

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Korea's immigrant population has been rapidly increasing because of economic growth, government policies designed to attract foreigners, and a decline in industrial populations resulting from changing national attitudes. In 2013, the number of foreigners in Korea, including ex-patriots, was approximately 1,576,000, exceeding 3% of the total population for the first time [1]. The majority of foreign-born individuals living in Korea were from Asia, primarily China (49.4%), followed by the United States (8.5%), Vietnam (7.6%), Japan (3.6%), and the Philippines (3.0%). However, the domiciles of foreign-born individuals are expanding to include Africa and other parts of the world [1]. At the same time, the number of overseas students attending Korean universities increased from 49,000 in 2007 to 86,000 in 2013, with students entering the country from various regions, including China (58.6%), Japan (5.1%), Mongolia (4.5%), Vietnam (3.5%), the United States (3.1%), and Taiwan (2.0%) [2]. These changes are closely related to the spread of infectious diseases. In 2014, a measles outbreak in Asian countries such as the Philippines and Vietnam spread primarily to schools in Korea, a country that had previously eradicated measles [3]. Vaccination of the immigrant population is therefore an important issue for the health of both foreigners living in this country and Korean people. Infectious diseases, vaccination rates, and mandatory childhood vaccination schedules vary by country. Difference in the seroprevalence of vaccine preventable diseases and the nationality of foreigners residing domestically must be considered when developing vaccination recommendation. Some Western countries have developed vaccination programs and recommendations for their immigrant population. However, Korea had not yet developed such vaccination recommendations, which has caused difficulties for front-line organizations responsible for vaccinations.
The Committee of Adult Immunization of the Korean Society of Infectious Diseases (KSID) recognized the necessity of vaccination recommendations for adult immigrants to respond to the changing domestic environment. After forming a team of experts and gathering data through a literature review, we developed vaccination recommendations based on the current situation in Korea. Unlike developed countries with sufficient statistical data to inform public health policies and mandatory childhood vaccination programs, less developed and developing countries have little or no data regarding disease statistics, childhood vaccination policies, or population immunity. We emphasize the difficulties in developing accurate and objective recommendations because of these data limitations. Our recommendations were developed by selecting infectious diseases with high morbidity in immigrant populations living in Korea for at least 3 months (depending on the vaccine, these recommendations may be applied for stays of less than 2 months).
Selection of target diseases for vaccination and development of a vaccine administration check list
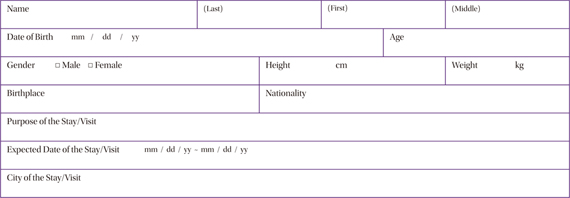
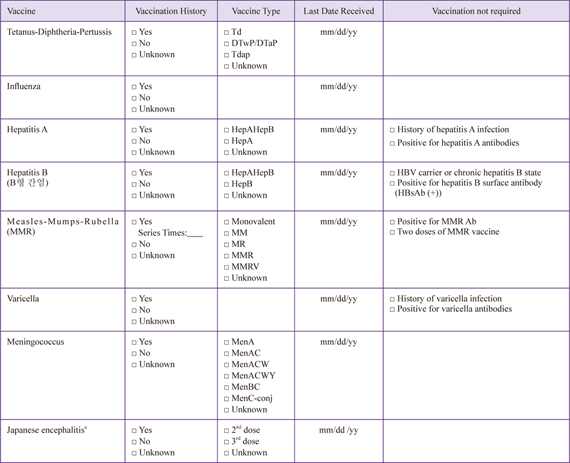
We reviewed target diseases for vaccination listed in the adult vaccination recommendation from the KSID, including tetanus, diphtheria, pertussis, influenza, hepatitis A, hepatitis B, measles, mumps, rubella, varicella, human papillomavirus (HPV), meningococcus, pneumococcus, and herpes zoster; we also included Japanese encephalitis [4]. Among these diseases, we developed recommendations for tetanus, diphtheria, pertussis, hepatitis A, measles, mumps, rubella, varicella, and Japanese encephalitis, which exhibit regional differences in disease epidemiology and current vaccine regimes, thus requiring additional consideration for the immigrant population. For the remaining diseases, we followed the current KSID adult vaccination recommendations. We also developed a vaccination confirmation form for use by clinics treating foreign patients (Appendix 1).
