

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The epidemic of tobacco use is a significant global public health threat that contributes to a substantial burden of disease and economic costs. Despite the abundant scientific evidence collected over the past 70 years describing the health hazards of tobacco products, smoking remains the leading cause of preventable disease, disability, and death.123 While the figures have steadily decreased over time, in 2020, approximately 22.3% of the global population aged 15 and older (an estimated 1.30 billion people) were currently using some form of tobacco.3 In 2019, tobacco use (smoking, second-hand smoke exposure, and smokeless tobacco) was the second-leading global risk factor for attributable deaths after high systolic blood pressure.4 The majority of smoking-related deaths are linked to four non-communicable diseases: ischemic heart disease, chronic obstructive pulmonary disease, stroke, and cancer of the trachea, bronchi, and lungs. Unless more effective measures are implemented to combat the tobacco epidemic, it is projected to result in over 1 billion deaths in this century.1
South Korea has historically recorded a high prevalence of smoking and cigarette consumption. As part of the global efforts to reduce smoking, Korea implemented national tobacco control policies in 1995 that have been continuously expanded and strengthened.5 Nevertheless, the daily smoking rate for men in Korea substantially exceeds the global median of daily smoking rates determined by the Organization for Economic Co-operation and Development (OECD) for populations aged 15 years and older.6 Studies have consistently highlighted the significant disease burden associated with smoking in Korea.5789 In 2021, lung cancer was the most prevalent newly diagnosed cancer in Korean men and the fourth most common new cancer in women.10 Smoking was a significant factor contributing to overall mortality, cancer mortality (all types), and especially lung cancer mortality among Koreans.11
Given the consistently high smoking rates, the severity of associated health consequences, and the substantial socioeconomic burden, prioritizing the cessation and prevention of tobacco use in Korea is crucial for public health authorities in the country. The recent emergence and extensive marketing of novel tobacco products, such as electronic nicotine delivery systems (ENDS or e-cigarettes) and heated tobacco products (HTPs), present additional challenges.121314 Tobacco control policies are crucial for improving individual health, reducing social health disparities, lowering national medical costs, and enhancing societal productivity. These policies necessitate evidence-based decision making and establishment of strategic goals.15 Therefore, gaining insights into the long-term trends and current epidemic features of tobacco use across demographics is essential for devising focused and effective tobacco control strategies. Of equal importance is the objective assessment and understanding of the impact of tobacco on individual and public health. Through the comprehensive monitoring of tobacco use patterns among different populations, policymakers and public health practitioners can effectively tailor interventions to address the unique challenges and needs of these groups.
The objective of this review is to present an updated overview and provide projections of the epidemiology of tobacco use in Korea by collating statistics from various national ministries and official agencies. Additionally, it aims to highlight public health issues associated with tobacco use.
Go to : 
SOURCES USED TO REVIEW EPIDEMIOLOGICAL INDICATORS
To examine tobacco use statistics across diverse demographics in Korea and facilitate a comprehensive understanding of use patterns, this study incorporates various data sources.
OECD Health Statistics
OECD Health Statistics provide the most comprehensive source of comparable health and health systems data across OECD and selected non-OECD countries, dating back to 1960.616 These statistics include data on tobacco consumption (considered a non-medical determinant of health), enabling cross-country comparisons of the proportion of daily smokers in populations aged 15 years and older.
Korea National Health Statistics from the Korea National Health and Nutrition Examination Survey (KNHANES)
KNHANES is a comprehensive, nationwide representative sample survey conducted periodically by the Korea Disease Control and Prevention Agency (KDCA) to assess the health and nutritional status of the Korean population.17 This source was used to examine long-term trends in tobacco use among Korean adults aged 19 years and older, as well as tobacco use statistics across various demographics.
Korea Youth Risk Behavior Survey (KYRBS)
KYRBS is a national, cross-sectional survey designed to evaluate health-risk behaviors among middle- and high-school students in Korea. Targeting a nationally representative population of students aged 12–18 years, this survey provides data on tobacco use among adolescents.18
Surveys and data on tobacco use among persons with disabilities
Statistics regarding tobacco use among individuals with disabilities are available from various sources, including the Healthcare statistics of Persons with Disabilities from the Korea National Rehabilitation Center, the Panel Survey of Employment for the Disabled from the Korea Employment Agency for Persons with Disabilities, and national health checkup data from the Korean National Health Insurance Service (NHIS). We reviewed cigarette smoking rates from various sources and compared these rates between individuals with and without disabilities (of varying severity and type).
Monitoring the use of novel tobacco products
KNHANES investigates the use of diverse tobacco products, including manufactured cigarettes, HTPs, e-cigarettes, and other items, such as dipping tobacco, water pipes, and cigars. Between 1998 and 2012, the survey focused solely on the rate of smoking cigarettes. Starting in 2013, the prevalence of e-cigarette use was assessed independently, and HTP use was incorporated in 2019. The survey currently calculates the prevalence of all tobacco product use, including cigarettes, HTPs, e-cigarettes, and other items. This comprehensive monitoring, including HTPs and e-cigarettes, was also reflected in the KYRBS, which targets youth.
Ethics statement
This study involved a review of published articles, reports, or open data obtained from various internet sources. The open data utilized in this study did not contain any personal information such as patient names, social security numbers, addresses, or phone numbers. As there were no ethical concerns involved, an Institutional Review Board review was deemed unnecessary for this study.
Go to :
A COMPARISON OF KOREA’S SMOKING PREVALENCE WITH OTHER COUNTRIES WORLDWIDE
The global prevalence of smoking has decreased substantially over the past 30 years.19 According to the OECD’s most recent time-trend analysis, the average daily smoking rate for individuals in OECD countries aged 15 and over fell from 20.6% in 2011 to 15.9% in 2021.16 However, there was considerable variation in daily smoking rates among individual countries, exceeding 25% in some and dropping below 10% in countries such as Iceland, Costa Rica, Norway, Mexico, Canada, the United States (US), New Zealand, and Sweden (Fig. 1A).
