

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
The prevalence of heart failure (HF) is increasing globally and growing evidence has shown that dietary factors play an important role in preventing and improving prognosis of HF. However, little data on nutrient intake in Korean HF patients which are available to develop dietary guidelines for HF. The aims of this study were to estimate nutrient intake in 78 HF patients and evaluate whether the estimated nutrient intake is appropriate compared to dietary reference intake for Koreans. Data are presented as the ratio of actual intake and estimated average requirement (EAR) for each nutrient. The result showed that the average nutrient intakes including total energy and protein met EAR in total patients. However, the deficiencies in mineral and vitamin intakes were found. Moreover, the proportion of subjects with lower intake than EAR was substantial. The results showed that the proportion of male HF patients with inferior intakes to EAR in calcium, potassium (compared to adequate intake: AI), folate and vitamin B12 were 38%, 79%, 38%, and 65%, respectively. Also, the proportion of female HF patients with inferior intakes to EAR in calcium, potassium (compared to AI), folate and vitamin B12 were 35%, 88%, 38% and 40%, respectively. In particular, the elderly with HF (≥ 70 yrs, n = 28) showed more serious deficiencies in calcium, potassium (compared to AI), folate and vitamin B12. In summary, the intakes of potassium, calcium, folate, and vitamin B12 were not sufficient to meet EAR in HF patients. Furthermore, the proportions of subjects with lower intake than EAR in these nutrients were substantial, raising the possibility that these micronutrients may be involved in the pathogenesis of HF. Practical dietary guideline for HF patients is needed to improve prognosis of HF.
Figures and Tables
Fig. 1
The proportion of HF subjects with inadequate nutrient intakes for EAR. *: The proportion of HF subjects with inadequate nutrient intake for AI. EAR: estimated average requirements, AI: adequate intake.
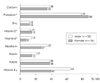
Fig. 2
The proportion of older (> = 70 yr) HF subjects with inadequate nutrient intakes for EAR. *: The proportion of HF subjects with inadequate nutrient intake for AI. EAR: estimated average requirements, AI: adequate intake.




References
1. Van Jaarsveld CH, Ranchor AV, Kempen GI, Coyne JC, Van Veldhuisen DJ, Sanderman R. Epidemiology of heart failure in a community-based study of subjects aged > or = 57 years: incidence and long-term survival. Eur J Heart Fail. 2006. 8(1):23–30.

