. The statistical significance of the differences identified among the subtype groups was examined using analysis of covariance (ANCOVA). Models were adjusted for potential confounding factors based on a review of relevant literature, including age, sex, income, smoking status, and regular exercise [21222324]. Duncan's multiple range test was used for post hoc analyses. For all analyses, a P-value < 0.05 was considered statistically significant.
RESULTS
General characteristics of subjects
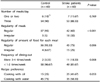
Mean age did not differ significantly between groups (Table 1). The waist:hip ratio was higher among stroke patients than control subjects (P < 0.001). Control subjects had higher total cholesterol (P = 0.019) and HDL cholesterol (P = 0.035) levels than stroke patients; however, the HDL-cholesterol/total cholesterol ratio was not different between two groups. Conversely, control subjects had lower fasting blood glucose levels (P = 0.001) than stroke patients. Hypertension (P < 0.001) and diabetes (P = 0.011) were more prevalent in stroke patients than in control subjects. The stroke group included more current smokers (P = 0.004) and fewer regular exercisers (P < 0.001) than the control group.
Dietary behavior and dietary intake of subjects
Dietary behaviors are summarized in Table 2. The number of meals consumed per day did not differ between groups. However, stroke patients were more likely to have irregular meals (30% vs. 5%, P < 0.001), consume inconsistent amounts of food at each meal (25% vs. 6.67%, P = 0.006), and eat-out (P = 0.008) than were control subjects.
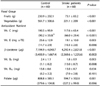
Intake of fruits and vegetables was significantly lower among stroke patients than control subjects (P < 0.001; Table 3). Correspondingly, intakes of antioxidant nutrients, including vitamin C (117.6 ± 63.4 mg vs. 190.5 ± 93.9 mg, P < 0.001), vitamin E (19.1 ± 10.0 mg α-TE vs. 25.6 ± 12.9 mg α-TE, P = 0.003) β -carotene (4,292.4 ± 2,821.8 µg vs. 7,194.9 ± 4,040.7 µg, P = 0.001), vitamin B6 (1.8 ± 0.9 mg vs. 2.4 ± 1.1 mg, P = 0.003), and folate (594.7 ± 302.6 µg vs. 808.8 ± 385.1 µg, P = 0.001) were significantly lower in stroke patients than in control subjects. These results remained consistent when nutrient intakes were expressed per 1,000 kcal.
Dietary intake of fruit and vegetables was inversely associated with the risk of ischemic stroke in unadjusted and adjusted models, including smoking status, total cholesterol, HDL cholesterol, and fasting blood glucose levels (Table 4). This inverse association of vegetables with the risk of ischemic stroke persisted after further adjustment for hypertension and regular exercise (OR, 0.001; 95% CI, 0.001-0.073). Dietary intake of vitamin C (OR, 0.093; 95% CI, 0.016-0.536) and folate (OR, 0.155; 95% CI, 0.025-0.939) were also negatively associated with the risk of stroke after adjusting for conventional risk factors. The association was not estimated for intakes of vitamin B12 because all control subjects consumed less than the RNI of the KDRIs (< 2.4 µg).
Dietary intake and homocysteine concentration in patients with and without cerebral atherosclerosis
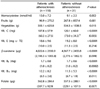
Table 5 lists dietary intake and homocysteine levels according to the presence or absence of cerebral atherosclerosis in stroke patients. Cerebral atherosclerosis plaques were present in 110/141 patients. When compared to patients without atherosclerosis, patients with atherosclerosis were older (66.4 ± 11.9 vs. 58.8 ± 11.2, P = 0.0018) and had lower income per month (P = 0.0442) (data not shown). Anthropometric and blood sample assessment results did not differ significantly, except for blood homocysteine levels. These patients had higher blood homocysteine levels (13.0 ± 7.2 nmol/ml vs. 9.1 ± 2.3 nmol/ml (P = 0.002)). Intake of vegetables, vitamin C, vitamin E, β-carotene, vitamin B6, and vitamin B12 were lower in patients with atherosclerosis. However, based on intakes expressed per 1,000 kcal, patients with atherosclerosis consumed lower levels of vitamin C (60.3 ± 275 mg vs. 73.0 ± 34.3 mg, P = 0.005), vitamin B6 (1.0 ± 0.2 mg vs. 1.0 ± 0.2 mg, P = 0.0002), vitamin B12 (6.5 ± 2.6 mg vs. 6.7 ± 1.9 mg, P = 0.011), and folate (307.7 ± 92.9 µg vs. 329.1 ± 107.1 µg, P = 0.007) than those without cerebral atherosclerosis.
Dietary intake and the blood homocysteine concentration of stroke patients according to the TOAST classification
In subanalyses of stroke subtypes (Table 6), the TOAST 5 group consisted of only four subjects with great variations in dietary intake and homocysteine level. Therefore, we combined the TOAST 4 and 5 groups and reanalyzed the data after adjusting for age, sex, income and smoking status. Overall vitamin B12 intake per 1,000 kcal differed according to the TOAST classification (P = 0.004), but post-hoc tests revealed no group differences among groups.
DISCUSSION
In the present study, ischemic stroke patients from Korea reported unfavorable dietary behaviors (e.g., irregular meals, inconsistent meal size, and frequent eating-out) compared with control subjects. Unfavorable dietary behavior was also characterized by a low intake of fruits and vegetables, and consequently, lower levels of antioxidants, vitamin B6, and folate. These results are consistent with those of a previous study that reported unfavorable dietary patterns and lower dietary quality among patients with cerebral infarction [25].
