

 PDF
PDF Citation
Citation Print
Print



Introduction
Background/rationale
According to the 2020 World Drug Report [1], the number of deaths due to opioid overdose has increased by 2.5
times, rising from 18,515 in 2007 to approximately 47,000 in 2018. A significant
aspect of the current overdose crisis is the growing addiction to prescription
narcotics [2]. Among patients prescribed
narcotics for chronic pain, 21%–29% misuse them, and 8%–12%
develop an addiction to these drugs [3].
In recent years, there has been a growing public awareness of the severity of
addiction to prescription narcotics [4].
Narcotic abuse can be defined in various ways; for example, MedlinePlus defines
prescription narcotic abuse as "taking medicine in a way that is
different from what the doctor prescribed" [5]. The primary cause of narcotics abuse is often a strong
desire to obtain more narcotics than those prescribed by doctors, driven by a
"strong desire or urge to use the substance" [6]. To combat prescription narcotic use
disorder (NUD), the Centers for Disease Control and Prevention (CDC) in the
United States has issued guidelines for prescribing narcotics [7]. Most states now mandate the registration
of narcotic users through prescription drug monitoring programs (PDMPs), which
track narcotic prescriptions [8].
According to the CDC guidelines, prescribing a morphine milligram equivalent
(MME) per day of ≥90 as the morphine equivalent daily dose (MEDD) should
be minimized as much as possible [7]. Some
studies have indicated that this system has decreased the prevalence of NUD and
its sequelae [9,10], but a recent review has reported ambiguous results
[11].
A limitation of the CDC guideline and PDMP is that they can only detect the risk
of NUD, not NUD itself. Furthermore, the cut-off values for the NUD high-risk
indexes are not definitive standards for identifying patients at risk of NUD.
For instance, the MEDD restriction cut-off varies significantly between
countries: it is 90 MME/day in the USA and 200 MME/day in Canada [12]. Although numerous studies have sought
to develop tools to predict NUD, these tools primarily focus on analyzing
high-risk factors rather than detecting NUD itself [13,14]. Therefore,
there is a need to develop a method that can definitively identify abnormal
prescription patterns indicative of NUD.
Hence, in this study, we developed a method to screen for patients with NUD by
directly applying the definition of prescription narcotic abuse to analyze
extensive real-world clinical data. Patients employing multiple strategies to
obtain additional narcotics may have an actual MEDD that exceeds the
doctor's intended MEDD due to overlapping prescriptions. To address this,
we introduced a weighted (wt)-MEDD score. This score is calculated based on the
number of prescription dates where the MEDD ratio ([actual MEDD]/[intended
MEDD]) was above a certain level (for example, 1.5), suggesting the presence of
NUD, as per the criteria for prescription narcotics abuse.
Methods
Ethics statement
This study received approval from the Institutional Review Board (IRB) of Seoul
National University Hospital (IRB No. 1806-182-955) and adhered to the ethical
standards established in the 1964 Declaration of Helsinki. The requirement for
informed consent was waived because the study was based on database
analysis.
Study design
This retrospective cohort study employed real-world data to develop detection
methods based on a defined criterion for narcotic abuse. The study adhered to
the guidelines outlined in the STrengthening the Reporting of OBservational
studies in Epidemiology (STROBE) statement, which can be accessed at: https://www.strobe-statement.org/.
Setting
This study evaluated the total narcotics prescriptions from July 2000 to June
2018 at a single large hospital. Prescriptions for patients with cancer and for
inpatients were excluded from the analysis. The analysis focused on the
following 12 narcotics: fentanyl, hydrocodone, hydromorphone, morphine,
oxycodone, oxycodone/naloxone, tapentadol, alfentanil, meperidine, remifentanil,
buprenorphine, and nalbuphine. Low-dose narcotics such as codeine and tramadol
were excluded from the study.
Most patterns of NUD involve taking higher doses than those intended by doctors.
The hypothesis was that a patient at risk of developing NUD would employ
multiple strategies to achieve a higher MEDD, resulting in a discrepancy between
the MEDD intended by the doctors and the overlapping MEDD that the patient
achieves through these strategies. Consequently, the MEDD ratio is defined as
follows (Fig. 1A):
Fig. 1.