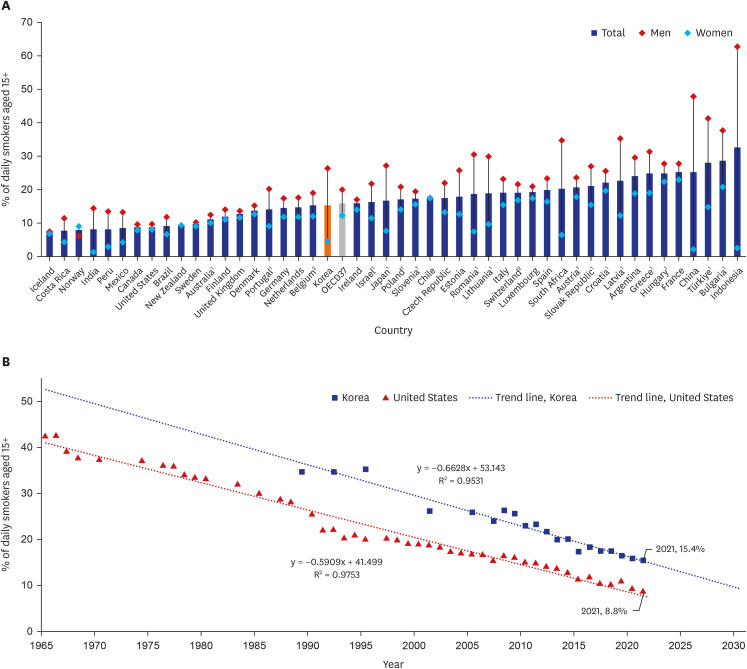 | Fig. 1A comparison of the percentage of the population aged 15 and older who are daily smokers, by country. (A) Percentage of daily smokers aged 15 and older across OECD and selected non-OECD countries, by sex, in 2021. Countries marked with 1 indicate data from 2019 and countries marked with 2 indicate data from 2017–2018. (B) Percentage of daily smokers aged 15 and older in the United States and South Korea from 1965–2021. Trend line statistics were calculated using a linear regression analysis.Data source: OECD (2023), “Population aged 15 and over smoking daily, by sex, 2021 (or nearest year),” in Health at a Glance 2023: OECD Indicators, OECD Publishing, Paris, https://doi.org/10.1787/32fae449-en.
|
Korea’s overall smoking rate of 15.4% aligns with the OECD average of 15.9%. However, Korea exhibited a significant gender disparity in smoking, with a gap of 21.8 percentage points between genders, compared to the OECD average of 7.6 percentage points. For men, the highest smoking rates were in Indonesia, China, and Turkey (over 40%), while the lowest were in Norway, Iceland, Canada, New Zealand, and the US (less than 10%). In Korea, the smoking rate for men was 26.3% in 2021, surpassing the OECD average (19.9%) by 6.4 percentage points. By contrast, women in Korea had one of the lowest rates at 4.5%, along with India, China, Indonesia, Peru, Costa Rica, and Mexico (less than 5%).
The US was among the first countries that introduced tobacco control policies to protect public health and to reduce smoking rates. Although the US is home to multinational tobacco companies and has not yet ratified the Framework Convention on Tobacco Control (FCTC), its tobacco control policies and models significantly influenced the early development of tobacco control efforts in Korea.20 In 1964, the first Surgeon General’s report on smoking was published. Titled “Smoking and Health: Report of the Advisory Committee to the Surgeon General of the Public Health Service,” the report recognized the link between smoking and health consequences and provided an objective synthesis of the evidence based on causal criteria.21 Following this, health warnings began appearing on cigarette packs in 1966 in response to congressional legislation. Additionally, the US implemented regulations on tobacco products and their advertising in conjunction with anti-smoking mass media campaigns. Tobacco control efforts included banning the sale of tobacco products to youth (raising the minimum sales age to 21), eliminating smoking in public places, enacting measures at state and federal levels, raising tobacco taxes, developing smoker treatment programs, and enhancing coverage of cessation treatments.22 Over the course of 60 years, these efforts resulted in a remarkable 79.2% decrease in the daily smoking rate among individuals aged 15 and over, from 42.4% in 1965 to 8.8% in 2021 (Fig. 1B).
In Korea, tobacco control policies began in earnest with the enactment of the National Health Promotion Act in 1995, approximately 30 years later than in the US.2324 Drawing on accumulated experience and examples of past tobacco control measures in developed countries such as the US, Korea was able to create effective tobacco control policies and initiatives. Furthermore, in recent years, there has been a notable increase in public awareness regarding the harmful effects of cigarettes compared to the past.
While the US daily smoking rate of 8.8% is 6.6 percentage points lower than Korea’s 15.4%, our findings show that the rate of decrease in daily smoking rates in Korea over the past 30 years has been steeper than in the US. This suggests that, like the US, Korea is making significant progress in reducing tobacco use, but the later implementation of tobacco control measures between the two countries may limit direct comparisons. However, if the current downward trend in the graph continues, the daily smoking rate among Korea’s population aged 15 and older is expected to fall below 10% after 2030, similar to that of the US.
To ensure continued reductions and accurately identify vulnerable groups in tobacco control efforts, a more detailed understanding of changes in tobacco use levels within countries is necessary, including tobacco control policies and demographic characteristics.
Go to :
ADVANCEMENTS IN TOBACCO CONTROL POLICIES AND LONG-TERM TRENDS IN TOBACCO USE IN KOREA
The FCTC was established by the World Health Organization (WHO) to present a comprehensive framework aimed at curbing tobacco supply and demand through a range of price and non-price measures.25 Price measures aim to reduce tobacco consumption by increasing the prices of tobacco products, including increasing product taxes and adding additional charges. It is recognized as one of the most effective tobacco control policies recommended by the WHO. In particular, it is the most cost-effective way to reduce tobacco use, especially among youth and low-income groups.26 Non-price policies refer to regulations and support policies such as designating non-smoking areas; banning tobacco advertising; creating regulations for tobacco product packaging and labeling (including pictorial warnings); running public campaigns; and providing education, treatment, and support for smoking cessation.
Korea became a party to the FCTC in 2005 and has since consistently strengthened tobacco control measures to implement the guidelines outlined by the FCTC. As the 20th anniversary of the FCTC ratification approaches, it is crucial to assess the progress of Korea’s tobacco control policies in terms of the changes in smoking rates thus far and discuss directions for further advancements.
Long-term trends in adult tobacco use
As a country, Korea has a high prevalence of smoking in the adult male demographic. According to the national smoking survey conducted by the Korean National Tuberculosis Association, the prevalence of smoking among adult males reached its peak at 79.3% in 1980.27 It is not an exaggeration to say that the Korean government had almost no tobacco control policies during this period. Restrictions on cigarette advertising began in 1986 with the enactment of the Tobacco Business Act. However, tobacco control policies were implemented in earnest with the legislation of the National Health Promotion Act in 1995 and the subsequent launch of the National Health Promotion Fund, funded by a tobacco tax, in 1997 (Table 1).
