

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The difficulty in falling asleep is the most classic sleep complaint, which is often equated with the concept of insomnia. Trouble falling asleep is a common complaint heard by clinicians. Nevertheless, the meaning of this complaint may be quite variable and complex. It has not been determined whether a certain sleep latency (time to fall asleep) marks a threshold between normal and abnormal.
Self-reported sleep latency (SRSL), the reported time in falling asleep, may be determined by several biological and psychosocial factors. Sleep onset time may be influenced by biological factors determining sleep propensity and by subjective preference or psychosocial factors for determining the sleep onset time. One hypothesis to describe sleep propensity is the interaction of homeostatic processes termed 'process S' and circadian process termed 'process C' (1). Process S mediates the rise of sleep propensity that increases progressively during wakefulness or sleep deprivation and decreases progressively during (non-REM) sleep. Process C represents a clock-like process underlying a (nearly) 24-hr oscillatory variation in the propensity of sleep, which is basically independent of prior sleep and waking. Thus, sleep propensity associated with SRSL can be affected by biological aspects of both process S and process C. The preferred sleep onset time can be affected by psychosocial factors such as work, school, exercise, and lifestyle. A longer or shorter SRSL may cause the discrepancy between the sleep onset time influenced by sleep biological propensity and the sleep onset time that psychosocial factors might promote. Sleep state misperception such as overestimation of SRSL compared to objective sleep latency may affect this discrepancy (2).
In this study, we focused on SRSL in a large group of postmenopausal women. The prevalence of insomnia with a longer SRSL sharply increases in women around the age of menopause (3-5). In postmenopausal women, complaints of trouble falling asleep are frequent, although complaints of mid-sleep awakenings and early awakening are even more prevalent (6). Specific aims of these analyses were to evaluate how SRSL is affected by sleep habits, mood states, depressive or primary sleep disorders, and circadian phase.
MATERIALS AND METHODS
Subjects
A group of 459 women who had volunteered for the Observational Study of the Women's Health Initiative (WHI) (7) at the San Diego Clinical Center further volunteered for an ancillary study of sleep. All subjects were relatively healthy women, living independently in the community. Women aged 50 to 81 yr with a life expectancy of 3 yr or more were eligible; subjects were not excluded because of medications or most illnesses. A group of 384 women who completed at least 6 days of both of sleep log and actigraphic data were selected from the larger group for analysis. Other results from this study have been reported elsewhere (8-11). This study was approved by the Institutional Review Board of the University of California San Diego. Each woman gave written informed consent to participate.
Subjects completed sleep questionnaires, underwent one-week wrist actigraph recordings at home, and collected fractional urine specimens over two 24-hr intervals. Information on the body mass index (BMI) and systolic and diastolic blood pressure was obtained from baseline measurements taken upon enrollment in the WHI. Blood pressure was calculated from the mean of two blood pressures in the resting state. Psychiatric diagnoses were made by a single observer within 1-3 weeks after each subject had completed her wrist actigraphic recording.
Questionnaires and psychiatric interview
The WHI insomnia rating scale (12, 13), Burnam mood screening scale (14), a hot flash rating log (7), a medication history, and daily sleep logs during actigraphic recording were completed. The sleep habit questionnaire was composed of 10 items, and the national distributions of responses to this questionnaire were described by Kripke et al. (6). Levine (13) showed that there was a principal insomnia factor in WHI insomnia rating scale consisting of 5 items of these 10 questionnaire items, which was named by Levine's factor. Levine's factor or insomnia factor was used by the insomnia scale in this study. The Burnam mood screening scale was calculated according to the Burnam-Rand depression P index (14, 15). The hot flash rating log was the number of reported total episodes during the actigraphic recording for 7 days. The medication history enumerated analgesics, antacids, anticonvulsants, antidepressants, antihistamines, antihypertensives, antiparkinson pills, bronchodilators, cardiac drugs (antiarrhythmic drugs), beta blockers or alpha/beta adrenergic blockers, corticosteroids, cytotoxic drugs, diuretics, hormones, insulin, laxatives, major tranquilizers, minor tranquilizers, narcotics, over-the-counter hypnotics, oxygen, sedative hypnotics, stimulants, vasodilating drugs, and other drugs. During the 1-week home activity recordings, the women completed a daily sleep log reporting bedtimes, sleep times, time to fall asleep (SRSL), wake up times, and when they took the actigraph off the wrist, among other items. A daily medication history within the sleep log recorded nonsteroidal anti-inflammatory analgesics, estrogen, progestin, and sleeping pills for each night. This study focused on the SRSL from these daily sleep logs, specifically the question "How long did it take you to fall asleep last night?" For most of the items, the women contributed complete data and could be included in all analyses.
