

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Wiskott-Aldrich syndrome (WAS) (Online Mendelian Inheritance in Man [OMIM] 301000) is an X-linked recessive disorder characterized by thrombocytopenia, eczema, and immunodeficiency. Clinical symptoms include petechiae, bloody diarrhea, inability to generate antibodies against polysaccharide antigens, and in some cases, autoimmune manifestations. Affected boys often die because of malignant tumors, particularly lymphoma (1, 2). Treatments for WAS include antimicrobial therapy for infections, intravenous immune globulin, splenectomy for thrombocytopenia, and allogeneic bone marrow transplantation (3-5).
The gene responsible for WAS was isolated, and designated the WAS gene (6). The gene is composed of 12 exons spanning approximately 9 kilobases. The encoded protein is a 502 amino-acid long intracellular protein, which is broadly expressed in hematopoietic cells (7). The WAS gene was found to be mutated, not only in classic WAS patients, but also in patients with X-linked thrombocytopenia (XLT), which is a clinically mild allelic variant (8, 9). Recent reports have expanded the WAS mutation phenotype to include intermittent XLT, X-linked neutropenia with or without myelodysplasia, or WAS/XLT in females with heterozygous mutations (10, 11).
Many WAS gene mutations have been reported in patients with WAS. However, little is known about Korean WAS patients in terms of their molecular genetic diagnosis. In this report, we describe a Korean family with WAS, which was diagnosed as having exon 2 mutation, based on the WAS gene mutation analysis. This is the first identified case of a hotspot mutation in exon 2 of WAS in Korea.
MATERIALS AND METHODS
Subjects
A one-day-old male neonate was admitted to the hospital because of jaundice and petechiae on the body. He was born after 37 weeks gestation, by Cesarean section due to breech presentation and had a birth weight of 2,800 g. Laboratory data showed a hemoglobin of 16.8 g/dL, a white blood cell count of 17,050/µL, a platelet count of 39,000/µL, and a high reticulocyte count (9.1%), but Coombs' tests were negative. The level of serum bilirubin (total/direct) was 7.3/0.4 mg/dL, and the result of the liver function test was unremarkable. Also, immunoglobulin (Ig) M titers to TORCH were negative. Serum Ig measurements at day 1 revealed an elevated Ig A level (28.8 mg/dL; normal range, 1.3-3.6) (Ig G: 1,216.8, Ig M<23.8, Ig D<1.5, and Ig E<18.0). The results of peripheral blood smear were unremarkable, except for a markedly decreased number of platelets. A bone marrow aspiration smear showed slight erythroid and megakaryocytic hypoplasia. Karyotyping analyses of both the patient and his mother were normal. A review of family history revealed his maternal uncle was clinically diagnosed as having WAS at five years of age. The patient was treated with platelet transfusion, and petechiae on the body disappeared immediately. However, the patient's thrombocytopenia persisted. When the patient was 18 months old, genetic counseling was provided at his mother's request.
Mutation analysis
Genomic DNA was isolated from peripheral blood leukocytes by using the Wizard Genomic DNA purification kit, according to the manufacturer's instructions (Promega, Madison, WI, U.S.A.). In order to examine mutations on the WAS gene, polymerase chain reaction-single strand conformational polymorphism (PCR-SSCP) was performed for all 12 coding regions of the WAS gene by using the primer sets as listed in Table 1. The PCR was performed with a thermal cycler (model 2400, Applied Biosystems, Foster City, CA, U.S.A.) as follows: 32 cycles of 1 min at 94℃ for denaturation, 1 min at 55-60℃ for annealing depending on the primers, and 1 min at 72℃ for extension. Final extension was performed at 72℃ for 10 min. The PCR products were electrophoresed on an agarose gel and stained with ethidium bromide to confirm the size of the bands. The PCR products were also denatured in formamide loading buffer and electrophoresed through 8% and 10% polyacrylamide gels. Silver stain was performed to develop bands (12). To determine the sequences of the DNA samples showing mutant bands, direct sequencing was performed on the ABI Prism 3100 Genetic Analyser (Applied Biosystems).