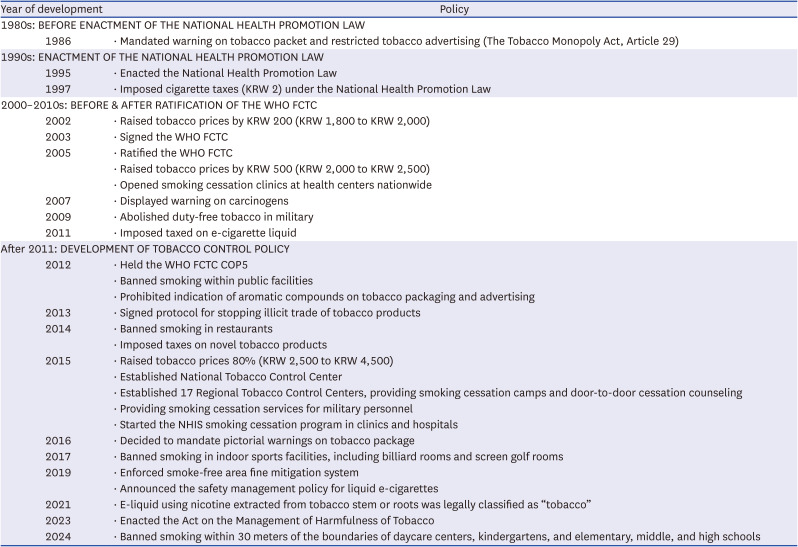
Table 1
Progress of tobacco policy in Korea
KRW = Korean won, WHO = World Health Organization, FCTC = Framework Convention on Tobacco Control, NHIS = National Health Insurance Service.
Data source: National Tobacco Control Center, Korea Health Promotion Institute. “History of tobacco control policy, At a Glance: Tobacco Control in Korea.” https://nosmk.khepi.or.kr/ntcc/eng/subIndex/548.do. accessed 13 Mar 2024.
![]()
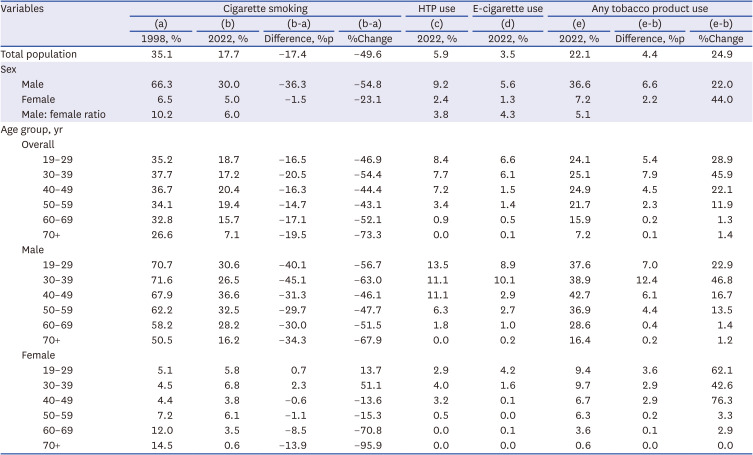
Although a few more surveys on smoking rates were conducted after the 1980s, the regular compilation of national statistics regarding smoking prevalence (in a nationally representative sample of Koreans) started in 1998 with the KNHANES and has continued to the present.23 Notable shifts in smoking prevalence among adults aged 19 years and older in Korea have been observed during these periods (Fig. 2A, Table 2). In 1998, the prevalence of cigarette smoking was notably high. Approximately 35.1% of the Korean adult population (including 66.3% of male adults) reported being current smokers. Smoking was more socially accepted during this period, and public awareness about the health risks associated with tobacco use was lower. However, over the course of three decades, Korea has implemented a range of tobacco control measures and anti-smoking movements to reduce the prevalence of smoking. As a result, awareness of the adverse effects of smoking increased in Korea in a relatively short period of time.27
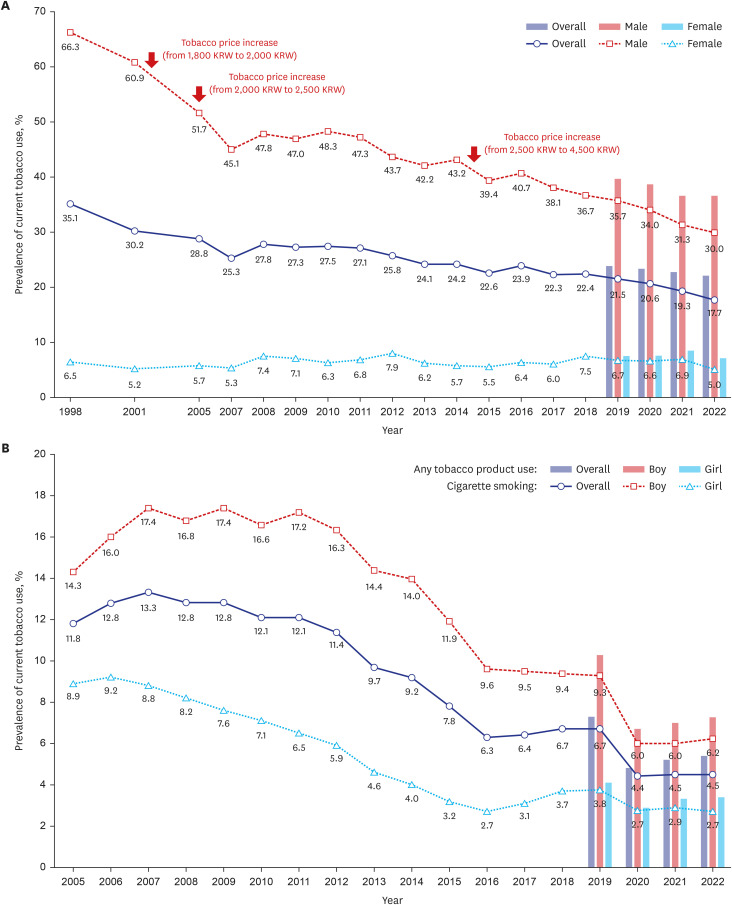 | Fig. 2Long-term trends in tobacco use among (A) adults aged 19 and older (1998–2022) and (B) adolescents aged 13 to 18 (2005–2022) in South Korea, by sex.Data source for (A) adults: Korea Disease Control and Prevention Agency (2023), “Korea Health Statistics 2022: Korea National Health and Nutrition Examination Survey (KNHANES IX-1),” https://knhanes.kdca.go.kr/knhanes/sub04/sub04_04_01.do.