2. Redfield MM. Heart failure-an epidemic of uncertain proportions. N Engl J Med. 2002. 347(18):1442–1444.
3. Song EK, Kim CJ, Yoo IY, Kim GY, Ju HY, Ha JW. Factors influencing functional status in patients with heart failure. J Korean Acad Nurs. 2006. 36(5):853–862.
4. McMurray John J V, Pfeffer Marc A. Heart failure. Lancet. 2005. 365(9474):1877–1889.
5. Davis RC, Hobbs FD R, Lip GY H. ABC of heart failure: history and epidemiology. BMJ. 2000. 320(7226):39–42.
6. Adams KF, Arnold JMO, Baker DW. HFSA 2006 comprehensive heart failure practice guidelines. J Card Fail. 2006. 12(1):e29–e37.
7. Gorelik O, Almoznino-Sarafian D, Feder I, Wachsman O, Alon I, Litvinjuk V, Roshovsky M, Modai D, Cohen N. Dietary intake of various nutrients in older patients with congestive heart failure. Cardiology. 2003. 99(4):177–181.
8. Witte KK, Clark AL, Cleland JG. Chronic heart failure and micronutrients. J Am Coll Cardiol. 2001. 37(7):1765–1774.
9. De Lorgeril M, Salen P, Accominotti M, Cadau M, Steghens JP, Boucher F, de Leiris J. Dietary and blood antioxidants in patients with chronic heart failure: insights into the potential importance of selenium in heart failure. Eur J Heart Fail. 2001. 3(6):661–669.
10. Witte KK, Nikitin NP, Parker AC, von Haehling S, Volk HD, Anker SD, Clark AL, Cleland JG. The effect of micronutrient supplementation on quality-of life and left ventricular function in elderly patients with chronic heart failure. Eur Heart J. 2005. 26(21):2238–2244.
11. Shane E, Mancini D, Aaronson K, Silverberg SJ, Seibel MJ, Addesso V, McMahon DJ. Bone mass, vitamin D deficiency and hypoparathyroidism in congestive heart failure. Am J Med. 1997. 103(3):197–207.
12. Colin Ramirez E, Castillo Martinez L, Orea Tejeda A, Rebollar Gonzalez V, Narvaez David R, Asensio Lafuente E. Effects of a nutritional intervention on body composition, clinical status, and quality of life in patients with heart failure. Nutrition. 2004. 20(10):890–895.
13. Shim JS, Oh KW, Suh I, Kim MY, Shon CY, Lee EJ, Nam CM. A study on validity of a semiquantitative food frequency questionnaire of Korean adults. Korean J Community Nutr. 2002. 7(4):484–494.
14. Institute of Food and Nutrition Science in Yonsei University. Fatty acid composition of Korean foods. 1995. Shin Gwang Press.
15. National Rural Living Science Institute. Food composition table. 1996. 5th Revision.
16. Korea Food and Drug Administration in Ministry of Health and Welfare. Korean food composition table. 1996.
17. The Korean Nutrition Society. Dietary reference intakes for Koreans. 2005. Seoul:
18. Berry C, Clark AL. Catabolism in chronic heart failure. Eur Heart J. 2000. 21(7):521–532.
19. Poehlman ET, Scheffers J, Gottlieb SS, Fisher ML, Vaitekevicius P. Increased resting metabolic rate in patients with congestive heart failure. Ann Intern Med. 1994. 121(11):860–862.
20. Riley M, Elborn JS, McKane WR, Bell N, Stanford CF, Nicholls DP. Resting energy expenditure in chronic cardiac failure. Clin Sci. 1991. 80(6):633–639.
21. Toth MJ, Gottlieb SS, Fisher ML, Poehlman ET. Daily energy requirements in heart failure patients. Metabolism. 1997. 46(11):1294–1298.
22. Pasini E, Aquilani R, Gheorghiade M, Dioguardi FS. Malnutrition, muscle wasting and cachexia in chronic heart failure: the nutritional approach. Ital Heart J. 2003. 4(4):232–235.
23. Filippatos GS, Anker SD, Kremastinos DT. Pathophysiology of peripheral muscle wasting in cardiac cachexia. Curr Opin Clin Nutr Metab Care. 2005. 8(3):249–254.
24. Horwich TB, Kalantar-Zadeh K, MacLellan RW, Fonarow GC. Albumin levels predict survival in patients with systolic heart failure. Am Heart J. 2008. 155(5):883–889.
25. Curtis JP, Selter JG, Wang Y, Rathore SS, Jovin IS, Jadbabaie F, Kosiborod M, Portnay EL, Sokol SI, Bader F, Krumholz HM. The obesity paradox: body mass index and outcomes in patients with heart failure. Arch Intern Med. 2005. 165(1):55–61.
26. Suzanne L, Nancy A. Nutrition and congestive heart failure in the prevention and treatment of disease. 2001. Academic press;325–333.
27. Greger JL. Dietary intake and nutritional status in regard to zinc of institutionalized aged. J Gerontol. 1977. 32(5):549–553.
28. Sullivan JF, Blotcky AJ, Jetton MM, Hahn HK, Burch RE. Serum levels of selenium, calcium, copper, magnesium, manganese and zinc in various human diseases. J Nutr. 1979. 109(8):1432–1437.
29. Ripa S, Ripa R, Giustiniani S. Are failured cardiomyopathies a zinc-deficit related disease? A study on Zn and Cu in patients with chronic failured dilated and hypertrophic cardiomyopathies. Minerva Med. 1998. 89(11-12):397–403.
30. Golik A, Cohen N, Ramot Y, Maor J, Moses R, Weissgarten J, Leonov Y, Modai D. Type II diabetes mellitus, congestive cardiac failure and zinc metabolism. Biol Trace Elem Res. 1993. 39(2-3):171–175.
31. Coudray C, Charlon V, de Leiris J, Favier A. Effect of zinc deficiency on lipid peroxidation status and infarct size in rat hearts. Int J Cardiol. 1993. 41(2):109–113.
32. Kang YJ. The antioxidant function of metallothionein in the heart. Proc Soc Exp Biol Med. 1999. 222(3):263–273.
33. Anker SD, Clark AL, Teixeira MM, Hellewell PG, Coats AJ. Loss of bone mineral in patients with cachexia due to chronic heart failure. Am J Cardiol. 1999. 83(4):612–615.
34. Zittermann A, Schleithoff SS, Koerfer R. Markers of bone metabolism in congestive heart failure. Clin Chim Acta. 2006. 366(1-2):27–36.
35. Maclaughlin J, Holick MF. Aging decreases the capacity of human skin to produce vitamin D3. J Clin Invest. 1985. 76(4):1536–1538.
36. Dalery K, Lussier-Cacan S, Selhub J, Davignon J, Latour Y, Genest J Jr. Homocysteine and coronary artery disease in French Canadian subjects: relation with vitamins B12, B6, pyridoxal phosphate and folate. Am J Cardiol. 1995. 75(16):1107–1111.
37. Kang SS, Wong PW, Norusis M. Homocysteinemia due to folate deficiency. Metabolism. 1987. 36(5):458–462.
38. Nygord O, Refsum H, Ueland PM, Vollset SE. Major lifestyle determinants of plasma total homocysteine distribution: the Hordaland Homocysteine study. Am J Clin Nutr. 1998. 67(2):263–270.
 XML Download
XML Download