

 ePub
ePub Citation
Citation Print
Print


| Korean J Gastroenterol. 2016 Jan;67(1):28-34. English. Published online Jan 26, 2016. https://doi.org/10.4166/kjg.2016.67.1.28 | |
| Copyright © 2016 The Korean Society of Gastroenterology | |
|
Baek Gyu Jun,
Sae Hwan Lee,
Hong Soo Kim, | |
| Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. | |
|
1Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea. | |
|
2Department of Internal Medicine, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea. | |
|
3Department of Internal Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea. | |
| Received October 14, 2015; Revised December 25, 2015; Accepted December 29, 2015. | |
|
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- | |
|
Abstract
| |
|
Background/Aims
The optimal timing for discontinuing oral antiviral therapy in patients with HBeAg-positive chronic hepatitis B (CHB) is unclear. The aim of our study was to investigate sustained remission after stopping antiviral therapy in patients with HBeAg-positive CHB.
Methods
We analyzed the medical records of 58 patients who were HBeAg-positive and had discontinued antiviral therapy. Antiviral therapy was discontinued after HBeAg seroconversion and HBV DNA negativity for 6-12 months with consolidation therapy. Virologic relapse was defined as an increase in serum HBV DNA >2,000 IU/mL.
Results
No difference was observed between the virologic non-relapse and virologic relapse groups in baseline HBV DNA level (p=0.441) or duration of seroconversion (p=0.070). Time-to-undetectable HBV DNA during treatment was shorter in the virologic non-relapse group (29 patients) compared to the relapse group (29 patients) (4.9±2.6 vs. 13.2±12.7 months; p<0.01). Cumulative relapse rates were 12.7 in month 3, 32.7 in month 6, 47.3 in month 12, and 52.7% in month 18. We determined by multivariate analysis that the consolidation period (≥18 months, p=0.020) and early virologic response (HBV DNA <20 IU/mL) at six months during antiviral therapy (p=0.017) were significant predictors for sustained remission.
Conclusions
A consolidation period of at least 18 months and early virological response at six months during antiviral therapy were associated with sustained remission in patients with HBeAg-positive CHB after treatment. |
|
Keywords: Treatment; Chronic hepatitis B; Discontinuation; Remission; Relapse |
|
|
INTRODUCTION
|
HBV is an important contributor to liver disease, and chronic HBV infection can cause cirrhosis and hepatocellular carcinoma (HCC).1 Antiviral therapy with nucleos(t)ides (NAs) is effective in suppressing viral replication to normalize liver enzymes in patients with chronic HBV infection.2, 3 However, virologic relapse often occurs after treatment, necessitating long-term antiviral therapy in such patients. Long-term treatment entails considerable financial burden on national health care systems.4, 5 Because the optimal time to discontinue antiviral drug therapy is unclear, it is difficult to formulate a plan for discontinuation of oral NA antiviral therapy, needed to save cost and improve patient compliance.
In patients with HBeAg-positive chronic hepatitis B (CHB), current clinical practice guidelines suggest that treatment can be stopped after HBeAg seroconversion and an additional six to twelve months of consolidation therapy.6, 7 The Asian Pacific Association for the Study of the Liver (APASL) guidelines recommend that treatment should be continued until the patient has achieved HBeAg seroconversion and undetectable serum HBV DNA with at least six months of additional treatment after the appearance of anti-HBe.6
The durability of virologic non-relapse after treatment discontinuation appears to be low in patients with HBeAg-positive CHB. Patients experience high virological relapse rates after treatment, even when following the current recommendations.8, 9, 10, 11, 12 In a Korean study, younger age, lower bilirubin, and a longer consolidation period were predictive of sustained remission.8 Liang et al.10 reported that serum HBsAg levels at the end of treatment and rate of HBV DNA suppression are important for determining the appropriate time to stop antiviral drug treatment. The level and kinetics of HBsAg have recently emerged as useful tools for predicting virologic response and relapse after treatment discontinuation.10, 13, 14 However, the factors associated with virologic relapse have not been assessed. To improve the sustained remission rate in patients with CHB, more stringent criteria are needed to update practice guidelines.