Data source for (B) adolescents: Korea Disease Control and Prevention Agency (2023), “18th Korea Youth Risk Behavior Survey,” https://www.kdca.go.kr/yhs/.
|
Table 2
Percentage of adults aged 19 and older who reported the current use of tobacco products, grouped by type of product, sex, and age cohort
HTP = heated tobacco product.
Data source: Korea Disease Control and Prevention Agency (2023), “Korea Health Statistics 2022: Korea National Health and Nutrition Examination Survey (KNHANES IX-1),” Korea Disease Control and Prevention Agency, Osong, https://knhanes.kdca.go.kr/knhanes/sub04/sub04_04_01.do.
![]()
In the 2000s, two increases in tobacco product prices, in 2002 and 2005, resulted in a significant decline in the adult cigarette smoking rate. Particularly noteworthy was the substantial drop in the male adult cigarette smoking rate, which fell by 9.2 percentage points, from 60.9% in 2001 to 51.7% in 2005. Concurrent non-price measures included the notable expansion of smoke-free areas and the establishment of smoking cessation clinics at public health centers nationwide. The FCTC was also ratified in 2005. The impact of these measures persisted into the following years, with the male smoking rate further decreasing to 45.1% in 2007, marking the first time it fell below 50%. The smoking rate among all adults fell below 30% for the first time in 2005 and reached 25.3% in 2007. However, it increased slightly afterward and plateaued until 2011.
A more robust tobacco control policy was promoted in the 2010s to implement the FCTC’s six MPOWER measures (monitoring tobacco use and prevention policies, protecting people from tobacco smoke, offering help to quit tobacco use, warning about the dangers of tobacco, enforcing bans on tobacco advertising and sponsorship, and raising taxes on tobacco).28 More aggressive regulations included granting local governments the authority to designate smoke-free areas and banning smoking in restaurants and all public facilities. In 2015, the price of tobacco products increased by 80%, from 2,500 Korean won (KRW) to 4,500 KRW. Simultaneously, the National Tobacco Control Center and 17 Regional Tobacco Control Centers were established, providing expanded national smoking cessation support services, including smoking cessation camps and door-to-door cessation counseling. The NHIS smoking cessation program in clinics and hospitals was also launched in 2015, based on strong evidence that behavioral support and pharmacotherapies enhance individuals' chances of successfully quitting smoking. This program provides financial assistance for smokers to receive professional consultations with physicians and to purchase smoking cessation medications. It subsidizes consultation fees for up to six visits and supports the purchase of smoking cessation medications (e.g., bupropion, varenicline, and nicotine replacement therapy) for 8 to 12 weeks after registration.29 As a result, the overall adult cigarette smoking rate further dropped to 22.6% in 2015. Among adult males, the rate decreased to 39.4%, marking the first time it fell below 40%.
From the late 2010s to the early 2020s, additional policies were introduced, including the requirement for pictorial warnings on cigarette packages, the expanded enforcement of smoke-free areas, and the imposition of taxes on tobacco products containing nicotine extracted from tobacco stems or roots. In 2023, the Act on the Management of Tobacco Harmfulness was enacted. In August 2024, smoking bans were extended to include areas within 30 meters of daycare centers, kindergartens, and elementary, middle, and high schools. These measures reflect Korea’s continued progress in tobacco control policy. The overall cigarette smoking rate dipped below 20% for the first time in 2021. As of 2022, the overall cigarette smoking rate is 17.7%, indicating a remarkable decrease of 17.4 percentage points (a 49.6% decrease) compared to 1998. Notably, the reduction in the cigarette smoking rate among adults seems to be primarily attributable to a significant decline among men. As of 2022, the male cigarette smoking rate stands at 30.0%, marking a significant decrease of 36.3 percentage points (a 54.8% decrease) from the rate observed in 1998. In contrast, the prevalence of cigarette smoking among females fluctuated between 5% and 7% during this period, ultimately reaching only 5.0% in 2022. This represents a decrease of only −1.5 percentage points (a 23.1% decrease) from 1998.
Long-term trends in adolescent tobacco use
The prevalence of current cigarette smoking among Korean middle and high school adolescents has shown a decreasing trend (Fig. 2B). Specifically, there was a notable decrease between 2011 and 2016. The 80% increase in tobacco prices appears to have significantly contributed to the decline in cigarette smoking rates observed in 2015 and 2016, particularly among male youth. However, between 2016 and 2019, the rates plateaued or even increased, particularly among adolescent girls, until another significant decrease was observed in 2020, coinciding with the onset of the coronavirus disease 2019 pandemic. As of 2022, the overall prevalence of cigarette smoking among adolescents was 4.5%, marking a decrease of 7.3 percentage points (a 61.9% decrease) compared to 2005. However, this trend is currently plateauing again among both male and female youth.
For female youth, the decline in the prevalence of cigarette smoking began in the late 2000s. The most recent data for female youth recorded a prevalence of 2.7%. Among male youth, the decline began in the 2010s, with the most recent data showing a prevalence of 6.2%. However, it’s essential to note that the data is based on the KYRBS, which is conducted within schools. As a consequence, it fails to capture the prevalence of smoking among adolescents who are not part of the school system. According to the “2023 Out-of-School Youth Survey” released by the Ministry of Gender Equality and Family, the smoking rate among out-of-school youth was relatively high, at 19.3%.30 Additionally, because this was a self-reported online survey conducted during school hours, it may underestimate the actual smoking prevalence among Korean adolescents.
In conclusion, despite some limitations in the data, sustained declines in smoking prevalence have been observed among both adults and adolescents in Korea. These trends reflect the influence of expanded tobacco control policies and cessation services, proactive public health campaigns, systematic monitoring of key tobacco indicators, and changing social norms that increasingly view smoking as socially unacceptable. As shown in the WHO’s assessment of Korea’s compliance with MPOWER measures (Table 3), since 2013, Korea has consistently received “complete” evaluations for “Monitoring tobacco use and prevention policies (M),” “Offering help to quit tobacco use (O),” and “Warning about the dangers of tobacco (through anti-tobacco campaigns) (W).” Although the implementation of pricing policies remains insufficient, the increase in tobacco taxes during this period, along with various non-price strategies, appears to have played a significant role in reducing tobacco use. Nonetheless, challenges remain, particularly in addressing persistently high smoking rates within specific demographic groups in Korea, as well as in managing the growing concerns surrounding new types of tobacco products, such as e-cigarettes and HTPs, especially among younger populations.
