

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Low back pain (LBP) is the second most common cause of hospital visits (1). With a globally aging population, the incidence of low back and leg pain, especially attributable to degenerative causes including lumbar zygapophyseal joint (LZJ) and sacroiliac joint (SIJ) arthopathies, is rapidly increasing (2). However, it is often difficult to define the source of pain. Only about 12% of cases with LBP can be given a specific pathoanatomical diagnosis using modern diagnostic techniques (3), and the remainder of patients are often grouped in vague terms such as lumbago, low back strain, mechanical low back pain, etc. Traditionally, the diagnosis of low back pain depends primarily upon the clinical examination and neuroimaging findings (4-6). These diagnostic methods can provide confirmatory information on the source of pain if neurological deficits are evident, so that appropriate treatment can be chosen with good outcome. However, most patients with LZJ and SIJ arthropathy pain have referred somatic pain, in which neurological symptoms and signs are not so apparent. Subsequently, it is difficult to make definite diagnosis in these disease entities (7-9).
Traditional dilemmas in diagnosing spinal disorders were much resolved by the advent of high-resolution neuroimaging including magnetic resonance imaging (MRI) and computerized tomography (CT). These imaging modalities are excellent in demonstrating structural abnormalities of the spine and neighboring structures, thus make it easier to reach a confirmatory diagnosis in the selected cases of herniated lumbar disc that are correlated with patients' neurological symptoms and signs (6, 10). However, these conventional diagnostic approaches are currently being challenged, with an evolving body of evidence demonstrating that asymptomatic volunteers have a high incidence rate of disk herniation or extrusion (5, 11). Furthermore, CT findings have been proven to have no value as a diagnostic test for LZJ arthropathy, as well as for SIJ arthro- pathy (12, 13). Therefore, other new methods to make decisions in patients with spinal pain, especially somatic referred pain, are now in higher demand.
In somatic referred pain, clinical histories and physical examinations present unreliable features. Several criteria have been proposed to substantiate the diagnosis or to predict pain relief after nerve blocks, yet they are not sufficient to provide clinicians with a roadmap for these syndromes. We previously developed the pain distribution pattern template (PDPT) as a guide for clinical decision-making in patients with LBP and leg pain (7, 14). In the present paper, we evaluated the correlation between PDPT and diagnostic nerve blocks in patients with LZJ or SIJ arthropathies to determine the diagnostic accuracy of PDPT and its usefulness as an initial guide in the management of LBP.
MATERIALS AND METHODS
Development of pain distribution pattern templates
Drawings of pain distribution patterns were collected from a pool of 200 patients with spinal disorders with confirmed diagnoses. The spinal disorders included in the study consisted of LZJ pain and SIJ arthropathy. The drawings were analyzed to harvest the most frequently presented patterns and the pain distribution patterns of each spinal disorder were classified.
LZJ pain patterns were classified into five types of pain patterns (Fig. 1): Type A shows the pain distribution in the paravertebral area, localized or band-like extension. Type B combines Type A with leg pain in the posterior thigh and calf. Type C combines Type A with leg pain in the posterior thigh only. Type D combines Type A with leg pain confined to calf only. Type E indicates pain that has components of referred pain similar to above types but also shows mixed pain patterns of other spinal disorders or is otherwise difficult to fit into the above types.
SIJ pain patterns were also classified into five types (Fig. 2): Type A shows pain distribution in the lower back, gluteal region, and lateral aspect of the thigh; type B is similar to type A, with the addition of groin pain; type C has pain in the lower back and posterior aspects of the gluteal region. Type D combines type C and groin pain. Type E indicates pain that has components of referred pain similar to the above types and mixed pain patterns of other spinal disorders or is otherwise difficult to fit into the above types.