The aim of this study was to investigate the factors predicting sustained remission after stopping antiviral therapy in patients with HBeAg-positive CHB.
|
SUBJECTS AND METHODS
|
1. Patients
We analyzed the medical records of patients who were HBeAg-positive and had discontinued antiviral therapy from March 2008 to December 2013 at Soonchunhyang University Hospitals in Cheonan, Seoul, and Bucheon, and at Gangneung Asan Hospital, Korea. We selected as study subjects patients who had discontinued antiviral therapy following HBeAg seroconversion and maintained undetectable HBV DNA for at least six months, as recommended by the APASL in 2008. We also required posttreatment care for at least 12 months, and analyzed until 24 months maximum. All patients had serum HBV DNA, serologic hepatitis B markers, and liver biochemical tests every three to six months. We excluded patients who were infected concurrently with hepatitis C, hepatitis D, or human immunodeficiency viruses, were exposed to hepatotoxic drugs, consumed a significant amount of alcohol, or underwent interferon or immunosuppressive therapy. No patients had liver cirrhosis, HCC, or any other malignancy.
Virologic response was defined as undetectable HBV DNA in serum using a sensitive PCR assay6. Patients with an HBV load over 2,000 IU/mL after treatment discontinuation were characterized as having virologic relapse.15 Biochemical relapse was defined as return to an ALT level in serum more than twofold the upper limit of normal.6 The primary outcome was virologic relapse after cessation of antiviral therapy. This study was approved by the Investigation and Ethics Committee for Human Research at Soonchunhyang University Medical Center (Cheonan, Seoul, and Bucheon Hospital) and Ulsan University Medical Center (Gangneung Asan Hospital), and informed consent in writing was obtained from each patient in the study.
2. Laboratory methods
Serum HBV DNA was quantified using with the COBAS AmpliPrep-COBAS TaqMan HBV test (CAP-CTM; Roche Molecular Systems, Inc., Branchburg, NJ, USA), with a lower limit of detection of 20 IU/mL. Serum hepatitis markers including HBsAg, anti-HBs, HBeAg, and anti-HBe were detected using commercially available microparticle enzyme immunoassays (Abbott, Wiesbaden, Germany). Lamivudine-resistant mutations were identified using second-generation INNO-LiPA HBV DR v2 (Innogenetics NV, Ghent, Belgium).
3. Statistics
Statistical analysis was performed using SPSS (version 14.0; SPSS, Inc., Chicago, IL, USA). Continuous variables were expressed as means with standard deviation or medians with range, and categorical variables were expressed as a proportion. Student's t-test and Mann-Whitney U-test or χ2 test and Fisher's exact test were used to make comparisons between the sustained remission and relapse groups. The cumulative relapse rate was calculated by the Kaplan-Meier method, and the difference was determined by the log-rank test. Cox's proportional hazard model was used for multivariate analysis. Null hypotheses of no difference were rejected if p-values were less than 0.05, or, equivalently, if the 95% CIs of risk point estimates excluded 1.
|
RESULTS
|
1. Baseline characteristics
Eighty-six possible study subjects who were HBeAg-positive and had discontinued antiviral therapy were initially identified. Twenty-eight patients were excluded due to a history of interferon treatment (eight patients), not meeting the APASL recommendations (11 patients), less than 12 months of regular follow-up (3-6 months) after cessation of antiviral treatment (six patients), or malignancy (three patients). The remaining 58 patients were enrolled. The initial clinical features of the 58 patients in this study are described in Table 1. Twenty-three patients received 0.5 mg entecavir, 26 patients received 100 mg lamivudine, and nine patients received 10 mg adefovir combined with 100 mg lamivudine. No differences were observed between the virologic non-relapse and virologic relapse groups in terms of age, gender, baseline HBV DNA level, treatment naivety, lamivudine resistance, total treatment duration, or median follow-up duration after treatment. Time-to-first undetectable HBV DNA during treatment (4 [3-6] months vs. 9 [6-16.5] months; p<0.01) was shorter and duration of seroconversion was longer (21 [16-36] months vs. 13 [12-26.5] months; p=0.040) in the virologic non-relapse group compared to the relapse group, while baseline ALT (242 [119-798] IU/mL vs. 150 [83-331] IU/mL; p=0.003) was higher in the virologic non-relapse group compared to the relapse group.
|

2. Virological and biochemical relapse
After completing antiviral therapy, the cumulative relapse rates were 12.7 in month 3, 32.7 in month 6, 47.3 in month 12, and 52.7% in months 18 and 24 (Fig. 1). Most relapses (47.3%) occurred within one year after stopping antiviral therapy. The mean time tovirologic relapse is 15.6±8.8 months. When evaluating the influence of drug type on virologic relapse, no difference was detected among entecavir (50.9%), lamivudine (42.4%), and lamivudine with adefovir (42.4%). Of the 29 patients who had a virologic relapse, 10 also experienced a biochemical relapse, while nine (60.0%) of the 15 patients with posttreatment HBV DNA levels >10,000 IU/mL had biochemical relapse (Table 2). Seventeen (58.6%) patients who experienced virologic relapse resumed antiviral therapy. Among 12 patients who did not resume antiviral treatment, HBV DNA level decreased <2,000 IU/mL in eight patients and remained high without biochemical relapse in four patients at the end of follow-up.