Schematic diagram of the calculation of the weighted MEDD score. MEDD, morphine equivalent daily dose; wt-MEDD, weighted MEDD.
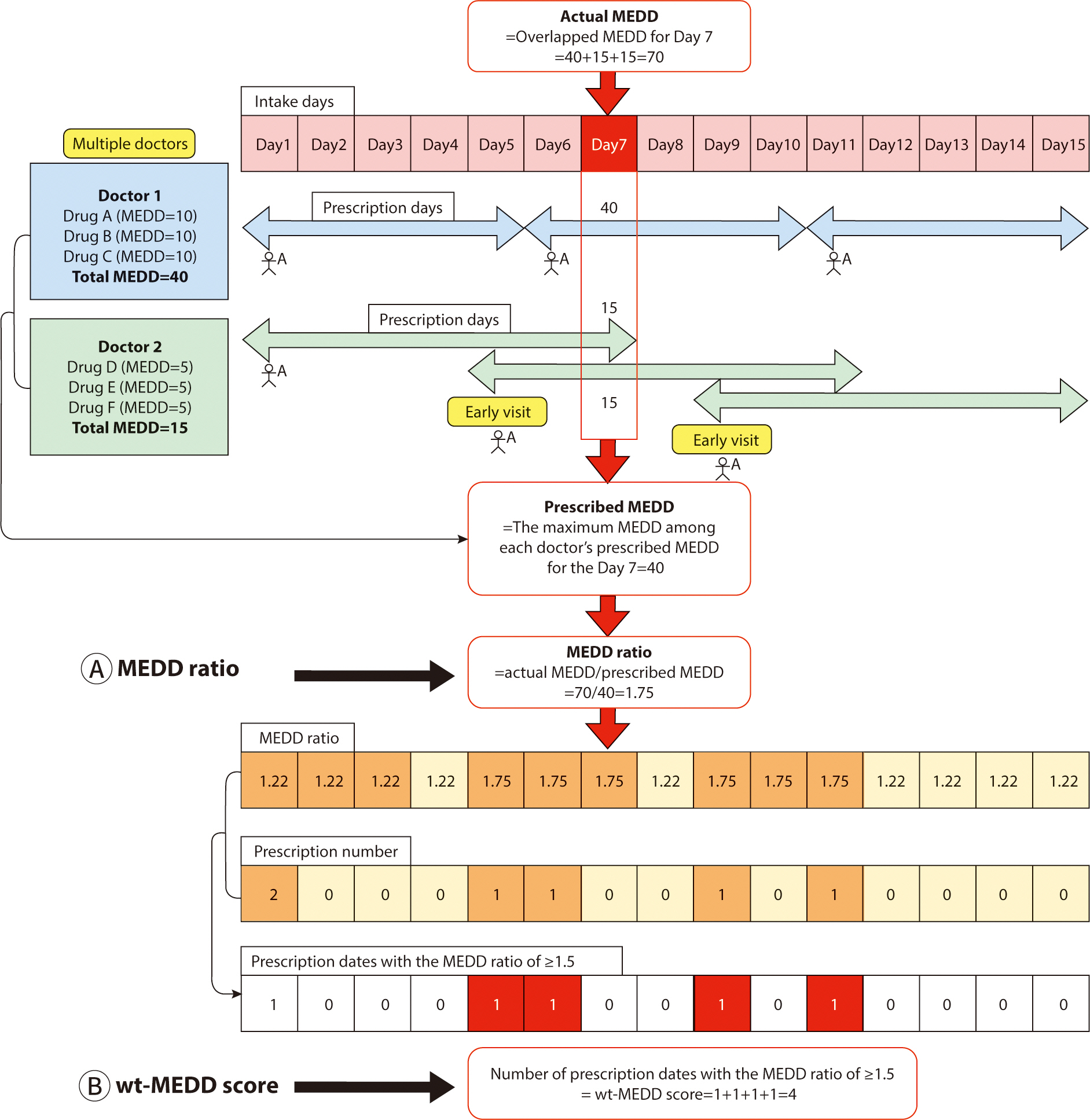
For example, doctor 1 prescribes 40 MEDD to patient A, deeming it an appropriate
dosage. However, patient A subsequently visits Doctor 2 to obtain an additional
prescription for narcotics. Unaware of the previous prescription from Doctor 1,
Doctor 2 prescribes an additional 15 MEDD, considering it suitable for patient
A. Later, patient A returns to doctor 2 before the scheduled follow-up, claiming
to have lost the previous prescription, and receives another 15 MEDD.
