

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Figures and Tables
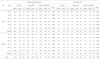
Table 1

1) Health status of people were classified by the presence of diabetes, hypertension, and metabolic syndrome, 2) Percentage of people in each age and sex group, 3) Metabolic syndrome (MetS) by the modified NCEP ATP III criteria (any 3 of 5 constitutes, for waist circumstances ≥ 90 cm in men, ≥ 80 cm in women, for triglyceride ≥ 150 mg/dL or on drug treatment for elevated triglyceride, for HDL-cholesterol < 40 mg/dL in men, < 50 mg/dL in women or on drug treatment for reduced HDL-cholesterol, for blood pressure ≥ 130 mmHg systolic blood pressure or ≥ 85 mmHg diastolic blood pressure or on antihypertensive drug treatment, for fasting glucose ≥ 100 mg/dL or on drug treatment for elevated glucose), 4) Prevalence of MetS was calculated by the criteria of modified NCEP ATP III either with or without diabetes or hypertension. 5) % of cases calculated from weighted frequency, 6) 'Control' are those who didn't have metabolic syndrome, diabetes, and hypertension, 7) 'New MetS' are those with MetS with no diabetes or hypertension diagnosed, 8) 'Control w/disease' are people who had been diagnosed with diabetes or hypertension, 9) P value by ANOVA among three groups
Table 2

1) 'Control' are those who didn't have metabolic syndrome, diabetes, and hypertension, 2) 'New MetS' are those with MetS with no diabetes or hypertension diagnosed, 3) Metabolic syndrome (MetS) by the modified NCEP ATP III criteria (any 3 of 5 constitutes, for waist circumstances ≥ 90 cm in men, ≥ 80 cm in women, for triglyceride ≥ 150 mg/dL or on drug treatment for elevated triglyceride, for HDL-cholesterol < 40 mg/dL in men, < 50 mg/dL in women or on drug treatment for reduced HDL-cholesterol, for blood pressure ≥ 130 mmHg systolic blood pressure or ≥ 85 mmHg diastolic blood pressure or on antihypertensive drug treatment, for fasting glucose ≥ 100 mg/dL or on drug treatment for elevated glucose), 4) 'Control w/disease' are people who had been diagnosed with diabetes or hypertension, 5) P value by ANOVA among three groups
Table 3
1) carbohydrate energy = [carbohydrate intake (g) × 4 (kcal/g)]/[carbohydrate intake × 4 + protein intake × 4 + fat intake × 9] × 100, 2) fat energy = [fat intake (g) × 9 (kcal/ g)]/(carbohydrate intake × 4 + protein intake × 4 + fat intake × 9) × 100, 3) 'Control' are those who didn't have metabolic syndrome, diabetes, and hypertension, 4) 'New MetS' are those with MetS with no diabetes or hypertension diagnosed, 5) Metabolic syndrome (MetS) by the modified NCEP ATP III criteria (any 3 of 5 constitutes, for waist circumstances ≥ 90 cm in men, ≥ 80 cm in women, for triglyceride ≥150 mg/dL or on drug treatment for elevated triglyceride, for HDL-cholesterol < 40 mg/dL in men, < 50 mg/dL in women or on drug treatment for reduced HDL-cholesterol, for blood pressure ≥ 130 mmHg systolic blood pressure or ≥ 85 mmHg diastolic blood pressure or on antihypertensive drug treatment, for fasting glucose ≥ 100 mg/dL or on drug treatment for elevated glucose, 6) 'Control w/disease' are people who had been diagnosed with diabetes or hypertension, 7) P value by ANOVA among three groups
Table 4

1) 'Control' are those who didn't have metabolic syndrome, diabetes, and hypertension, 2) 'New MetS' are those with MetS with no diabetes or hypertension diagnosed, 3) Metabolic syndrome (MetS) by the modified NCEP ATP III criteria any 3 of 5 constitutes, for waist circumstances ≥ 90 cm in men, ≥ 80 cm in women, for triglyceride ≥ 150 mg/dL or on drug treatment for elevated triglyceride, for HDL-cholesterol < 40 mg/dL in men, < 50 mg/dL in women or on drug treatment for reduced HDL-cholesterol, for blood pressure ≥ 130 mmHg systolic blood pressure or ≥ 85 mmHg diastolic blood pressure or on antihypertensive drug treatment, for fasting glucose ≥ 100 mg/dL or on drug treatment for elevated glucose, 4) 'Control w/disease' are people who had been diagnosed with diabetes or hypertension, 5) Odds ratio
Table 5

1) Every occasions each dish or food eaten. Some people might eat some dish or food many times a day, 2) Total carbohydrate intake from each dish or food/frequency of each dish or food, 3) 'Control' are those who didn't have metabolic syndrome, diabetes, and hypertension, 4) 'New MetS' are those with MetS with no diabetes or hypertension diagnosed, 5) Metabolic syndrome (MetS) by the modified NCEP ATP III criteria any 3 of 5 constitutes, for waist circumstances ≥ 90 cm in men, ≥ 80 cm in women, for triglyceride ≥ 150 mg/dL or on drug treatment for elevated triglyceride, for HDL-cholesterol < 40 mg/dL in men, < 50 mg/dL in women or on drug treatment for reduced HDL-cholesterol, for blood pressure ≥ 130 mmHg systolic blood pressure or ≥ 85 mmHg diastolic blood pressure or on antihypertensive drug treatment, for fasting glucose ≥ 100 mg/dL or on drug treatment for elevated glucose, 6) 'Control w/disease' are people who had been diagnosed with diabetes or hypertension, 7) Not found, 8) Rice is consumed as not only cooked rice (white rice alone) but also various types of cooked rice with other grain (s) or beans.
Table 6

1) Every occasions each dish or food eaten. Some people might eat some dish or food many times a day, 2) Total fat intake from each dish or food/frequency of each dish or food, 3) 'Control' are those who didn't have metabolic syndrome, diabetes, and hypertension, 4) 'New MetS' are those with MetS with no diabetes or hypertension diagnosed, 5) Metabolic syndrome (MetS) by the modified NCEP ATP III criteria any 3 of 5 constitutes, for waist circumstances ≥ 90 cm in men, ≥ 80 cm in women, for triglyceride ≥ 150 mg/ dL or on drug treatment for elevated triglyceride, for HDL-cholesterol < 40 mg/dL in men, < 50 mg/dL in women or on drug treatment for reduced HDL-cholesterol, for blood pressure ≥ 130 mmHg systolic blood pressure or ≥ 85 mmHg diastolic blood pressure or on antihypertensive drug treatment, for fasting glucose ≥ 100 mg/dL or on drug treatment for elevated glucose, 6) 'Control w/disease' are people who had been diagnosed with diabetes or hypertension, 7) Not found
 XML Download
XML Download