Patient population
Between October 2003 and October 2004, a total of 419 patients were confirmed to have LZJ or SIJ arthropathy by comparative nerve blocks or radiofrequency (RF) neurotomies in our institution. Before the procedures, all the patients had pain lasting more than 3 months and pain intensity greater than 5 on the numerical rating scale (NRS). Thorough clinical and neurological examinations and simple radiography were performed routinely. MRI and CT examinations were performed in the selected cases mostly to rule out disk herniations if patients presented clinical signs or pain patterns of disk herniations. All patients were interviewed by a pain-specialist nurse, who recorded the pain distribution pattern, nature of pain, pain-related dynamic factors, and factors influencing life pattern and daily activities. Excluded were patients who presented evidence of lumbosacral radiculopathy with signs of myotomal weakness, sensory disturbances, or loss of reflexes. Even if signs of radiculopathy were absent, patients were excluded if they demonstrated midline back pain and/or radicular pain. Patients who had collagen, vascular, or rheumatologic diseases were also excluded.
Classification of pain distribution patterns
PDPT was presented to the patients during the course of interview to indicate their own pain patterns. In addition, detailed drawings were obtained from all the patients. If patients were not confident about their pain types, only drawings were selected to determine their own pain patterns. These drawings were presented to three other observers (HIK, DGS, and DAS), blind to the patients' detailed history, to harvest the pain patterns presumed to arise from LZJ and SIJ. Pain patterns were again classified depending on the location of joints involved. Further diagnostic procedures were decided in weekly spinal pain conference. Pain patterns were divided into type A, B, C, D, or E in the patients presumed to have LZJ arthropathy and type A, B, C, D, or E in SIJ arthropathy.
Comparative nerve blocks and RF neurotomies
All the patients underwent diagnostic nerve blocks to confirm the presumptive diagnosis based on the pain distribution patterns. To minimize the false positive rate, diagnostic blocks were performed more than twice for all patients who showed a positive response on the first block. All the procedures were performed in the operating room under a C-arm intensifier. Medial branches of L2, L3, L4, and L5 dorsal ramus were chosen over 2-3 levels depending on the pain patterns in the patients with LZJ arthropathy. Targeted nerves were blocked with 0.5 cc of either 0.5% bupivacaine or 4% lidocaine. For sacroiliac joint arthropathy, the intraarticular joint capsule or deep interosseous ligament (DIOL) was blocked in the same manner. After blocks, patients were instructed to indicate the change of their usual pain every 30 min for 3 days as complete relief, nearly complete relief, 50% reduction of pain, slight reduction of pain, or no change. If the patients' pain relief persisted, other additional procedures were not planned. However, if patients continued to have pain, RF neurotomies were performed for medial branches in LZJ arthropathy and lateral sacral branches in SIJ arthropathy. Sensory stimulation was used to select the "pathological branches" for RF coagulation among the branches that showed the positive responses to nerve blocks in a group. If the pain response by sensory stimulation was the same as that of the usual pain with lower than 0.6 V amplitude, a cannula was maintained for RF coagulation of the branches. Radiofrequency lesioning was made on the targeted nerve branches at 80℃ for 90 sec. Multiple lesions were produced for every branch; meanwhile, a single lesion was produced for the L5 dorsal ramus.
Evaluation of outcome
Numerical rating scores for pain were checked before and after each procedure as part of a baseline questionnaire administered in all patients. The reliability of the PDPT-based diagnosis was determined by either of two criteria. Firstly, patients' pain was markedly improved by single block and further treatment was not required for more than three months, or secondly, if the patients demonstrated concordant pain relief better than "50% of pain reduction" on double comparative blocks. If either of these criteria was fulfilled, the PDPT-based diagnosis was considered to be correct. Similarly, if patients had more than 50% pain reduction following RF neurotomies, the diagnosis in those patients was also considered to be correct. For analysis of treatment outcomes, patients who showed more than 50% pain reduction following RF neurotomies or comparative nerve blocks were included in the favorable outcome group.
Statistical analysis
The statistical analysis was performed using SPSS 12.0 (SPSS, Chicago, IL, U.S.A.). Relationships between pain patterns and multiple data of nerve blocks were analyzed using two-way ANOVA. Pain patterns, nerve block data, and treatment outcome were evaluated using a chi-square test. All differences were regarded as significant if p<0.05. A Z-value was calculated to determine the diagnostic reliability and treatment outcome. Z-values higher than 95% were regarded as significant.