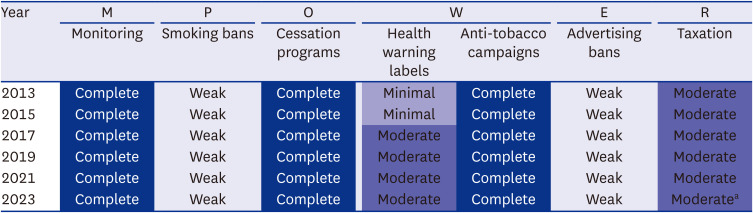
Table 3
The state of tobacco control policies in South Korea as measured by MPOWER measures (2013–2023)
Assessment scale consists of four levels: “Weak,” “Minimal,” ”Moderate,” and “Complete.”
aNo change in the trend of cigarettes affordability between 2012 and 2022.
Data source: Kong J, Lim S, Choi S, Kim G. Status and Challenges of Implementing Tobacco Control Policies in Korea: Focus on WHO MPOWER Measures. JKSRNT 2023;14:21-32.
World Health Organization. (2023). WHO report on the global tobacco epidemic, 2023: protect people from tobacco smoke. World Health Organization.
![]()
Go to :
EPIDEMIC FEATURES OF TOBACCO USE
Proliferation of novel tobacco products
There is a prevailing perception that “tobacco = cigarettes”, but today’s tobacco products are evolving rapidly. As of 2022, the prevalence of adult tobacco product use, which includes cigarettes, HTPs, e-cigarettes, and other tobacco products, stands at 22.1%. This represents a 4.4 percentage point increase (a 24.9% increase) from the previously calculated cigarette smoking rate of 17.7% (Table 2, Fig. 3). Specifically, the use of HTPs and e-cigarettes among Korean adults accounts for 5.9% and 3.5%, respectively. These numbers suggest that relying solely on cigarette smoking rates is no longer adequate to gauge the extent of the tobacco use epidemic, as they indicate that some populations use multiple tobacco products.
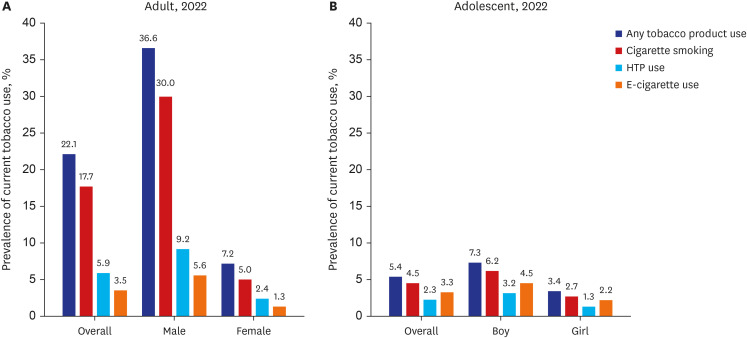 | Fig. 3Percentage of (A) adults aged 19 and older and (B) adolescents aged 13 to 18 who reported the current use of tobacco products, by type of product and sex (2022).HTP = heated tobacco product.
Data source for (A) adults: Korea Disease Control and Prevention Agency (2023), “Korea Health Statistics 2022: Korea National Health and Nutrition Examination Survey (KNHANES IX-1),” https://knhanes.kdca.go.kr/knhanes/sub04/sub04_04_01.do.
Data source for (B) adolescents: Korea Disease Control and Prevention Agency (2023), “18th Korea Youth Risk Behavior Survey,” https://www.kdca.go.kr/yhs/.
|
Notably, the prevalence of using any tobacco product is 36.6% in males (6.6 percentage points higher than the cigarette smoking rate of 30.0%; a 22.0% increase) and 7.2% in females (2.2 percentage points higher than the cigarette smoking rate of 5.0%; a 44.0% increase). The relative increase in the prevalence of overall tobacco product use compared to the prevalence of cigarette smoking was greater among women than men. The prevalence of HTP use was 1.6 to 1.8 times higher than the prevalence of e-cigarette use for both adult men and women. Specifically, the prevalence of HTP use was 9.2% for men and 2.4% for women, while the prevalence of e-cigarette use was 5.6% for men and 1.3% for women.
The prevalence of any tobacco product use among adolescents stands at 7.3% for male youth (1.1 percentage points higher than the cigarette smoking rate of 6.2%; a 17.7% increase) and 3.4% for female youth (0.7 percentage points higher than the cigarette smoking rate of 2.7%; a 25.9% increase). Contrary to results in adults, e-cigarette use was more common than HTP use among both male and female youth. Specifically, the prevalence of HTP use was 3.2% for male youth and 1.3% for female youth, while the prevalence of e-cigarette use was 4.5% for male youth and 2.2% for female youth. However, the greater concern is that the use of HTPs and e-cigarettes has continued to increase in recent years for male and female adolescents.
The evolution of tobacco products and dynamic changes in tobacco use behaviors pose additional challenges for tobacco control efforts in Korea. The landscape of tobacco consumption has undergone a significant transformation by expanding to include a diverse range of products that provide smokers with more choices. Instead of serving solely as a method for quitting smoking, this availability now leads to situations where individuals may use multiple tobacco products simultaneously, depending on circumstances or conditions.31 This suggests the need to develop targeted interventions for individuals who use multiple tobacco products concurrently.