Consequently, patient A ends up receiving a total of 70 MEDD of narcotics, which
is 1.75 times the highest intended dose of 40 MEDD prescribed by the doctors.
The MEDD ratio, defined as the ratio between the actual MEDD received and the
maximum intended MEDD prescribed by the doctors, is thus 1.75 in this scenario
(Fig. 1A).
We defined the wt-MEDD score as follows (Fig.
1B):
In Fig. 1, patient A consults doctor 1 on
days 1, 6, and 11, and sees doctor 2 on days 1, 5, and 9. This results in a
total of five prescription dates for patient A (days 1, 5, 6, 9, and 11). Out of
these, the number of dates where the MEDD ratio is ≥1.5 amounts to four
(day 5, 6, 9, and 11). The wt-MEDD score, which is defined as the number of
prescription dates with a MEDD ratio of ≥1.5, is therefore 4, as shown in
Fig. 1B. If patient A persists in
obtaining narcotics prescriptions from multiple doctors and visiting them
earlier than scheduled, the wt-MEDD score will continue increasing.
The choice of a MEDD ratio of 1.5—higher than 1.0 but lower than
2.0—was made to accommodate minor discrepancies between the intended MEDD
prescription by doctors and the actual MEDD, such as during initial dose
adjustments at the start of narcotic prescriptions. This range also effectively
identifies abnormal prescriptions that require further review. Ratios below 1.5
may be overly sensitive, failing to distinguish significant deviations between
the actual and intended MEDD. Institutions can adjust the cut-off MEDD ratio
based on their preferences, opting for less than 1.5 to increase sensitivity or
more than 1.5 to increased specificity. The wt-MEDD score served as a proxy for
NUD because repeated prescriptions with a high MEDD rate suggest that the
patient is consistently receiving more narcotics than originally prescribed by
the physician.
We investigated the clinical applicability of the wt-MEDD score, specifically to
monitor abnormal narcotics prescription patterns in a hospital setting. It is
necessary to identify both the doctors and patients involved in these practices
and to provide them with feedback. To this end, we utilized the wt-MEDD score to
compile lists of doctors and patients associated with abnormal prescription
patterns. We identified doctors with outlier wt-MEDD scores and similarly
generated a list of patients exhibiting outlier scores to closely monitor their
prescription behaviors. These individuals were characterized by a two-tailed
P-value of <0.001, corresponding to a Z score of ≥3.29 or
≤–3.29. We then extracted the lists of doctors and patients with
these outlier wt-MEDD scores and determined the cut-off score for both groups to
effectively monitor and address abnormal narcotics prescribing patterns.
