

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Although the incidence of female breast cancer in most Asian countries is much lower than that in Western countries (Hirose et al., 2007), there has been a marked increase in recent years. Each year, it is estimated that one million women are newly diagnosed with breast cancer (Stewart & Kleihues, 2003). The incidence have been shown to be rising in Asian countries due to changes in lifestyle. In Korea, the incidence of breast cancer has doubled between 1987 and 2002 (Ministry of Health and Welfare, 2002).
Much of the international variation is due to differences in established genetic risk factors but diet might also contribute to risk and provide a potentially modifiable target for prevention. Recent efforts have focused on identifying dietary risk modulators. Both fat and fatty acids (Jakovljevi et al., 2002; Smith-Waner et al., 2001; Velie et al., 2000) have been shown to confer an increased risk, while fruits and vegetables (Gandini et al., 2001; Hanf & Gonder, 2005; Olsen et al., 2003) and phytoestrogens (Dai et al., 2002; Horn-Ross et al., 2001; McMichael-Phillips et al., 1998; Ziegler, 2004) afford a protective effect against breast cancer. Comparison studies of the food intake in breast cancer patients in Korean women are relatively rare. Therefore, we compared food intakes between Korean breast cancer patients and their age-matched controls.
Subjects and Methods
Subjects
The cases included 97 women with diagnosed breast cancer, and the age-matched controls included 97 women who were clinically healthy. Case subjects were collected women with histologically newly confirmed diagnosis of breast cancer at the inpatient or outpatient clinic of Yeouido St. Mary's Hospital, Seoul, Korea. The patients were chosen for the study after having a preliminary evaluation consisting of a brief medical history, smoking and alcohol habits and physical examinations. Patients with any history of liver diseases, diabetes mellitus, respiratory disorders and cardiovascular diseases were not included in the study. Controls were frequency matched by age and included outpatients in the department of general surgery at the same hospital during the same time period. Exclusion criteria for controls were those with known malignant, hormonal, gynaecological or endocrine diseases. All cases and controls were interviewed by a trained dietitian. The questionnaire included general information (age, sex and marital status), age at menarche, and pregnancy history.
Estimation of nutrient intake
We used an interviewer-administered quantitative food frequency questionnaire to estimate nutrient intake during the 2 year before the diagnosis for cases and before the interview for controls. The questionnaire included a list of 117 food items. Selection criteria were 1) most frequently consumed food items, 2) food items consumed in greatest amounts and 3) major food items supplying each nutrient, especially antioxidant vitamins. The selection was based on the Korean National Health and Nutrition Survey Report Ministry of Health and Welfare. Selected food items were categorized according to food groups and subdivided by food preparation methods, nutrient content and portion sizes. Categories and numbers of food items in each category were cereals and starches-15, soups-7, meats-12, egg-2 fish and other seafoods-12, legumes-4, milk and dairy products-5, vegetables-28 fruits-12 seasonings-3, oils-4, hot beverages and soft drink-10 and snacks-3. Subjects were asked to state the average frequency of consumption of each food item according to the categories of frequency, 'never or less than once per month', '1 per month', '2~3 per month', '1 per week', '2 per week', '3~4 per week', '5~6 per week', '1 per day', '2 per day', '3 per day'. The portion sizes were set as follows: a 0.5 serving size, a serving size, and a 1.5 serving size. The interviewer showed food models and photographs of the standard serving size, and asked the subjects to refer to those portions when selecting the amounts of foods consumed. The food frequency questionnaire was coded and analyzed for nutrient intake by a computer aided nutrient analysis program for professionals (CAN-Pro, APAC Intelligence, Seoul, Korea).
Results
Demographic characteristics
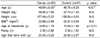
The demographic characteristics of breast cancer patients and their age-matched controls were similar (Table 1). Statistical analysis showed no significant differences between breast cancer patients and the control group in age, anthropometric variables, parity, or age at first full-term birth. However, the mean age at menarche was significantly younger in the patient group (p<0.01).