Psychiatric diagnoses including depressive disorders were done by a board-certified psychiatrist using the Structured Clinical Interview for DSM-IV Axis I Disorders-Non-patient Edition (SCID) (16). The global assessment of functioning scale (GAF scale) of Axis V in SCID evaluated general functioning level; higher values reflected better overall functioning. DSM-IV sleep disorder diagnosis was also made, based on the subjective data, interviews, and actigraphic and oximetry recordings. DSM-IV permitted sleep diagnoses without polysomnography.
Actigraphic data
Wrist activity was recorded with the Actillume I device (Ambulatory Monitoring, Inc., Ardsley, New York, U.S.A.), using a precision accelerometer for 7 days (n=363) except for some subjects measured for 6 days (n=21). The sleep/ wake state of each minute was determined with a computer algorithm (17). This automatic sleep scoring was edited with assistance of daily sleep logs, notes, the illumination channel from the Actillume, and Webster's rules (18). The actigraphic sleep latency (ASL) was the interval from bedtime to the first minute scored as sleep.
6-Sulfatoxymelatonin (aMT6s) assays
To obtain a marker of circadian system phase, the women were asked to collect and measure every fractional urine voiding volume over two 24-hr intervals in the course of the week, approximately 3 days apart. They were instructed to urinate approximately every 2 hr during the day and to collect all nocturnal voidings, which resulted in an average of 10 samples per 24 hr. A 2-mL aliquot associated with each collection interval was frozen at home and then later stored at -70℃ for further assaying in the laboratory. Urinary aMT6s was assayed by radioimmunoassay (RIA) using melatonin kits (ALPCO Diagnostics, Windham, HN, U.S.A. with reagents from Stockgrand LTD) using a 125I-aMT6s tracer (19). At a sample dilution of 1:125, the sensitivity of the assay was <0.2 ng/mL. Intra- and inter-assay coefficients of variation were 3.3% and 6.7%, respectively. When necessary, the sensitivity of this assay was increased further by lessening the dilution factor. The excretion rate (ng/hr) between voidings was computed and transformed into 5 min epochs for time series display and cosine analysis. Further details of analyzing melatonin data were described in Tuunainen et al. (8). Subjects with reliable aMT6s (n=332) were selected.
Statistical analysis
Data analyses were performed with SPSS 12.0 statistical software (SPSS, Inc., Chicago, IL, U.S.A.). Two-sided p<0.05 was regarded as statistically significant. SRSL was transformed by common log transformation to normalize SRSL data. LT-SRSL (log-transformed SRSL) was used in statistical analyses. The demographic data set included age, BMI, systolic and diastolic blood pressures, and the use of antihypertensive drug. The behavioral symptom data set was composed of age, Burnam depressive mood score, GAF scale of DSM-IV Axis V, and hot flash rating log. The circadian rhythm data set included daily light exposure and wrist activity, the acrophases of circadian rhythms such as activity, light, sleep, and aMT6s, and the onset and offset times of sleep, and aMT6s. These variables were partially correlated with LT-SRSL controlling age and BMI. Correlations between SRSL and ASL or difference in SRSL-ASL were used by Spearman correlation because SRSL did not show Gaussian distribution. Multiple linear regression was used to analyze the relationships between the dependent variable of LT-SRSL and the independent variables of 3-separate variable sets: demographic, behavioral, and circadian. The non-parametric Kruskal-Wallis test was used to compare four different diagnostic groups in demographic, questionnaire, sleep and circadian rhythm data because the number of subject in the current depressive disorder group (n=10) was too small.
RESULTS
Subject characteristics
The mean age of the 384 women in this sample was 67.9±7.7 yr. The racial/ethnic distribution of the participants was 72.7% White, 13.3% Hispanic, 9.1% African-American, 4.2% Asian, and 0.8% Native American. Further characteristics of the sample are given in Table 1. Based on primary insomnia and depressive disorder, 4 groups were selected: 1) primary insomnia without any Axis I disorder (n=20), 2) current depressive disorder with insomnia (n=10), 3) past depressive disorder without any primary sleep disorder (n=77), and 4) control (n=140; subjects without any primary sleep disorder or any past or present Axis I psychiatric disorder). The subjects (n=137) who were diagnosed with any Axis I psychiatric disorder other than primary insomnia or depressive disorder were excluded in that grouping.