Second, we examined whether the wt-MEDD score could be utilized to identify
patients with NUD at an earlier stage. Our analysis focused on determining the
optimal cut-off value of the wt-MEDD score for detecting patients diagnosed with
NUD by physicians, aiming for the highest sensitivity and specificity. If the
cut-off value demonstrated high sensitivity and specificity, and if it was
reached before the doctors' diagnosis of NUD, it could serve as an early
indicator for NUD detection. A list of patients diagnosed with NUD by doctors
was extracted from the clinical data warehouse using the codes from the 10th
revision of the International Statistical Classification of Disease and Related
Health Problems (ICD-10) and diagnostic terms in the doctors’ medical
chart. The accuracy of the NUD diagnoses was verified by ensuring that the chart
records met the diagnostic criteria outlined in the DSM-IV-TR or DSM-V. We
selected only those patients who had been repeatedly prescribed narcotics at our
hospital prior to their NUD diagnosis. Patients diagnosed with NUD at other
hospitals, who had little or no history of narcotics prescriptions at our
facility, were excluded. Two physicians reviewed the electronic medical record
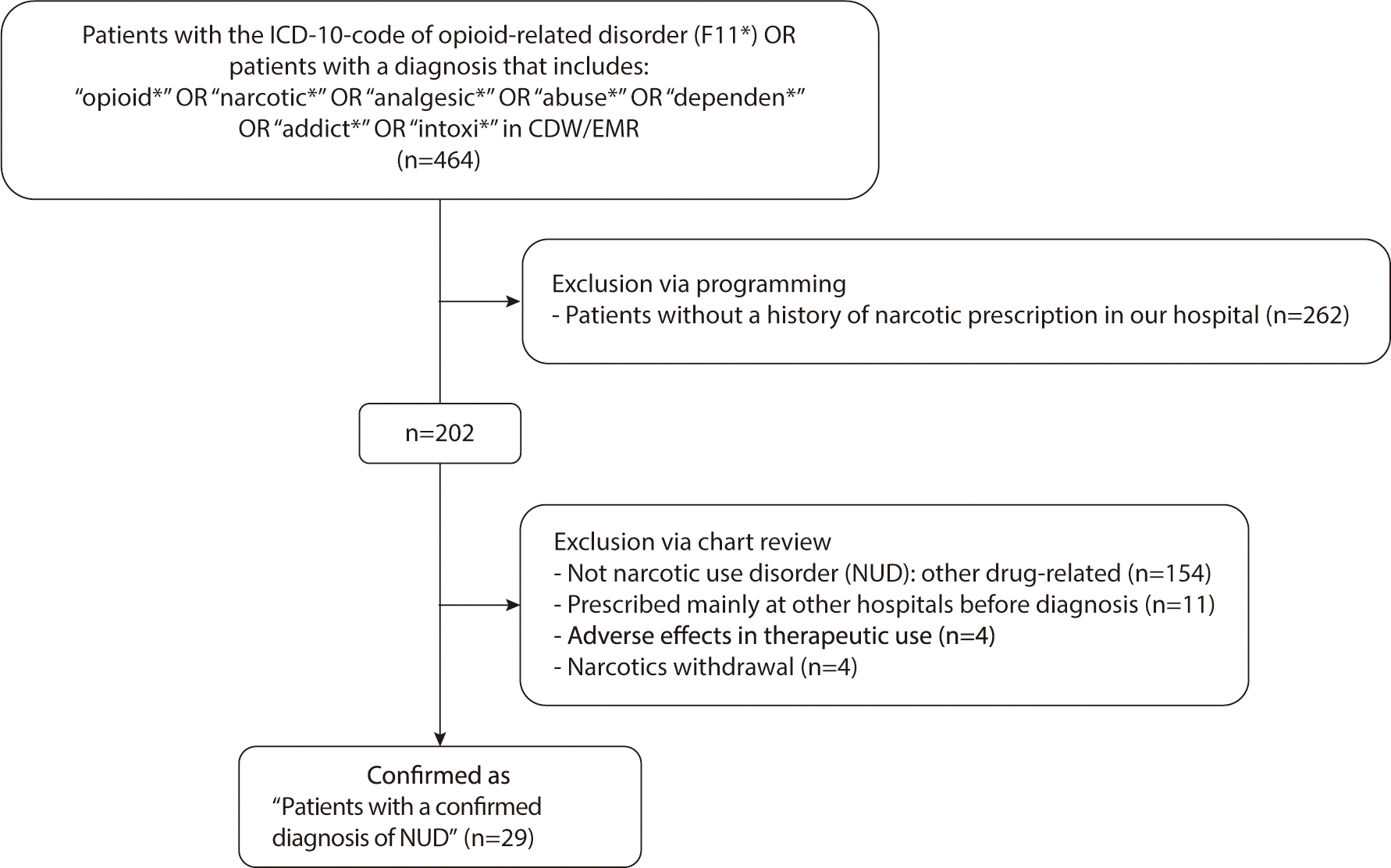
charts to confirm the accuracy of the diagnoses (Fig. 2). Any prescriptions issued to these patients after their NUD
diagnosis were omitted from the analysis.