Nutrient intake of study subjects
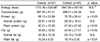
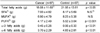
Daily nutrient intake is shown in Table 2. The mean energy intake of breast cancer patients was not significantly different than that of the control subjects. However, the intake of total protein and fat was significantly lower among breast cancer patients (p<0.05). Breast cancer patients consumed significantly less polyunsaturated fatty acids (p<0.001), ω-3 fatty acids (p<0.001) and ω-6 fatty acids (p<0.01) compared to the controls (Table 3).
The association between major antioxidant vitamin intake and the risk of breast cancer is presented in Table 4. The patient group consumed significantly less vitamin A (p<0.01), retinol (p<0.01), carotene (p<0.01), vitamin C (p<0.05) and vitamin E (p<0.001) compared to the control group.
Food stuff intake of study subjects
The mean daily selective food stuff intake is shown in Table 5. The breast cancer patients consumed significantly greater quantities of cooked rice, noodles, deep fried chicken, satsuma mandarin, Korean melon, kimchi and coffee. While they consumed a significantly lower quantity of bean curd in the legume category, onion, garlic, green pepper, sweet pepper, kale, cucumber, seasoned bean sprouts, sesame leaf, zucchini, radish, mushroom, crown daisy in the vegetable category, red pepper paste, bean paste, spicy bean paste in the seasonings category, and orange juice, grape juice, tomato juice in the beverages category compared to controls.
Among the food items from each group, the intake of eggs (p<0.01), legumes (p<0.05), vegetables (p<0.05), seasonings (p<0.001), and oils and fats (p<0.01) in the breast cancer patients was significantly lower than those of the controls (Figure 1).
Discussion
This study compared with in food intakes between Korean breast cancer patients and their age-matched controls. The demographic characteristics of breast cancer patients and their age-matched controls were similar. However the age at menarche was younger in breast cancer patients, implying that earlier exposure to hormones may be a key determinant in these subjects. A younger age at menarche is associated with a higher risk of breast cancer and increases lifetime exposure to estrogens. There has been a decrease in the average age of menarche in Western countries (Yoo et al., 2006). This, coupled with the increase in body size and fat percentage, has been attributed, in part, to nutritional factors. It has been argued that over-nutrition, in early life, causes rapid growth resulting in early menarche and in turn an increased risk of breast cancer (Law, 2000). There is evidence from cohort studies, after control for body sizes and energy intakes, that higher consumptions of grains, nuts, and legumes are associated with later menarche whereas higher consumptions of meat are associated with earlier menarche (Law, 2000).
Earlier findings from international comparisons and case-control studies suggested a positive association between a Western-style diet and breast cancer risk (Zaridze et al., 1991). However, a large scale prospective cohort of 8 years has failed to prove that breast cancer risk is reduced by a low-fat diet (Prentice et al., 2006). Results from the present study showed a lower total fat intake in the control subjects and no difference was found in total caloric intake. In our study, means of fat intake of the breast cancer patients and the controls were 8.6% and 10.1% of total energy intakes, respectively. And which is much a smaller quantity than the study population of other nations, especially European and Western countries. In a recent study carried out in the United States (Velie et al., 2000), means of daily intake of total fat was 35.0% of total energy, which is almost three times higher than those of our study population. The level of energy from fat is relatively low in Korean patients compared to their Western counterparts, and fat consumption may not be an independent risk factor at this level. Venkatraman et al. (2000) suggested that lipids are mediators of the immune system and that they may modulate its immune-regulatory effects. That study has shown that a low-fat/high-carbohydrate diet may increase inflammatory and decrease antiinflammatory immune factors, and depresses antioxidants. An association between the specific type of dietary fat consumed or the ω3/ω6 fatty acids ratio and breast cancer risk should also be considered.