Moreover, as tobacco products continue to evolve, ongoing research is essential to fully comprehend the potential health risks linked with new types of tobacco and nicotine products. Public health campaigns and educational initiatives should adapt by incorporating information about the risks associated with various tobacco products. Tobacco control policies should also be designed to respond sensitively and proactively to both novel tobacco products and traditional manufactured cigarettes. While traditional tobacco control approaches were designed with a focus on combustible cigarettes, the emergence of other alternatives necessitates a reevaluation and adaptation of existing strategies.32 In particular, legal and institutional improvements are needed to prevent regulatory blind spots, such as strengthening the management and regulation of synthetic nicotine, which cleverly avoids the definition of tobacco, and electronic devices designed for tobacco and nicotine use.33
Age disparities in tobacco use
While there has been an overall decline in the prevalence of cigarette smoking across most age groups between 1998 and 2022, notable age disparities persist in tobacco use in Korea (Table 2). Specifically, among men, the lowest prevalence of cigarette smoking was observed in individuals aged 70 and over, who had a smoking rate of 16.2%. The highest prevalence was noted among men in their 40s and 50s, with approximately 36.6% and 32.5% of men in these age brackets identified as current cigarette smokers. However, the use of newer types of tobacco products, such as e-cigarettes or HTPs, was more widespread among young adults. HTP use was prevalent among individuals in their 20s (13.5%), 30s (11.1%), and 40s (11.1%), while e-cigarette use was prevalent among those in their 20s (8.9%) and 30s (10.1%).
Age disparities were also evident among women. As of 2022, the lowest prevalence of cigarette smoking was among those aged 70 and over, at 0.6%. The highest prevalence was observed in women in their 20s, 30s, and 50s, with rates of 5.8%, 6.8%, and 6.1%, respectively. HTP use was widespread among women in their 30s (4.0%), 40s (3.2%), and 20s (2.9%), while e-cigarette use was prevalent among those in their 20s (4.2%).
Over the past two decades, an overall decline in the prevalence of cigarette smoking has been observed across all age groups for men. The decline in prevalence has been less significant for younger women than older women. In fact, in certain age groups, tobacco use has increased. Specifically, from 1998 to 2022, cigarette smoking prevalence increased for women in their 20s by 0.7 percentage points (a 13.7% increase) and for women in their 30s by 2.3 percentage points (a 51.1% increase).
These disparities in tobacco use across age groups underscore the challenges of promoting tobacco prevention and cessation within specific demographics and highlight the urgency of tailoring proactive programs to specifically target young adults and youth. In addition, there is a growing movement in several countries to raise the legal age to purchase cigarettes. The US has already raised this age by three years, and some countries have attempted to introduce smoke-free generation laws. Monitoring the success of these plans in other countries can provide insight into the potential benefits of raising the age of purchasing cigarettes in Korea, which is currently set to 19 years. Raising the minimum age to purchase tobacco could delay the onset of tobacco use among young people, including adolescents, potentially lowering long-term tobacco use and associated health risks.
Gender disparities in tobacco use
Historically, tobacco use has been more prevalent among Korean men, a pattern consistent with many other countries.16 The disparity in the prevalence of cigarette smoking between Korean men and women, which was 10.2 times (66.3% for men vs. 6.5% for women) in 1998, has decreased over time to 6.0 times (30.0% for men vs. 5.0% for women) in 2022 (Table 2). While the prevalence of cigarette smoking among Korean men has significantly declined over the past two decades, narrowing the gender gap, it remains significant. Compared to other countries, the prevalence of cigarette smoking among men in Korea has remained consistently high,6 while it has plateaued among women. With the spread of new types of tobacco products used by young women, the male-to-female ratio decreased to 5.1 for the prevalence of any tobacco product use, including cigarettes and novel tobacco products. Additionally, this ratio has further decreased to 4.3 for the prevalence of e-cigarette use and 3.8 for the prevalence of HTP use.
The average age of initiating cigarette smoking for women decreased from 29.4 years in 1998 to 22.6 years in 2022, indicating a notable difference of 6.8 years. In contrast, for men, the average age of initiation decreased by only 2.1 years, from 20.8 years in 1998 to 18.7 years in 2022. The significant decrease in the age at which women start smoking suggests a potential increase in the female smoking population; the only demographic in which cigarette smoking rates escalated during this timeframe was women in their 20s and 30s. Thus, while the overall smoking rate among Korean women appears to have plateaued, this reflects contrasting age-specific trends. Furthermore, the prevalence of any tobacco product use notably surged within these age groups due to the adoption of new types of tobacco products.
Previous studies have suggested that the smoking rate among Korean women may be underestimated.1534 Within the cultural context of Korea, where female smoking is viewed negatively, self-reported questionnaires are prone to underestimation. Indeed, the female smoking rate, determined through urinary cotinine levels, was approximately 2.6 times higher than the rate estimated by the KNHENES based on self-reporting.34 The potential underestimation of female smoking rates could result in the marginalization of female smokers in tobacco control policy efforts. The clear downward trend in adult male smoking rates over the past two decades suggests that tobacco control policies in Korea may have been more focused and effective for men. These findings call for gender-specific approaches to tobacco control policies that recognize the unique challenges and trends observed in men and women.
Young women and youth, who are potentially significant customers for tobacco companies, are the targets of aggressive marketing and face considerable vulnerabilities related to tobacco use. Therefore, they require intensive attention in prevention and cessation efforts. It is crucial to ensure that support services for tobacco cessation are accessible and tailored to the specific needs of young women. These services should address the unique challenges and motivations that influence young women’s smoking behavior, including social norms, the targeted marketing strategies of tobacco companies, and the impacts of tobacco use on maternal and reproductive health. As part of the comprehensive tobacco control measures, strict restrictions on the marketing, advertising, and promotion of tobacco products, especially those targeting girls and young women, should also be considered.
Disparities in tobacco use among individuals with disabilities
Current statistics on smoking rates among individuals with disabilities in Korea are not comprehensive and vary slightly depending on the definition used to identify disabilities, the survey method, and the data source. Additionally, variations in the inclusion or exclusion of specific disability types or severity levels can result in differing reported smoking rates. Therefore, it is crucial to interpret smoking prevalence data among people with disabilities cautiously.
According to the Healthcare Statistics of Persons with Disabilities from the Korea National Rehabilitation Center, among the people with disabilities who participated in the national health checkup in 2020, the overall smoking rate was recorded at 17.7%, which is lower than the 20.2% rate among those without disabilities.35 Similar to the general population, there was a significant gender disparity in smoking rates between males (26.8%) and females (2.5%). Additionally, significant variations were observed depending on the type of disability, with higher smoking rates noted among individuals with mental, facial, physical, and visual disabilities. Notably, men with mental disorders exhibited a particularly high smoking rate of 42.7%.
A previous study using data from the Panel Survey of Employment for the Disabled found that the smoking rate among people with disabilities was 1 to 2 percentage points lower than non-disabled people and that it was continuously decreasing.36 However, when examining smoking rates by the severity of disability, it was found that the milder the disability, the higher the smoking rate. Specifically, the smoking rate among individuals with grade 6 disabilities (the least severe) was 2.6 times higher than that of individuals with grade 1 disabilities (the most severe).
