

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Extramedullary hematopoiesis (EMH) is occasionally reported in idiopathic myelofibrosis and is generally found in the liver, spleen, and lymph nodes (1). Involvement of other sites, such as the intrathoracic cavity, kidney, and thyroid, has been reported (1, 2). However, involvement of the dura mater of the spinal cord, resulting in spinal cord compression, has rarely been described between two and 20 yr after diagnosis of myelofibrosis (2-6), and myelofibrosis presenting as spinal cord compression, resulting from EMH tissue, is also very rare (7). We report the first case of EMH due to chronic idiopathic myelofibrosis in the lumbar spinal canal in Korea and present the surgical outcome.
CASE REPORT
A 39-yr-old man presented with back pain, subjective weakness and numbness in both legs that had progressed over 2 weeks. His medical history was not significant except that he received anti-tuberculosis medication at the age of 12 yr for pulmonary tuberculosis. There was no history of trauma or primary malignancy.
On physical examination, his blood pressure was 110/70 mm Hg, pulse 94 beats per minutes, and respiratory rate was 18 breaths per minute. There was no pallor or jaundice, nor clinically palpable hepatosplenomegaly. His neurological status was unremarkable except for paresthesia at bilateral L5 and S1 sensory dermatomes and decreased deep tendon reflexes on ankle. He had normal mental function and no abnormality of the cranial nerves. Laboratory workup showed a normal hemoglobin level of 16.9 g/dL (range, 13-17 g/dL), mean corpuscular volume of 83.5 fL (range, 95-105 fL), mean corpuscular hemoglobin of 28.6 pg (range, 25-35 pg), hyperleukocytosis of 23,800/µL (range, 4,000-10,000 g/L), and platelet count 111,000/µL without any other abnormal findings. Liver and renal function tests were also normal.
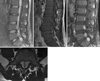
Chest and lumbar radiography was normal. Sagittal magnetic resonance imaging (MRI) showed multiple anterior epidural mass extending from L4 to S1 with compression of the thecal sac and nerve root (Fig. 1A-C). Axial images revealed an extradural mass extending into the neural foramen bilaterally (Fig. 1D), which gave slightly high signal on T2-weighted images; isointense on T1-weighted images and enhanced strongly with gadolinium. The mass seemed encapsulated and showed no invasion or communication with neuronal structures.
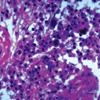
For neurological resuscitation and histological confirmation, the patient underwent decompressive surgery via L4, 5 and S1 total laminectomy and gross total removal of the epidural masses which located in the ventral portion of thecal sac. The intraoperative finding included several round and lobulated reddish tumors that was partially adherent to the ventral dura mater (Fig. 2). Four masses were removed in total. Two were removed from both sides of L5 vertebra and two from the right side of L4 and S1 vertebra. Each mass was independent from each other without connection or adhesion. Histological analysis showed islands of myelopoietic cells surrounded by fatty tissue, consistent with EMH (Fig. 3). Bone marrow aspiration and biopsy performed after surgery revealed hypercellular marrow and megakaryocytic hyperplasia and focal fibrosis. The final diagnosis was chronic idiopathic myelofibrosis (agnogenic myeloid metaplasia) leading to EMH on lumbar spinal canal.
Postoperatively, there was marked improvement of neurological symptom within a few days. Since there was no abnormal hematological finding except mild myelofibrosis, additional treatment such as radiothepary was not administered in consideration of radiotoxicity. On 6-month follow-up examination, the patient remained clinically stable and the MR imaging studies demonstrated no disease recurrence in the epidural space.
DISCUSSION
EMH is usually seen as a reactive process in various hematological diseases, with the liver and spleen as primary manifestation sites (1, 8-14). Rarely, EMH has been found localized in dura matter of spinal cord, and can result in spinal cord compression (2-14). EMH causing spinal cord compression was first reported in 1956 by Close et al. in a patient with thalassemia minor (8). Although this most often occurs in thalassemia, it has also been described in myeloproliferative diseases such as polycythemia vera, sideroblastic anemia, pyruvate kinase deficiency, and myelofibrosis disorders (8-14). In our patient, unusually, there was no predisposing hematological disorder at presentation, and the diagnosis of EMH and idiopathic myelofibrosis was made retrospectively. Another atypical feature was the relatively minor degree of splenomegaly at presentation. In case of myelofibrosis with EMH a far greater degree of splenomegaly would usually be expected (2-6, 8).
The exact origin of EMH in the dura mater is unknown. Some previous reports indicated the dura mater has a hematopoietic capacity in the fetus and EMH may develop from primitive rests (2, 3). However, it is unlikely that EMH arises from extrusion of vertebral bone marrow in the absence of bony erosion or fractures. Symptomatic spinal cord compression secondary to EMH shows a preference for localization in the middle and lower thoracic spine. Some authors related this to the narrow spinal diameter at this level (3, 5-14).
Radiologic features of intraspinal EMH are well defined especially on MR imaging. Some authors emphasized the use of MR imaging because of the notable isointense T1- and T2-weighted images secondary to the deposition of iron. The principal MR imaging characteristics of EMH include the followings: an extramedullary mass (more often in the posterior location of the epidural space and in the thoracic region), with homogeneous signal intensity on T1-weighted images, slightly higher intensity of signal than the adjacent red marrow of the vertebral bodies on T2-weighted images, and enhancement after Gadolinium injection (2, 5). However, the diagnosis can be confirmed by fine-needle aspiration cytology or open biopsy in case of unusual imaging findings or clinical history (1, 6, 11-14). The lesion is composed of various numbers of hematopoietic cells from all three hematologic cell lines.
Finally, management of patients with epidural EMH remains controversial, and there are no widely accepted treatment guidelines. Regarding the pathophysiology of the disease, low doses of radiotherapy or blood transfusion has been recommended as the initial treatment during the past two decades (3, 5, 6, 9). However, the risks of radiotherapy in the treatment of cord compression in such patients include the lack of any tissue for histological diagnosis and the risks involved in radiation exposure, and the transfusion also has a risk such as infectious disease, iron overload, formation of antibodies (10). Recently, hydroxyurea has been proposed as a complementary approach to increase the efficiency of erythropoiesis and reduce the volume of transfusion required (7). These non-surgical approaches can be undertaken in patients in whom the diagnosis of EMH is highly expected, based on clinical presentation, known chronic anemia, and MR imaging features. Although they can avoid surgery-related complications such as the high risk of bleeding due to the lesion's vascularity or difficulty in transfusion due to antibodies and cardiopulmonary stress, disadvantages are they do not allow definitive diagnosis and have a high rate of recurrence. In cases of symptomatic spinal cord compression, surgical decompression and subsequent low-dose radiotherapy have been recommended (2, 11-14). Decompessive surgery is immediately effective in most cases and radiotherapy is introduced as an adjunct to surgery because of prevention of recurrence, incomplete excision, or persisting neurological deficit. As an alternative option, radiation can be saved as a salvage procedure for recurrence, if complete removal was accomplished (10). We decid- ed to treat our patient with surgical removal without adjuvant therapy to prevent complication of adjuvant therapy, and the postoperative result was favorable during the 6-month follow-up period.
In conclusion, authors successfully treated a rare case of EMH on spinal canal with surgical management. Although medical treatment should be first advised after discussion with the hematologist, surgical approach may be successfully used in case of severe neurologic deficit, failure of medical treatment, or uncertain diagnosis.

 XML Download
XML Download