In the current study, the breast cancer patient group consumed significantly less major antioxidant vitamins including vitamin A, retinol, carotene, vitamin C and vitamin E compared to the control group. And they consumed significantly lower quantities of onion, garlic, green pepper, sweet pepper, kale, cucumber, seasoned bean sprouts, sesame leaf, zucchini, radish, mushroom and crown daisy. These foods contain vitamins, minerals, fiber and non-nutritional components that may reduce the risk of cancer that can be used together or alone. Several studies have found that the consumption of vegetables and fruit is associated with a lower risk of cancer (Ching et al., 2002; Nissen et al., 2003; Rock et al., 2005). The study by Ronco et al. (1999) showed that high intake of raw and cooked vegetables seemed to be inversely associated with breast cancer. A follow-up study by Dorgan et al. (1998) reported that 105 cases of histologically confirmed breast cancer patients were diagnosed during 9.5 years, and intake and serum carotenoids were associated inversely with risk. About the study of the relationship between dietary intakes and death after breast cancer diagnosis, McEligot et al. (2006) reported nutrient including vitamin C and carotenoids intakes were significantly associated with reduced mortality. Vitamin C, vitamin E, and the carotenoids act as antioxidants, which protect DNA from oxidative damage (Rock et al., 2000). In addition, each has other chemopreventive properties (Rock et al., 2000). Carotenoids found in orange vegetables and fruits, may inhibit cell proliferation and inhibit cellular growth via conversion into retinols (Borek, 2004). A pooled analysis of 12 early case-control studies found that women in the highest fifth percentile of β-carotene consumption had a 19% reduction in breast cancer incidence compared to other postmenopausal women (Howe et al., 1990). A meta-analysis of literature from 1982 to 1997 found a similar result (Gandini et al., 2001).
In addition to its antioxidant potential, vitamin C is also crucial for immune function (Rock et al., 2000). A meta-analysis of case-control studies found a 37% reduction in breast cancer risk among postmenopausal women in the highest fifth percentile of consumption of vitamin C (Willett, 2001). In animal models, vitamin E has been found to inhibit tumors and reduce cell proliferation (Rock et al., 2000). However, available epidemiologic data do not support this effect (Willet, 2001).
In our study, breast cancer patients consumed lower quantities of red pepper paste, bean paste and spicy bean paste. Pepper is also a major source of flavonols, which may have a protective effect on breast cancer risk in laboratory and animal studies (Acklane et al., 2005; Zhong et al., 2003).
Among the food items from each group, the intake of legumes in breast cancer patients was significantly lower than those of the controls. Adlercreutz (2002) reported breast cancer rates in Asian women consuming soy-containing diets have been noted to be lower than in Western nations. In one study, women who reported having consumed soy at least once a week during adolescence showed a statistically significant reduced risk of breast cancer (Wu et al., 2002). Yamamoto et al. reported that increased miso soup and/or isoflavone consumption was associated with a reduced risk of breast cancer in Japanese women. In Ingram et al., US women were the breast cancer risk reduction associated with greater urinary excretion of phytoestrogens than in Australian women aged 30-84 years, among whom the level of consumption of traditional soy-based foods is low. Studies have investigated the effect of soy consumption on cell proliferation or biomarkers of cell proliferation in breast tissue (Hargreaves et al., 1999; Jenkins et al., 2002; Nishio et al., 2007). These data suggest that short-term dietary soy supplementation can induce proliferation of breast tissue in premenopausal women with breast disease. In contrast, soy consumption has been associated with a reduction inmammographic density (Atkinson & Bingham, 2002) whereas Maskarinec & Meng (2001) reported a positive correlation between self-reported soy food intake and percentage of breast density of women living in Hawaii. Increased mammographic density has been associated with a four to six fold increased risk of breast cancer (Atkinson & Bingham, 2002). In addition, the epidemiology of breast cancer in relation to dietary intake of phytoestrogens has been adequately reviewed and suggests that early exposure to relatively high concentrations of soy phytoestrogens may have a protective effect against breast cancer in later life (Adlercreutz, 2002). Despite the evidence that some phytoestrogens at low doses can promote the growth of breast cancer cell lines and increase biomarkers of cellular proliferation in human breast cells, current evidence suggests that a high dietary intake of soy decreases the risk of breast cancer (Maskarinec et al., 2004).
In summary, we compared the intake of nutrients and foods between Korean breast cancer patients and age matched controls. Fat intake was lower in the breast cancer patients and no difference was found in total caloric intake compared those of controls. However, that breast cancer patients consumed lesser amounts of legumes and vegetables, which are rich sources of antioxidant nutrients and phytosterols than those of the controls. Thus, dietary guidance to increase legume and vegetable intake may be beneficial in the prevention of breast cancer.



 XML Download
XML Download