Another study comparing smoking rate trends between men with and without disabilities found that as of 2017, the age-standardized smoking rate for men with mild disabilities (43.0%) in the younger age group (20–49 years) was 1.16 times higher than that of non-disabled men (36.8%).37 The highest smoking rate was observed in men with physical disabilities in the younger age group. In the older age group (50 years and over), the highest smoking rate was among men with intellectual or psychological disabilities.
These notable disparities suggest that smoking cessation programs and interventions for people with disabilities should consider the unique needs and challenges faced by distinct subgroups, starting with the type and severity of the disability. These targeted efforts should consider the health vulnerabilities of people with disabilities, improve the accessibility and usability of smoking cessation programs, and develop targeted educational content and counseling. Crucial steps include ensuring the physical accessibility of organizations providing smoking cessation services, offering materials in additional formats (e.g., braille, large print, or audio), and providing assistive technologies to aid communication. Additionally, individuals with cognitive disabilities might benefit from simplified instructions and repeated follow-up, while those with physical disabilities may need guidance on managing stress and nicotine cravings without exacerbating their condition. Reducing smoking rates in this population is crucial for improving their health outcomes and quality of life while preventing secondary conditions. In turn, these strategies will promote health equity in public health.
Mortality and disease burden due to smoking in Korea
Tobacco contains more than 8,000 chemicals, many of which are known to be carcinogenic and exhibit toxic, cytotoxic, genotoxic, mutagenic, and teratogenic properties.3839 The tobacco epidemic is a significant public health issue that substantially impacts health and life by increasing the prevalence of cardiovascular disease (CVD), cancer, chronic respiratory disease, and respiratory infections, making it a leading cause of preventable mortality globally.
In 2019, smoking tobacco products accounted for 7.69 million deaths worldwide and 200 million disability-adjusted life years (DALYs). It was the leading risk factor for death among males, responsible for 20.2% of all male deaths. Of the 7.69 million deaths attributable to smoking, 6.68 million (86.9%) were current smokers.19 Additionally, considering the estimated 1.3 million deaths in non-smokers due to second-hand smoke exposure, tobacco kills more than 8 million people prematurely worldwide each year.2640 At the global level, tobacco-related deaths in 2019 were mainly attributed to CVD (36.7%), cancer (29.9%), chronic respiratory disease (20.6%), and respiratory infections (7.0%). Despite efforts to curb tobacco use, the global disease burden related to tobacco remains high in many countries,40 including Korea.
According to the KDCA and Cho et al. report, as of 2019, the total number of deaths attributed to direct smoking in Korea was 58,036, averaging approximately 159 deaths per day.941 Deaths directly related to smoking accounted for 32.3% of all reported deaths in men and 5.3% in women. Current male smokers have a 70% higher likelihood of death compared to non-smoking men. Similarly, for women, smoking increases the risk of death by 80%. For former smokers, the risk of death increases by 1.1 times for men and 1.3 times for women.
The economic costs of tobacco use are substantial. They include significant healthcare costs for treating diseases caused by tobacco use as well as the lost human capital resulting from tobacco-attributable morbidity and mortality.26 Using the cost of illness approach, the socioeconomic cost of smoking in Korea in 2019 was estimated to be 12,191.3 billion KRW, approximately 16.8% of the total expenditure of the Korean Ministry of Health and Welfare (72.5 trillion KRW in 2019). In detail, this cost includes 4,619.2 billion KRW for the medical treatment of smokers' diseases, transportation costs, and nursing care; 1,111.5 billion KRW for productivity loss during the period of medical service use; and 6,460.6 billion KRW for productivity loss due to the premature death of smokers.9
Tobacco use brings suffering, disease, and death. It also impoverishes families and national economies, contributing to poverty by diverting household spending from basic needs such as food and shelter to tobacco. This creates a vicious cycle of poverty and poor health, especially among low-income families.26 Treating diseases caused by tobacco use places a substantial financial burden on healthcare systems. In many countries, a significant portion of healthcare budgets is consumed by tobacco-related diseases that divert resources from other essential health services. Additionally, tobacco use results in a loss of productivity for businesses and the economy as a whole due to the illness, disability, and premature death of individuals.42 As the review thus far demonstrates, the socioeconomic impacts of tobacco use are profound and multifaceted, affecting individuals, families, communities, and societies at large.
Go to :
DISCUSSION AND CONCLUSION
This research aimed to provide an updated overview of the epidemiology of tobacco use in Korea, highlight Korea’s progress in tobacco control, and emphasize the emerging challenges associated with tobacco use and control policies. There was a notable decrease in the prevalence of tobacco smoking in adults over the past quarter-century, particularly in men. This positive trend reflects the efforts of public health initiatives aimed at reducing smoking and mitigating associated health risks. However, the dynamic landscape of the tobacco epidemic, including the emergence of novel tobacco and nicotine products and their evolving usage patterns, presents additional challenges for tobacco control efforts. While the smoking rates for traditional cigarettes may continue to decrease, the use of alternative tobacco products, such as e-cigarettes and HTPs, as well as the use of multiple tobacco products, may increase.
Tobacco companies often employ sophisticated marketing and product development strategies to promote novel tobacco products as less harmful or safer alternatives. To effectively counter these industry tactics, ensure accurate public health messaging, and promote informed decision-making, public health organizations and policymakers must continuously monitor and gather scientific evidence regarding the short-term and long-term health impacts of these products. To ensure that there are no regulatory blind spots, tobacco control policies should be designed to proactively address both novel tobacco products and traditional cigarettes.
Age- and gender-specific variations in tobacco use reveal changing behaviors across the lifetime of the Korean population. The age at which individuals begin using tobacco is decreasing, and the cigarette smoking rate is now highest among men in their 40s and 50s and among women in their 20s and 30s. Historically, the cigarette smoking rate among women was highest in older age groups; however, this trend has now completely reversed. Additionally, new tobacco products, such as HTPs and e-cigarettes, are gaining traction among young adults and adolescents. Understanding these features and variations of tobacco use across demographics is crucial for tailoring cessation and prevention efforts to specific populations and age groups. Addressing the significant disparities in tobacco use that persist among specific demographic groups, including young women, adolescents, and socially disadvantaged groups, such as persons with disabilities, remains a critical public health priority in Korea.