In this study, the intakes of fruits and vegetables, vitamin C, and folate were significantly associated with the risk of ischemic stroke after adjusting for confounders. Antioxidant intake was also lower in patients with atherosclerosis than in those without atherosclerosis after adjusting for energy intake per 1000 kcal. Increased oxidative stress including excessive generation of reactive oxygen species, oxidation of lipoproteins, and formation of arteriosclerotic plaques can lead to arteriosclerotic vascular damage. Oxidative stress contributes to neuronal damage induced by ischemic stroke [26]. Numerous studies have suggested that a high intake of fruits and vegetables is associated with a reduced risk of ischemic stroke, possibly due to antioxidant intake [2728]. Micronutrients may also have beneficial effects on several risk factors for stroke, including high blood pressure, insulin resistance, platelet aggregation, and atherosclerotic processes [29]. Accumulating evidence indicates that dietary and plasma β-carotene levels are inversely associated with the risk of cerebral infarction [30]. A high intake of vitamin C has also been associated with lower risks of certain stroke subtypes [21] and ischemic stroke [31].
Intakes of vitamin B6, vitamin B12, and folate affect cardiovascular health and may be beneficial for stroke prevention via the reduction of plasma homocysteine levels [143233]. Correspondingly, subclinical deficiencies of B vitamins and the antioxidant, vitamin E, appear to increase cognitive impairment in stroke patients [3435]. Several studies have also shown that diets rich in micronutrients, including B vitamins and vitamins E and C, can reduce the risk of stroke and improve post-stroke associated functional decline [12]. In the present study, stroke patients had lower intakes of vitamin B6 and folate than control subjects. Although plasma folate has not previously been associated with ischemic stroke, dietary folate has been shown to independently protect against its development [36]. Elevated homocysteine levels and deficiencies in B-group vitamin cofactors have also been found in atherosclerotic patients who have experienced stroke [37]. Furthermore, other studies have demonstrated the beneficial effect of a reduction in homocysteine concentrations was concomitant with the intake of antioxidants and B-group vitamin supplements and natural food [3738].We obtained results consistent with these findings upon comparison of homocysteine levels and antioxidant intakes between patients with and without atherosclerosis in the present study.
Several studies have reported the effects of dietary factors on stroke according to the incidence of subarachnoid hemorrhage and intra cerebral hemorrhage stroke [213940]. Although ischemic stroke constitutes approximately 80% of all stroke cases [41], very few studies have examined the relationships between dietary factors and ischemic stroke subtypes. Moreover, based on the association between ischemic stroke and cerebral atherosclerosis, the identification of dietary factors known to influence atherosclerosis is important. The present study is consistent with previous studies indicating that the intake of dietary antioxidants, is associated with reduced risks of stroke and atherosclerosis [89]. Prior to the present study, only one case-control study compared dietary scores according to TOAST classification groups, and no significant difference in dietary score was observed [42].
Lacunar infarction is the most common manifestation and prevalent type of ischemic stroke in Asians [43]. Although it is well defined, the relationship between large-artery atherosclerosis and homocysteine levels and lacunar/small artery diseases still need to be investigated [44]. High levels of mean homocysteine were detected in large-artery disease and small artery disease in etiological subtypes of ischemic stroke [45]. In the present study, although there was no significant difference in the level of homocysteine between TOAST classifications, we found that patients with lacunar origins (TOAST 3) and with large artery atherosclerosis (TOAST 1) had higher plasma homocysteine levels than those with other stroke types, which was consistent with the results of a previous study [45]. Furthermore, in the present study, patients with lacunar origins had the lowest intake of Vit B12, which indicated that low dietary intake of vitamin B12 might be a new risk factor for lacunar/small artery diseases among other etiologic subtypes of ischemic stroke. Chambers et al. showed that combination therapy of folic acid and vitamin B12 significantly improved endothelial dependent dilation [46], indicating that vitamin B12 and coronary artery disease were intimately correlated. The novel contribution of the present study concerns the potential differences in dietary components such as vitamins C, E, B6, and β-carotene according to the presence or absence of atherosclerosis and TOAST classification among Korean ischemic stroke patients, which is consistent with the results of previous studies indicating beneficial effects of antioxidants on risk of stroke. Further studies with larger sample pools are needed to determine whether dietary intakes differ according to stroke subtypes.
It should be noted that this study has several limitations. the causality of associations between antioxidant and B vitamins intakes and risk of stroke could not be determined because of the cross-sectional nature of this study. Blood analyses were not performed to assess subjects' nutritional status. Although we found differences in dietary intake according to stroke subtypes, additional studies with larger sample pools are needed to confirm these preliminary results. In addition, we could not fully exclude the possibility of unmeasured and/or residual confounding. To address this issue, we adjusted for a range of potential confounding factors. However, to the best of our knowledge, this study is the first to compare blood homocysteine levels with antioxidants and B vitamins intakes according to stroke subtypes based on the existence of atherosclerosis and TOAST classification. In addition, our results are supported by other previous studies which suggest that they are not due to chance. Nevertheless, further large-scale prospective studies are needed to identify dietary risk factors for ischemic stroke in Korea and other countries.
The present study demonstrates that ischemic stroke patients, particularly those with cerebral atherosclerosis, tend to exhibit unfavorable dietary behavior characterized by irregular meals, more frequent dining-out, and low intake of fruits and vegetables, and antioxidants. Healthy dietary recommendations may help prevent ischemic stroke. Increased intake of antioxidants could be achieved readily with a consistently healthy diet, which would benefit public health overall.



 XML Download
XML Download