Fig. 2.
Flowchart of patient screening and enrollment. ICD, International Classification of Diseases; CDW, clinical data warehouse; EMR, electronic medical records.
We also analyzed the optimal cut-off values, sensitivity, and specificity of
other high-risk NUD indexes (such as the PDMP monitoring categories) and their
combinations to confirm the effectiveness of the wt-MEDD score. To determine
whether the differences in sensitivity and specificity between the wt-MEDD score
and other indexes were statistically significant, the McNemar test was
performed.
We observed the time points at which the cut-off values of the wt-MEDD score and
other NUD high-risk indexes were reached, as well as the time points at which
NUD was diagnosed by a doctor in a patient case. This investigation aimed to
determine whether the wt-MEDD score cut-off value could be used to identify NUD
earlier. The paired t-test was employed to compare the mean time from the first
prescription of narcotics to the point of reaching the wt-MEDD score cut-off
value and the subsequent NUD diagnosis by doctors.
Participants
We analyzed the narcotic prescriptions of 221,887 patients, which were prescribed
by 8,737 doctors from July 2000 to June 2018.
Variables (study outcomes)
Considering the definition of narcotic abuse and the conditions of PDMP
monitoring, the wt-MEDD score and NUD high risk indexes (MEDD, prescription
days, prescribing frequency and duration, number of prescribing doctors, and
number of early receipt of narcotics before the scheduled visit) were selected
for analysis.
Data sources
A clinical data warehouse is a near-real-time database that consolidates data
from various clinical sources. A web-based browser facilitated the extraction of
a list of patients who met the inclusion criteria, along with their
corresponding electronic medical records. Information regarding the prescribed
patients was downloaded from the clinical data warehouse into five tables: basic
information, narcotic prescription, admission, surgery, and diagnosis
records.
Measurements
We calculated the activity of each narcotic based on its mode of
administration—tablet, patch, or injection. The table included
information on the MME conversion factor, derived from PDMP supplements [15]. The MEDD is calculated by multiplying
the MME conversion factor by the daily dose. When MME conversion factor
information for a specific drug was not available, we estimated it from the
relevant literature [16].
Among the five types of downloaded tables, the narcotic prescription table
included information such as the name of the prescribed drug, the date of
prescription, the number of days prescribed, and the MEDD (Supplement 1). To
calculate the overlapping MEDD for a specific intake date, a new table was
created. This table transformed each intake date for a patient into individual
rows—not just the prescription dates—by reformatting the data from
the prescription table (Supplement 2).
A 3-month interval was established as the measurement period for the time-series
analysis, specifically January-March, April-June, July-September, and
October-December. The total number of prescriptions issued during each 3-month
period was calculated. To analyze temporal changes in MEDD per patient, the
highest MEDD recorded in each 3-month interval was identified and compared with
the highest MEDDs from the other intervals.
Study size
Sample size estimation was not performed because this study included all target
participants.
Statistical methods
R (R Foundation for Statistical Computing, Vienna, Austria; URL: http://www.R-project.org/, ver. 3.6.0) and RStudio (RStudio,
Boston, MA, USA; URL: http://www.rstudio.com/,
ver. 1.2.1335) were used for statistical analyses. The ‘dplyr’
package in R was used to analyze data, and the ‘ggplot2’ package
was used to generate graphs. Outlier analysis was performed using the
‘outliers’ package. Cut-off value, sensitivity, specificity, and
accuracy were calculated using the ‘pROC’ package. A two-tailed
P-value of less than 0.05 was considered statistically significant.
Results
Patient and doctor outliers of the weighted morphine equivalent daily dose score
This study included 221,887 patients who received prescriptions for narcotics,
written by 8,737 doctors, totaling 555,097 narcotic prescriptions. Upon
reviewing the records of 464 patients diagnosed with NUD in the CDM, only 29
were confirmed to have NUD following repeated narcotic prescriptions at our
hospital. The majority of patients were diagnosed with NUD at other hospitals
before being transferred to our facility (Fig.
2).
The cut-off wt-MEDD score for patient outliers (n=996) was 10.5 (P<0.001).