|

|

3. Factors related to virological relapse
The Cox proportional hazard model was used to analyze factors predictive of sustained remission after cessation of antiviral therapy. In a univariate analysis, these included virologic response at six months, time to seroconversion (≥2 years), and consolidation period (≥18 months). However, multivariate analysis indicated that the consolidation period (≥18 months; hazard ratio [HR], 0.37; 95% CI, 0.16-0.85; p=0.020), and early virologic response (HBV DNA <20 IU/mL) at six months during antiviral therapy (HR, 0.38; 95% CI, 0.17-0.84; p=0.017) were significant predictor variable of virologic non-relapse. Consolidation period (≥12 months) and young age were not predictive factors of virologic non-relapse (Table 3).
|

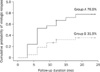
Cumulative relapse rates were significantly lower in the group with an HBV DNA response at six months (log-rank test, p<0.01; Fig. 2) and a significant reduction in cumulative relapse rates was seen for the group with a consolidation period of at least 18 months (log-rank test, p<0.01; Fig. 3). To analyze the relationship between consolidation period and HBV DNA response in relapse, we classified patients into three groups: group A, 23 (39.7%) patients with an HBV DNA response at six months and a consolidation duration of at least 18 months; group B, 22 (37.9%) patients with either an HBV DNA response at six months or a consolidation duration of at least 18 months; group C, 13 (22.4%) patients with no HBV DNA response at six months and consolidation duration <18 months after cessation of antiviral therapy. The cumulative relapse rate was significantly lower in group A than group B and C (log-rank test, p<0.01; Fig. 4).
|
|

|

|
DISCUSSION
|
Few studies have described how and when to discontinue antiviral therapy in patients with HBeAg-positive CHB, and the duration of the virologic response after ceasing antiviral therapy is unclear In our study, 58 patients were monitored after cessation of antiviral therapy. We found that the cumulative relapse rate at 12 months was 47.3%, similar studies reporting a cumulative virologic relapse rate of 42-67%.8, 9, 10, 12, 16 These high virologic relapse rates suggest that current international guidelines do not realistically predict the success of antiviral therapy discontinuation in patients with HBeAg-positive CHB. Most relapses occurred in the first 12 months after cessation of antiviral therapy in our study, similar to earlier studies.10, 16, 17 We believe that the first 12 months after cessation of antiviral therapy is a critical time in which to assess virologic relapse, and if a patient does not relapse within this period, they are more likely to remain in virologic non-relapse.
Low pretreatment HBV DNA level,16, 18, 19, 20 lower HBV DNA level at treatment discontinuation,21 genotype B,22 younger age,8, 12 longer duration of consolidation therapy23 and a higher total bilirubin level8 are associated with a low risk of posttreatment virologic relapse in HBeAg-positive patients. However, these parameters are not practical for determining when to stop antiviral therapy. In our study, we found that the baseline HBV DNA level, ALT, older age, gender, and total treatment duration could not predict the sustained response. Multivariate analysis showed that virologic response at six months and consolidation of at least 18 months were significantly predictive of virologic non-relapse in our study. The cumulative relapse rate was significantly lower in patients who had longer consolidation and rapid virologic suppression (Fig. 4), suggesting that we can cease antiviral therapy in patients who have rapid virologic suppression and longer consolidation.
Liang et al.10 demonstrated the importance of rapid virologic suppression on the risk of posttreatment relapse. Our study was consistent with these results, which showed that a rapid reduction of serum HBV DNA was highly predictive of virologic non-relapse after cessation of antiviral therapy in patients who are HBeAg-positive CHB. These results indicate that HBV DNA kinetics is important in predicting virologic non-relapse. Monitoring the HBsAg level at baseline or at the end of treatment could guide the timing of antiviral therapy cessation.10, 13, 14 Thompson et al.24 reported that a decline in HBsAg levels is associated with serum HBV DNA in HBeAg-positive CHB. Wehypothesized that for HBsAg, as well as HBV DNA, kinetics may be useful in predicting virologic relapse after treatment ceases. However, there are reports to the contrary, that quantitative HBsAg does not predict virologic relapse25, 26 or serologic relapse.27 Further studies should investigate the association of HBsAg level with virologic relapse.