RESULTS
Demographic data
The study population consisted of 103 males and 156 females with LZJ arthropathy, with a mean age of 62.04±12.01 yr, and 47 males and 113 females with SIJ arthropathy with a mean age of 61.43±11.18 yr. In the patients with LZJ arthropathy, the mean value of pain severity before treatment was 6.1 on NRS. This was reduced to 3.4 during the course of nerve blocks. In SIJ arthropathy, the mean NRS was 6.4, which was decreased to 3.5 after nerve blocks.
Diagnostic reliability of pain distribution patterns in LZJ arthropathy
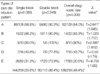
Diagnostic reliability of PDPT-based diagnosis in LZJ arthropathy is summarized in Table 1. Overall, 49% of patients showed a positive response to nerve blocks. Patients with Type A and C patterns showed a significantly positive response. The diagnostic rate was higher in Type C; however, the reliability was better in Type A. Type B, D, and E patterns failed to show significant rates of diagnosis. Single nerve blocks showed a diagnostic rate of 55.6%, which was increased to 86.4% on second comparative blocks because patients who showed a false positive response were excluded by the second block.
Diagnostic reliability of pain distribution patterns in SIJ arthropathy
Diagnostic reliability of pain distribution patterns in SIJ arthropathy is summarized in Table 2. Forty-six percent of patients with SIJ arthropathy could be diagnosed based on pain distribution patterns. The type C pattern showed a significant positive response and reliability for PDPT-based diagnosis. Diagnostic rates of type A and B were high, yet they were not statistically significant. Results of single nerve blocks showed a 54.4% diagnostic rate, which was increased to 78.8% on second comparative blocks because the patients who showed the false positive response on first block were dropped out. However, the validity of diagnostic rate of second block depending on pain patterns was not statistically significant.
Treatment outcomes and pain patterns
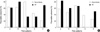
Analysis of treatment outcome in LZJ arthropathy showed no statistical difference between nerve blocks and RF procedures in Type A B, C, or D (Fig. 3A). This result indicated that patients with favorable outcome in nerve blocks were likely to have a similar result following RF procedure. However, Type C showed more favorable response from nerve blocks compared with that of RF procedure. Patients in Type E showed significantly better results from the RF procedure, despite lower rates of favorable outcome in nerve block. In the patients with SIJ arthropathy, there was no statistical difference between nerve blocks and RF procedures in Type A, B, or C. Type D did not have RF cases. Patients with type E showed similar results as in LZJ arthropathy although they could not demonstrate a statistical significance (Fig. 3B).
DISCUSSION
Pain complaints are not extensively employed in the diagnosis of LBP, for subjective complaints can vary depending on the patients' pain tolerance (15, 16). However, pain complaints contain invaluable information to indicate the source of pain (17, 18). Most patients with degenerative joint arthropathy lack objective symptoms or signs, which are often presented in the patients with disk herniations (4, 19). Therefore, it is logical to make use of pain complaints to find a clue to the diagnosis of spinal disorders. Typical pain patterns for LBP are shown in the literature, yet they do not encompass the diversity of the pain distribution patterns for each spinal disease entity (20-22). Pain patterns often overlap among the variety of spinal diseases, thus confounding the correlation between the pain pattern and the presumed diagnosis. The present study provides evidence that PDPT can be a quick guide to follow during diagnosis and treatment of somatic referred pain presenting LBP and leg pain. Our PDPT, developed from the analysis of drawings from each spinal disease, classifies the diverse pain distribution patterns into specific spinal disorders. Once presented to the patients, they can easily recognize the patterns that are similar to the pains they are suffering from. These pain patterns are directly linked to the presumed diagnosis; consequently, they can facilitate deciding the 'next step' in the course of diagnostic procedures.