1. Tetanus-diphtheria-pertussis (Tdap) vaccine
<Recommendation for Tdap vaccination>
Pre-exposure vaccination
a. Adults who completed their primary series of vaccination but who did not receive the Tdap vaccine or are unaware of their Tdap vaccine status should be administered the Tdap vaccine and a tetanus-diphtheria (Td) booster every 10 years.
b. Adults who may or may not have received three doses of primary vaccination should be administered the Tdap vaccine, followed by a Td booster 4-6 weeks later, a Td booster 6-12 months later, and a Td booster every 10 years thereafter.
c. Women with no history of Tdap vaccination should be vaccinated once before pregnancy or immediately after giving birth. However, if pertussis is prevalent in Korea, vaccinations are recommended for women at 27-36 week of pregnancy to prevent pertussis in their newborns.
Post-exposure vaccination
a. Administration of Tdap or Td vaccines to prevent tetanus should be based on the previous DTP or Td vaccination history and wound cleanliness (Table).
A. Evidence for recommendations
The importance of adult pertussis vaccination was emphasized in countries with high primary childhood vaccination rates after pertussis outbreaks in adults since the 1990s. The source of infections in infants less than 1 year of age with insufficient vaccine-induced immunity was determined to be adults. The US Advisory Committee on Immunization Practices emphasized the need for adult Tdap vaccinations for pregnant women in particular and recommended Tdap vaccination at 27-36 weeks of pregnancy regardless of the previous Td/Tdap vaccination history [5]. Whereas approximately 20 cases of pertussis have been reported in Korea each year since 2001, this number increased to 66 in 2009 and 97 in 2011 [6], followed by a 2012 outbreak of 230 cases reported especially in middle and high schools in the Jeollanam-do region [7]. Nevertheless, the Tdap vaccination rate in Korea is extremely low in both adults and women of fertile age, and awareness of the Tdap vaccine is also low [8]. Vaccination history should be used to determine whether citizens of countries with active childhood and adult vaccination programs such as the US and developed countries in Europe should be vaccinated. However, proactive Tdap vaccination could be considered for adults with uncertain primary vaccination history in countries without active childhood vaccination programs. In particular, in countries with large numbers of citizens residing in Korea, including China, Indonesia, Uzbekistan, and Mongolia, the DTP booster administered at 4-6 years of age does not contain pertussis [9]. The KSID recently revised its recommendations that pregnant women can be vaccinated with the Tdap vaccine [10]. However, the current incidence in Korea does not meet the level of evidence necessary for required vaccination with every pregnancy, as recommended by the Advisory Committee on Immunization Practices. Based on the benefits and safety of vaccination during pregnancy, a single vaccination is recommended before pregnancy for women planning a pregnancy; meanwhile, for those not vaccinated prior to pregnancy, the recommendation is to vaccinate at 27-36 weeks of pregnancy, identical to recommendations for the immigrant population.
2. Hepatitis A vaccine
<Recommendations for hepatitis A vaccination>
a. Vaccination is recommended for adults with no history of hepatitis A infection or vaccination.
b. Because hepatitis A antibody seroprevalence differs among different age groups and countries, antibody levels should be confirmed before vaccination.
c. The vaccine should be administered twice (second dose delivered 6-12 months after the first dose).
A. Evidence for recommendations
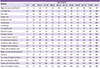
Approximately 1,400,000 individuals are infected with the hepatitis A virus annually, and the incidence is closely related to socioeconomic, health, and sanitation levels [11]. The disease mostly occurs in children in less developed countries, but the overall prevalence is low in countries with good sanitation. Because the rate of naturally acquired immunity in adults is low, sporadic outbreaks occur mostly in adults. The sanitary level in Korea improved considerably after the 1970s; after introduction of the vaccine in 1997, Korea has progressed toward becoming an epidemiologically low-risk region. Although there were 105 cases in 2001, the number increased significantly in 2006 to 1937. Most of the infected patients were in their 20s and 30s [11]. With active vaccination campaigns, the number of new patients reported each year is gradually decreasing, with 5,521, 1,197, and 867 in cases reported in 2011, 2012, and 2013, respectively [12]. However, vaccination is recommended in adults without immunity to reduce the risk of sporadic transmission in these individuals. The seroprevalence of hepatitis A antibody in adult foreigners differs according to country or origin and age group (Table 1). Generally, the seroprevalence of citizens of developed countries such as the US, Australia, and Western European countries is low, whereas that of citizens of less developed countries is high because of natural infection [13]. Therefore, the history of hepatitis A infection should be considered before vaccination. In some countries, the hepatitis A vaccine is included in the childhood vaccination schedule. For example, in China, which accounts for half of all foreigners residing in Korea, all children are vaccinated once at 18 months of age. However, countries such as the US, Japan, and Vietnam do not include the hepatitis A vaccine in their childhood vaccination schedules [14]. Because the situation is different for each country, it is recommended that IgG seropositivity against hepatitis A be assessed prior to vaccination, when possible.