Longer consolidation significantly reduces cumulative relapse rates at two years by up to 31% in our study (Fig. 2). Studies from Korea and Japan suggest that prolonged duration of lamivudine therapy reduces the relapse rate.8, 9, 11, 23 Ryu et al.23 showed that an additional 24 months of lamivudine therapy enhanced the durability of lamivudine-induced HBeAg seroconversion, and Song et al.12 found that long-term consolidation (>15 months) was associated with a reduced rate of relapse. A recent study also showed that prolongation of consolidation therapy beyond three years resulted in a reduction in virologic relapse episodes.25 On the basis of these results, the current consolidation duration recommended by international guidelines may not sufficefor a virologic non-relapse.
The current guidelines recommend that HBeAg-positive CHB patients with an HBV DNA level ≥105 copies/mL be considered for treatment intervention.6 In our study, high levels of HBV DNA (>10,000 IU/mL) were related to biochemical relapse compared to low levels of HBV DNA (<10,000 IU/mL) after treatment cessation (9/15 [60.0%] vs. 1/14 [7.1%], p<0.01; Table 2). These findings support the use of high posttreatment HBV DNA levels (>10,000 IU/mL) as a predictor of biochemical relapse, which could be useful in decidingresumption of antiviral treatment in patients experiencing virologic relapse.
Our patients were treated with oral antiviral agents including entecavir, lamivudine, and a lamivudine with adefovir combination. The cumulative relapse rate of entecavir was 60.9%, of lamivudine 42.3%, and of lamivudine with adefovir 44.4% (p=0.404). Entecavir was expected to have the lowest relapse rate due to a high resistance barrier and potent viral suppression, although no difference was observed. Sohn et al.11 reported that off-treatment remission rates were independent of NA antiviral potency, similar to what Song et al.12 reported. Therefore, factors such as consolidation duration and rapid virologic suppression may be more important than the type of drug in predicting virologic relapse.
Cessation of antiviral therapy is very important for both patients and physicians since lifelong use of antiviral agents is expensive. Some Asian countries reimburse the drug for a finite time regardless of cost,5 causing long-term financial problems for the health care system. Although NAs have few side effects compared to pegylated-interferon, the safety of NAs in long-term use is unknown.
Our study had several limitations. First, the sample size of this study was small. However, our study differs from previous studies because we included only patients who were HBeAg-positive. Second, this was a retrospectivestudy design, and thus selection or measurement bias could have interfered with the results. Third, our patients were treated with different types of oral antiviral agents, which led to subgroup analysis with each drug that concluded no difference in relapse rates, regardless of drug type. Fourth, owing to the use of clinical data, the baseline HBsAg level was not measured and thus could not be evaluated in this study.
In conclusion, virologic response atsix months during antiviral treatment and consolidation of at least 18 months were important predictors for virologic non-relapse after discontinuation of antiviral treatment. Treatment cessation was feasible in a select group of patients who have rapid virologic suppression and at least 18 months of consolidation.
|
Notes
|
Financial support:This work was supported by the Soonchunhyang University Research Fund.
Conflict of interest:None.
|
References
|
| 1. | Liaw YF. Natural history of chronic hepatitis B virus infection and long-term outcome under treatment. Liver Int 2009;29 Suppl 1:100–107. 
|
| 2. | Sung JJ, Tsoi KK, Wong VW, Li KC, Chan HL. Meta-analysis: Treatment of hepatitis B infection reduces risk of hepatocellular carcinoma. Aliment Pharmacol Ther 2008;28:1067–1077.
|
| 3. | Ahn SH, Chan HL, Chen PJ, et al. APPROACH Working Group. Chronic hepatitis B: whom to treat and for how long? Propositions, challenges, and future directions. Hepatol Int 2010;4:386–395.
|
| 4. | Chan HL. Antiviral therapy for chronic hepatitis B: challenges in Hong Kong. J Hepatol 2009;51:1088–1090.
|
| 5. | Dan YY, Aung MO, Lim SG. The economics of treating chronic hepatitis B in Asia. Hepatol Int 2008;2:284–295.
|
| 6. | Liaw YF, Kao JH, Piratvisuth T, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2012 update. Hepatol Int 2012;6:531–561.
|
| 7. | Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology 2009;50:661–662.
|
| 8. | Byun KS, Kwon OS, Kim JH, et al. Factors related to post-treatment relapse in chronic hepatitis B patients who lost HBeAg after lamivudine therapy. J Gastroenterol Hepatol 2005;20:1838–1842.