Recent investigations have highlighted the importance of LZJ and SIJ arthropathy, of which the prevalences are around 39% and 15-30%, respectively, among patients with chronic LBP (23, 24). Although the diagnostic rate of PDPT is not high compared with that of MRI in intervertebral disk disease, it can provide useful information in decision-making in patients whose pain is assumed to emanate from the LZJ and SIJ. In our study, the diagnostic accuracy of PDPT was 49% for LZJ and 46% for SIJ pain. Considering the diagnostic accuracy of MRI in the intervertebral disk disease is 78.3%, the diagnostic accuracy of PDPT may not be a competitive tool (5). However, Boos et al. pointed out that explanation of LBP and sciatica by MRI is questionable even in disk herniations despite its high diagnostic rate, since pathoanatomical alterations may not be directly related with the source of pain (4, 5). Furthermore, MRI or CT is not helpful to determine pain source in patients with somatic referred pain arising from the LZJ and SIJ (12, 25, 26). Considering the paucity of diagnostic maneuvers for somatic referred pain, PDPT is regarded to be uniquely useful in this situation.
No clear explanation exists for the diversity of pain patterns in LZJ or SIJ arthropathy. It is interesting to note that thoracic zygapophyseal joints are intrinsically smaller and hold less volume than lumbosacral joints. Consequently, more localized pain patterns are presented closer to the pain source (27). On the contrary, in the lumbosacral spine, referral can be extended into the thigh and leg with joint injection (28). Therefore, referral pain of lumbosacral joints is related to more diffuse patterns, distant to the origin of pain source. Another consideration is the interpersonal difference of nociceptive density responsible for transmitting painful response. There are a variety of intra-articular structures in the lumbar LZJ and SIJs, and sensory fibers innervating them have a diverse course, producing different nociceptive density in each individual (29). Coupled with the morphological differences between individuals, these situations result in diverse pain patterns even if the same joint is involved (30). PDPT encompasses the diverse pain patterns, which can arise from the LZJ and SIJ not to be misled or confused by the diversity of pain.
In a clinical setting, pain drawing has traditionally been used in the evaluation of the patients with LBP in a number of ways, including correlation with the results of psychological evaluation, documentation of symptom location, diagnosis of lumbar disk disease, evaluation of changes in pain, and prediction of treatment outcome (15, 21). Although pain drawing has advantages in the quantitative evaluation of the severity and body region of pain, it was not specifically designed for diagnosis of various spinal diseases (15, 16). Consequently, interpretation of pain drawings cannot be accurately related to the diagnosis of spinal disease. On the other hand, PDPT is mainly designed to provide disease-specific pain distribution patterns without quantitative scoring or evaluation. Therefore, the numerical rating score for pain or other measures for psychological factors are additionally required.
We found that PDPT combined with careful measurement of pain distributional area was useful in assessing treatment outcome. If patients showed typical pain patterns, they generally had favorable outcomes to nerve blocks and RF procedures. However, if the pain pattern was ambiguous, there was no correlation between nerve blocks and RF procedures. This finding indicates that PDPT-based diagnosis can be used to predict treatment outcome. In addition, patients who showed a favorable outcome following treatment usually showed a reduction of area or loss of a part in pain distribution. Interestingly, since patients have a tendency to emphasize the remaining pain, true effects of treatment can often be masked and regarded as failure. Careful analysis of the pain distribution patterns can reveal the treatment effects qualitatively by observing complete or partial reduction of pain as well as remaining pain. Sometimes different patterns of pain distribution, which indicate the different sources of pain, can be mistaken as treatment failure. Therefore, patients should be followed up not only quantitatively but also qualitatively to determine the treatment effect in the management of patients with LBP and leg pain.
One limitation of the present study is that final diagnosis was not based on 100% pain reduction on comparative blocks or total loss of pain following RF procedures. More than 50% pain reduction in nerve block may not be sufficient to be a criterion for final diagnosis. Generally our patients seemed to be more reluctant than expected to give favorable results, and one hundred percent pain reduction was never expressed. So we assumed more than 50% of pain reduction in comparative blocks were likely to be a relatively solid basis as a standard of final diagnosis. In addition, comparative nerve blocks used in this study are very likely to exclude the false positive response in this setting.
In conclusion, PDPT is designed to encompass the diversity of pain patterns arising from LZJ and SIJs. PDPT-based diagnosis can provide a quick and useful guide in clinical decision-making for the management of somatic referred pain in lumbosacral disease. Furthermore, it can be used as a tool to predict the treatment outcome as well as to follow the change of pain patterns.



 XML Download
XML Download