3. Measles-mumps-rubella (MMR) vaccine
<Recommendations for MMR vaccination>
a. Adults for whom it is unclear whether two doses of the MMR vaccine were administered after the age of 12 months are targets for vaccination. In particular, vaccination is recommended for immigrant populations from less developed and developing countries in Africa, the Middle East, and Asia.
b. One dose of the MMR vaccine is recommended. However, healthcare providers should be vaccinated twice, with an interval of at least 1 month between vaccinations.
c. Although antibody levels could be checked prior to vaccination, it is not recommended from a standpoint of cost-effectiveness.
d. When vaccination is considered to prevent rubella in women of fertile age, it is recommended to check for rubella antibody levels. If seronegative, one dose of the MMR vaccine should be administered (contraception should be used for 4 weeks following vaccination).
A. Evidence for recommendations
Since 2001, children entering school in Korea have been required to submit a vaccination certificate confirming administration of the second dose of the MMR vaccine. Since 2006, measles has been managed at an eradication level [15], and in 2014, the World Health Organization recognized that Korea had eradicated measles. However, a measles outbreak in East Asian countries such as the Philippines and Vietnam in 2014 resulted in an increased number of imported measles cases in Korea as a result of secondary spread in schools. Several countries are currently conducting vaccination projects to eradicate measles, aiming for a completion rate exceeding 95% for the two-dose MMR vaccination. However, actual vaccination rates vary significantly among different regions. In daveloped countries in Europe, Asia, and the Americas, two doses of the MMR vaccine are recommended, and the vaccination rate is relatively high [16]. However, although MMR vaccination is performed in less developed and developing countries in the Middle East and Asia, administration of two doses of the MMR vaccine is uncommon. The majority of countries in Africa use a measles vaccine instead of the MMR to vaccinate children once at 9 months of age, and the vaccination rate is considered low [1718]. Accordingly, the number of doses of the MMR vaccine should be checked; when it is not clear whether individuals have received two doses of the vaccine, an additional dose of the MMR vaccine is believed to be effective, with reference to the circumstances in each country and region. It is important to test for rubella antibody before pregnancy in women of reproductive age; if the woman is seronegative, a single dose of the MMR vaccine should be given to prevent rubella.
4. Varicella vaccine
<Recommendations for varicella vaccination>
a. Excluding individuals with a vaccination certificate that confirms vaccination against varicella, individuals with a history of varicella infection, and individuals seropositive for varicella antibodies, all others are assumed to have no immunity against varicella.
b. Vaccination candidates should be selected according to criteria from the KSID adult vaccination recommendation.
c. Because many individuals have varicella antibodies, even in the absence of a known history of varicella infection, vaccination can be performed after performing an antibody test to identify seropositive individuals. The vaccine is given in two doses with a 4-8-weeks interval.
A. Evidence for recommendations
Compared to other vaccines, few countries worldwide regularly administer the varicella vaccine, likely because varicella infections at a young age are not generally accompanied by major complications. Nevertheless, in countries in which vaccination is not performed, varicella can become an additional burden on society and families because outbreaks at day-care facilities can require home treatment of infected children and temporary closure of facilities to control outbreaks. For this reason, approximately 15 countries worldwide, including Korea, recommend varicella vaccination as part of their national vaccination programs (Table 2). Currently, in countries in North America and Germany, administration of the second dose at 4-6 years of age is mandatory because of varicella outbreaks in school-aged children because of breakthrough infections. In Australia, the decision to administer a second dose to children is left up to parents, and there is an ongoing debate regarding whether the second dose should become mandatory in the future [19]. In Japan, vaccines included in the national vaccination programs are divided into required and optional. Because the varicella vaccine is classified as optional, the cost of vaccination is not supported by the government. The varicella vaccination rate in Japan is an estimated to be 20-40% based on vaccine shipment data [20].