|
| 9. | Ito K, Tanaka Y, Orito E, et al. Predicting relapse after cessation of Lamivudine monotherapy for chronic hepatitis B virus infection. Clin Infect Dis 2004;38:490–495.
|
| 10. | Liang Y, Jiang J, Su M, et al. Predictors of relapse in chronic hepatitis B after discontinuation of anti-viral therapy. Aliment Pharmacol Ther 2011;34:344–352.
|
| 11. | Sohn HR, Min BY, Song JC, et al. Off-treatment virologic relapse and outcomes of re-treatment in chronic hepatitis B patients who achieved complete viral suppression with oral nucleos(t)ide analogs. BMC Infect Dis 2014;14:439.
|
| 12. | Song MJ, Song do S, Kim HY, et al. Durability of viral response after off-treatment in HBeAg positive chronic hepatitis B. World J Gastroenterol 2012;18:6277–6283.
|
| 13. | Lee JM, Ahn SH, Kim HS, et al. Quantitative hepatitis B surface antigen and hepatitis B e antigen titers in prediction of treatment response to entecavir. Hepatology 2011;53:1486–1493.
|
| 14. | Chen CH, Lu SN, Hung CH, et al. The role of hepatitis B surface antigen quantification in predicting HBsAg loss and HBV relapse after discontinuation of lamivudine treatment. J Hepatol 2014;61:515–522.
|
| 15. | Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006;295:65–73.
|
| 16. | Fung J, Lai CL, Tanaka Y, et al. The duration of lamivudine therapy for chronic hepatitis B: cessation vs. continuation of treatment after HBeAg seroconversion. Am J Gastroenterol 2009;104:1940–1946. quiz 1947.
|
| 17. | Wang L, Liu F, Liu YD, et al. Stringent cessation criterion results in better durability of lamivudine treatment: a prospective clinical study in hepatitis B e antigen-positive chronic hepatitis B patients. J Viral Hepat 2010;17:298–304.
|
| 18. | Yeh CT, Hsu CW, Chen YC, Liaw YF. Withdrawal of lamivudine in HBeAg-positive chronic hepatitis B patients after achieving effective maintained virological suppression. J Clin Virol 2009;45:114–118.
|
| 19. | Song BC, Suh DJ, Lee HC, Chung YH, Lee YS. Hepatitis B e antigen seroconversion after lamivudine therapy is not durable in patients with chronic hepatitis B in Korea. Hepatology 2000;32:803–806.
|
| 20. | Lee KM, Cho SW, Kim SW, Kim HJ, Hahm KB, Kim JH. Effect of virological response on post-treatment durability of lamivudine-induced HBeAg seroconversion. J Viral Hepat 2002;9:208–212.
|
| 21. | Lee HC, Suh DJ, Ryu SH, et al. Quantitative polymerase chain reaction assay for serum hepatitis B virus DNA as a predictive factor for post-treatment relapse after lamivudine induced hepatitis B e antigen loss or seroconversion. Gut 2003;52:1779–1783.
|
| 22. | Chien RN, Yeh CT, Tsai SL, Chu CM, Liaw YF. Determinants for sustained HBeAg response to lamivudine therapy. Hepatology 2003;38:1267–1273.
|
| 23. | Ryu SH, Chung YH, Choi MH, et al. Long-term additional lamivudine therapy enhances durability of lamivudine-induced HBeAg loss: a prospective study. J Hepatol 2003;39:614–619.
|
| 24. | Thompson AJ, Nguyen T, Iser D, et al. Serum hepatitis B surface antigen and hepatitis B e antigen titers: disease phase influences correlation with viral load and intrahepatic hepatitis B virus markers. Hepatology 2010;51:1933–1944.
|
| 25. | Chi H, Hansen BE, Yim C, et al. Reduced risk of relapse after long-term nucleos(t)ide analogue consolidation therapy for chronic hepatitis B. Aliment Pharmacol Ther 2015;41:867–876.
|
| 26. | Chen EQ, Wang TT, Bai L, et al. Quantitative hepatitis B surface antigen titres in Chinese chronic hepatitis B patients over 4 years of entecavir treatment. Antivir Ther 2013;18:955–965.
|
| 27. | Gish RG, Chang TT, Lai CL, et al. Quantitative hepatitis B surface antigen analysis in hepatitis B e antigen-positive nucleoside-naive patients treated with entecavir. Antivir Ther 2013;18:691–698.
|