RESULTS
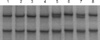
PCR and subsequent SSCP analysis in exon 2 of the WAS gene identified an aberrantly migrating band in the patient's mother, and in his maternal grandmother, compared to two wild type bands in the controls. The patient and his maternal uncle showed two bands, one of which was a lower wild single strand band and the other, an abnormal shifted band (Fig. 1). In the direct sequencing analysis of the PCR products for SSCP, the missense mutation was observed in the patient and his maternal uncle. This showed G-to-A transition at complementary nucleotide 257 (c.257G>A) (Fig. 2C), resulting in substitution of His for Arg at codon 86 (Arg86-His) (CGC→CAC). The patient's mother and his maternal grandmother were heterozygous for the mutation at codon 86 (Fig. 2B).
DISCUSSION
Mutations of the WAS gene result in 3 distinct phenotypes: the classic WAS triad of thrombocytopenia with small platelets, recurrent infections as a result of immunodeficiency, and eczema (1); the milder XLT variant, characterized predominantly by thromobocytopenia with small platelets (8, 9); and finally, congenital neutropenia without the clinical findings characteristic for WAS/XLT (10, 11).
As shown in WASPbase (13), a database of mutations, a total of 441 cases consisted of missense mutations in 179 cases (40.6%), deletions in 92 cases (20.9%), nonsense mutations in 64 cases (14.5%), splicing defects in 64 cases (14.5%), and insertions in 42 cases (9.5%). The exon distribution of over 5% frequency of mutation was located in exon 2 (27.0%), exon 10 (16.1%), exon 1 (13.8%), exon 4 (9.8%), exon 3 (7.5%), and exon 7 (6.4%). Notably, the frequency at codon 86 in exon 2 was 33.6% (40/119 cases). It is well known that the codon 86 of the WAS gene is the most common missense mutation site responsible for WAS/XLT (10, 13). To our knowledge, this is the first report on the hotspot missense mutation in exon 2 of WAS gene in Korea.
There are several reports on WAS mutations in Korean families (Table 2). As shown in Table 2, the predominant mutations were nonsense mutations and missense mutations (14-18). Only one small deletion was reported in exon 10 (15). In this report, we found a missense mutation in exon 2. In Korean patients' reports, including our results, mutations in exon 1, 2, 3, 7, 8, and 10 have been involved in WAS. Therefore, although it is necessary to accumulate mutation data from a large number of patients with WAS, the distribution of mutations may be highly diverse in Korean patients, as had been observed in other reports (9, 10, 13).
A correlation between clinical phenotype and genotype was reported independently by several investigators (19-21), but was not observed by all (22, 23). Imai et al. demonstrated that all WAS patients with missense mutations showed WASP-positive expression; in contrast, patients with nonsense mutations, large deletions, small deletions, and small insertions were WASP-negative expression. Patients with splicing mutations were either WASP-negative or WASP-positive. Lack of WASP expression was associated with severe clinical symptoms and poor prognosis (24). Jin et al. reported 5 mutational hotspots in the WAS gene from 227 WAS/XLT families with a total of 262 affected members. They also noted that the missense mutation at codon 86 was observed most frequently and associated with mild symptoms (25). Two previous reports (24, 25) showed that there is a strong possibility of establishing an association between genotype and phenotype. In spite of advances in the clinical treatment of WAS patients, WAS remains a life-threatening condition, resulting in a poor quality of life and a bad long-term prognosis, especially for those who lack an HLA-matched sibling. The discovery of the WAS gene, and the identification of the molecular basis of WAS, have made it possible to provide genetic counseling for at-risk families. Therefore, this report on the hotspot missense mutation in exon 2 of WAS gene, will help this patient's parent and his maternal uncle to understand WAS and plan both genetic counseling and family regulation.



 XML Download
XML Download