It is recommended that foreigners residing in Korea should also be vaccinated based on their age and immunity at the time of immigration. It is appropriate for foreigners in Korea to follow the same schedule as Korean children and receive vaccinations at 12-15 months of age, whereas older individuals should receive catch-up vaccinations. Because childhood varicella vaccination rates and seroprevalence differ by country, it is recommended that foreigners residing domestically be tested for varicella antibodies prior to vaccination.
5. Japanese encephalitis vaccine
<Recommendations for Japanese encephalitis vaccination>
a. Among foreigners without immunity, vaccination is recommended in the peak season (August-November) for the following groups:
- Individuals expecting to stay in the country longer than 1 month
- Individuals expecting to stay in the country less than 1 month but who are planning a trip to high-risk areas
b. Vaccination methods
- Inactivated mouse brain-derived vaccine: three doses of subcutaneous injections at 0, 7, and 30 days; a booster after 2-3 years should be considered for cases of continuous exposure
- Inactivated cell culture vaccine: administer two doses at 0 and 28 days and a booster after 1 year
- Attenuated live vaccine: not recommended as there are no studies in adults
A. Evidence for recommendations
The risk of Japanese encephalitis is generally low when people residing in non-endemic regions travel to endemic areas; the risk of infection for travelers to Asia is less than 1 in 1,000,000. Between 1973 and 2008, a total of 55 patients reportedly contracted Japanese encephalitis while travelling [2122]. The main countries in which infection occurred were Thailand, Indonesia, China, and the Philippines, and there are no cases of infection in foreigners in Korea after travel. However, between 2000 and 2012, 82 cases of Japanese encephalitis were reported in Korea [23]. As foreigners travelling to endemic regions have a similar risk as Korean residents, vaccination is recommended. Among patients who contract Japanese encephalitis after visiting an endemic area, 65% stayed for more than 1 month; when the duration of travel was short, 80% were infected outside of urban regions [24]. Based on this finding, the recommendations state that individuals staying in Korea longer than 1 month, as well as those staying for less than 1 month but who are planning a trip outside of urban areas, should undergo vaccination. The majority of cases of Japanese encephalitis occur between August and November in Korea, and it is recommended to undergo vaccination during this period [24].
Japanese encephalitis vaccination is mandatory among the following countries with Japanese encephalitis: South Korea, Japan, China, Taiwan, Hong Kong, and Thailand [924]. Vaccination is recommended for foreigners entering Korea from countries without Japanese encephalitis and for citizens of countries with mandatory vaccination policies without vaccine immunity who satisfy the criteria of the recommendations.
B. Consideration prior to vaccination
Only inactivated vaccines may be administered to adults, and there are three types of inactivated vaccines used globally (mouse brain-derived, hamster kidney-derived, and Vero cell-derived). Two inactivated vaccines are currently used in Korea: the mouse brain-derived Nakayama strain and the Vero cell-derived Beijing strain. However, in Western countries, including the US, only the inactivated Vero cell-derived SA 14-14-2 strain vaccine is used. Therefore, for foreigners with vaccine-based immunity to Japanese encephalitis who want a booster vaccination, the type of vaccine previously administered must be confirmed. An experimental study illustrated that a single booster dose with the inactivated Vero cell-derived SA 14-14-2 strain can increase immunity to Japanese encephalitis in adults who have completed primary vaccination with the inactivated mouse brain-derived Nakayama strain [25]. However, because there is no data on immunological reactions or adverse effects between other Japanese encephalitis vaccines, further studies are necessary.
6. Summary
In Western countries, imported infectious diseases occur more frequently among foreigners visiting friends or relatives than in general travelers [26]. Therefore, vaccination of the immigrant population is important for individual health, as well as for the national management of infectious diseases. The number of foreigners entering and staying in Korea has been continually increasing, and the nationalities of immigrants are also becoming more diverse. Because their immunity to various infectious diseases may differ from that of the general Korean population, separate vaccination recommendations need to be developed on the basis of their age, nationality, and medical history. To develop applicable vaccination recommendations for individual countries or regions, data on disease statistics, childhood vaccination policies, vaccination rates, and vaccine-related seroprevalence in each country are required. However, apart from advanced countries, these data are available for extremely few countries. Nevertheless, because there were similarities between vaccination policies and population seroprevalence for various pathogenic organisms according to national economic status and country or region, vaccination recommendations were categorized at the continent level (Table 3). In the future, to develop more precise vaccination recommendations, there is a need for epidemiological studies and public health statistical data on foreigners residing in Korea as well as analysis of data from additional foreign countries.



 XML Download
XML Download