Relationships between sleep and aMT6s circadian rhythms are shown in Table 2A. The phase timing between the two rhythms was well-correlated, though not identical, but the mesor aMT6s and onset-to-offset duration were not related to sleep duration. The sleep onset-to-offset duration (471.5±58.1 min) was shorter than the aMT6s (588.3±115.9 min) onset-to-offset duration. Illumination exposure and activity were correlated in both timing and rhythm amplitude (Table 2B).
Comparison of self-reported vs. actigraphic data
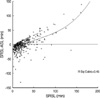
The mean SRSL was 26.5 min (SD 24.4; range, 0.0-161.4). The mean ASL measured by the Actillume was 27.8 min (SD 20.0; range 4.7-157.6). SRSL and ASL were correlated rs=0.387 (p<0.001), but showed a significant mean difference (Table 3). Self-reported and actigraphic data were more strongly correlated for other sleep variables than for the sleep latencies (Table 3). Although SRSL was correlated with the difference in SRSL and ASL (SRSL-ASL) (rs=0.603, p<0.001), the differences between SRSL and ASL tend to be negative in the short SRSLs whereas positive in the long SRSLs (Fig. 1). As compared to ASL, the short SRSLs tended to be underestimated whereas the long SRSLs above 50 min tended to be overestimated (Fig. 1).
Correlates of SRSL
LT-SRSL did not correlate with the subject's age or BMI. In partial correlations controlled for age and BMI, LT-SRSL was correlated with the insomnia factor (rp=0.331, p<0.001), the Burnam depression screening scale (rp=0.312, p<0.001), the hot flash rating log (rp=0.163, p=0.001), and GAF scale (rp=-0.257, p<0.001). LT-SRSL was significantly associated with systolic (rp=0.136, p=0.022) and diastolic (rp=0.132, p=0.027) blood pressures recorded at intake, use of antihypertensive drugs (rp=0.218, p<0.001), beta blockers (rp=0.176, p=0.004), cardiac drugs (rp=0.132, p=0.031), insulin (rp=0.168, p=0.006), and diuretics (rp=0.118, p=0.055), but was not correlated with the uses of sedative and hypnotics, antidepressants, anticonvulsants, antihistamines, and minor tranquilizers. LT-SRSL was correlated with daily light exposure (log10 lux) rp=-0.239, p<0.001), daily wrist activity (rp=-0.128, p=0.028), the acrophase of aMT6s excretion (rp=0.143, p=0.014) and the offset time of aMT6s excretion (rp=0.204, p<0.001) in partial correlations controlled for age of circadian rhythm variables.
Factors affecting SRSL
Multiple linear regression analysis showed that the best-fit model to predict LT-SRSL included the use of antihypertensive drugs (p=0.008) from the demographic data set, GAF scale of DSM-IV Axis V (p=0.004) from the behavioral symptoms data set, and daytime light exposure (p=0.023) from the circadian rhythm data set. In contrast, other variables did not add significant contributions to the model (Table 4).
Comparison of psychiatric diagnostic groups
The sleep, circadian rhythm, questionnaire, and demographic data were compured among four different diagnostic groups (Table 5). In the sleep data, SRSL, ASL and self-reported sleep period time (SPT) showed significant differences, but actigraphic SPT did not. The circadian rhythm data did not show any significant differences. The questionnaire data associated with the insomnia factor (Levine's factor), Burnam-Rand depression P index, and GAF score showed significant differences, but the hot flash rating log did not. In the demographic data, systolic BP showed a significant difference, but diastolic BP, age, and BMI did not.
DISCUSSION
The short subjective SRSLs appeared to be underestimated and the long SRSLs more than 50 min appeared to be overestimated as compared with objective ASL (Fig. 1). There is a well-known tendency to overestimate sleep onset latency in primary insomnia (20). The discrepancy between SRSL and ALS in primary insomnia may be due to distorted sleep perception affected by presleep cognitive and physiological arousal, as suggested by Tang and Harvey (21). While many studies about overestimated sleep latency had been done, we have found no discussion on underestimated sleep latencies that may be clinically of less concern.
The values of LT-SRSL were significantly associated with the use of antihypertensive drugs, decreased GAF scale of DSM-IV Axis V, and decreased daily light exposure in multiple linear regression analyses intended to emphasize the major correlates. Possible means to alleviate lengthened SRSL may include selecting antihypertensive drugs not provoking insomnia, alleviating impairments caused by mental illnesses such as the relief of affective illnesses and anxiety disorders, and promoting increased daily light exposure in underexposed subjects.