Korea is approaching the 20th anniversary of its ratification of the WHO FCTC, a global public health treaty aimed at combating the tobacco epidemic. This milestone presents an opportune moment to reflect on Korea’s progress in tobacco control over the past decades. The WHO has conducted six previous assessments of Korea’s tobacco control policies, measured by the MPOWER framework, which have quantified both the achievements and shortcomings in the implementation of Korea’s tobacco control policies. Korea has consistently received “complete” evaluations in “Monitoring tobacco use and prevention policies (M),” “Offering help to quit tobacco use (O),” and “Warning about the dangers of tobacco (through conducting anti-tobacco campaigns) (W).” However, policies concerning “Protecting People from Tobacco Smoke (P)” and “Enforcing Bans on Tobacco Advertising, Promotion, and Sponsorship (TAPS) (E)” have consistently been rated as “weak.”
To protect against exposure to tobacco smoke (P), establishing completely smoke-free public places is a key criterion for evaluation. However, in Korea, the allowance of smoking rooms within designated smoke-free areas does not meet the standards set by the FCTC for fully smoke-free environments. Despite this limitation, efforts to expand smoke-free areas are ongoing. Previously, smoke-free zones were designated to extend 10 meters from the boundaries of daycare centers and kindergartens and were limited to the premises of elementary, middle, and high schools. With the revision of the National Health Promotion Act, smoke-free zones around kindergartens and daycare centers have been expanded to 30 meters, and a 30-meter smoke-free zone has also been newly designated around elementary, middle, and high school facilities. To eliminate exposure to second-hand smoke and ensure that more public places become completely smoke-free, it remains essential to continuously expand smoke-free zones and implement stricter regulations on smoking rooms.
In Korea, regulations on TAPS remain an area of tobacco control requiring immediate improvement and further efforts. A comprehensive ban on both direct and indirect TAPS, as outlined in the guidelines to Article 13 of the WHO FCTC, can effectively protect individuals, particularly young people, from the marketing tactics of the tobacco industry. The implementation of TAPS regulations is considered “complete” if all forms of direct and indirect tobacco advertising are fully regulated or if policies prohibiting tobacco advertising, sales promotions, and sponsorship activities by tobacco companies cover at least 90% of the population.43 However, Korea still allows tobacco advertising in magazines and retail stores, as well as promotional activities on international aircraft and passenger ships, and sponsorship of social, cultural, art and sports events. For TAPS bans to be effective, they must be comprehensive, covering all marketing categories without exceptions or loopholes. Otherwise, the tobacco industry may redirect resources to unregulated marketing channels, including those promoting new tobacco products. Recently, the diversification of the media environment has led to the emergence of various promotional methods that extend beyond the current scope of regulation. Regarding sponsorship channels, various approaches are being employed, including direct sponsorship, sponsorship through independent corporations, and indirect sponsorship via third-party organizations. Therefore, it is crucial to fully understand the scope and operation methods of these advertising, promotion, and sponsorship activities, and to conduct a systematic review of the extent and adequacy of existing regulations.44 It is imperative to expedite comprehensive regulations on TAPS, as this area has been vulnerable to regulatory gaps thus far in Korea.
Moreover, the evaluation of another component of the “Warning about the Dangers of Tobacco (W)” policy—health warnings on tobacco product packaging—along with the “Raising Taxes on Tobacco (R)” policy, was assessed at a “moderate” level, without reaching the “complete” level. Notably, the “Raising Taxes on Tobacco (R)” policy has remained at a “moderate” level since 2013, with no increases in tobacco taxes implemented for several years. The total tax rate on cigarettes in Korea is 73.8% of the retail price, nearing the 75% tax share recommended by the FCTC. However, this rate has remained unchanged for nearly a decade. Additionally, the taxation rates for HTPs (66.8%) and e-cigarettes (41.9%) are significantly lower than those for conventional cigarettes.45 Currently, the price of a pack of cigarettes (20 sticks) in Korea remains at 4,500 won (USD 3.45), a level set by a 2015 tax increase. In 2022, this price ranked as the fifth lowest among the 38 OECD countries, following Colombia (USD 1.63), Turkey (USD 1.76), Costa Rica (USD 2.98), and Mexico (USD 3.44), and represented only 14.8% of the price in Australia (USD 23.26), which had the highest cigarette price.46 New Zealand (USD 19.83), Ireland (USD 16.11), Norway (USD 15.38), the United Kingdom (USD 12.67), and Iceland (USD 11.35) also had high cigarette prices. While smoking rates were not universally inversely proportional to cigarette prices across all countries, those with high cigarette prices—such as Australia, New Zealand, Norway, and Iceland—reported significantly lower smoking rates, ranging from 5.7% to 8.5% in 2022–2023, compared to 14.7% in Korea.47 Significant increases in tobacco excise taxes and prices are recognized as the most effective and cost-efficient measure to reduce tobacco use. However, consumer purchasing power for tobacco products has increased in Korea, which appears inconsistent with a comprehensive strategy for reducing tobacco use. The tobacco taxation policy should be revised to reduce affordability by accounting for the effects of inflation and economic growth. Additionally, a simplified tax structure that does not differentiate based on tobacco product types should be adopted to discourage consumers from shifting to cheaper brands.48 There is an urgent need to evaluate whether the current tobacco price in Korea is adequate to deter tobacco use and consider whether further price increases are necessary.
In conclusion, Korea has made significant progress in reducing the prevalence of tobacco use, driven by the impact of expanded tobacco control policies and public health initiatives. These efforts have contributed to a gradual decline in smoking rates and have reflected the nation’s commitment to safeguarding public health. However, substantial challenges remain. It is crucial to expedite the comprehensive implementation of the WHO FCTC measures to address the shortcomings in each MPOWER field and further reduce the ongoing prevalence of tobacco use, related health disparities, and their adverse health and socioeconomic consequences. Prioritizing the strengthening of enforcement for the “Protecting People from Tobacco Smoke (P)” and “Enforcing Bans on Tobacco Advertising, Promotion, and Sponsorship (E)” components of the MPOWER framework—both consistently identified as weak—should be central to ensuring a more effective tobacco control strategy. To advance to the next level in tobacco control policies, it is essential for Korea to proactively adapt to changes in the policy environment surrounding tobacco regulation through a joint, multisectoral response involving health authorities, policymakers, and civil society. Through such coordinated efforts, Korea can effectively mitigate the ongoing public health burden posed by tobacco use.
Go to :
 XML Download
XML Download