The current data showed that an increased SRSL was related to a mixture of factors, that is, other sleep complaints, indicators of depression, reported hot flashes, general measures of activity and global function (inversely), hypertension, medications such as antihypertensive drugs, and delayed circadian rhythms in several indices. It has often been reported that depression (as indicated by the Burnam mood screening scale) was correlated with subjective sleep latency. Depression was reported as a risk factor associated with insomnia (22). Chronic insomnia was related to major depression (23). Hot flashes are one of vasomotor symptoms associated with insomnia (24). What the GAF scale of Axis V in DSM-IV accessing psychosocial functioning was inversely correlated with SRSL suggests that primary insomnia, depressive disorder and some other psychiatric disorders decreasing GAF can be related to the increased SRSL. Unexpectedly, SRSL was not correlated with the uses of sedative and hypnotics. It might be inferred that the subjects taking those drugs one time per week were included in that medicated group or that SRSL was not likely to be reported short in the group taking those drugs everyday.
SRSL was inversely correlated with the levels of daily light exposure and wrist activity, but SRSL was not correlated with the acrophases of light or activity. One causal pathway might be that low light exposure leads to depression, which leads to both lower activity and longer sleep latency. Although there is a limitation of using self-assessment to measure sleep and exercise in the methodology, some studies (25) reported that exercise promoted sleep, as suggested by the reverse relationship between SRSL and the level of daily activity presented in the present paper. The review article by Montgomery and Dennis (26) also showed exercise improved sleep onset latency in elderly individuals. However, Youngstedt et al. (27) reported that exercise did not promote sleep: an explanation might be that daytime activity might often be a proxy for daylight exposure, as in the association of daylight exposure and daytime activity presented in this paper.
SRSL was correlated with the acrophase and the offset time of aMT6s, but it was not correlated with the onset time of aMT6s. This might suggest that delayed circadian rhythms can prolong sleep latency. It is notable that the offset time of aMT6s excretion correlated significantly with SRSL instead of the onset time of aMT6s excretion. This might suggest that the melatonin offset is the more functionally important marker to predict SRSL. Unexpectedly, SRSL was not significantly correlated with the acrophase, onset and offset time of actigraphic sleep. Perhaps this indicates that the underlying circadian process is more closely anchored in the circadian rhythm of aMT6 less affected by environmental factors as compared to the circadian rhythm of sleep.
The sleep, circadian rhythm, questionnaire, and demographic data were compared among four different diagnostic groups. SRSL, ASL, self-reported SPT, insomnia factor (Levine's factor), Burnam-Rand depression P index, GAF score, and systolic BP showed significant differences. It is of interest that the difference in total sleep time between groups was greater as reported subjectively than objectively observed. This may reflect a negative cognitive self-perception of sleep among depressed and insomniac patients. It was notable that systolic BP was highest in the current depressive group. Scherrer et al. (28) reported that hypertension was significantly associated with the degree of depression in epidemiological twin study. However, the present results had a limitation in that the number of current depressive group was relatively small as compared with other groups.
The current study had some other limitations. It was based partly on retrospective data from a study not prospectively designated to test the hypotheses. Another limitation was the potential inaccuracy of SRSL by memory bias when the subjects were asked to estimate SRSR in the next morning. Another limitation was the modest inaccuracy of the actigraphic method for the exact evaluation of sleep data not supported by nocturnal polysomnography (NPSG). Especially, ASL may be relatively unreliable actigraphic measure because some sleepers may lie in bed motionless before they actually fall asleep. ASL correlated less than other actigraphic measures with self-reported sleep variables as indicated in Table 3. Another limitation of the study was that the circadian rhythms of aMT6s might be partly masked by room illumination (29). The association between SRSL and circadian rhythm data, especially the circadian rhythm of melatonin, might be underestimated by the malsynchronization and the phase dispersion of melatonin circadian rhythm due to aging (30).
In spite of the limitations aforementioned, this study suggested that SRSL may be determined in a complex manner by psychophysiological factors as well as circadian rhythm function. The therapeutic approaches such as increase of daylight exposure, improvements in general health, or modification of anti-hypertensive pharmacotherapy could be suggested in the long SRSLs that might have trouble falling asleep.





 XML Download
XML Download