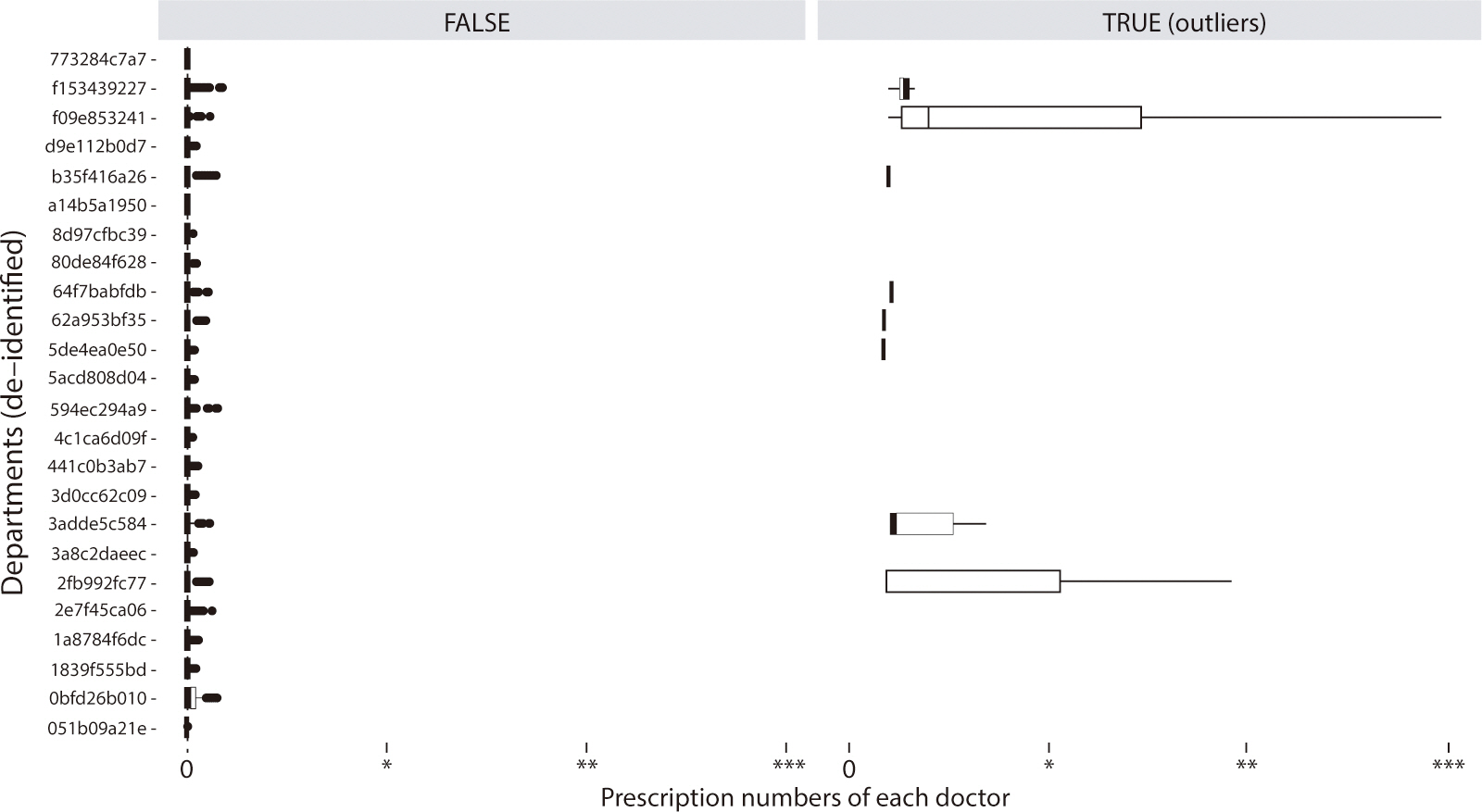
The list of doctor outliers (n=23) for the wt-MEDD score can be found in Supplement 3 and Fig. 3. This list, which included both
doctors and patients, was extracted and provided to the hospital committee to
monitor prescription abnormalities and offer feedback to the involved
doctors.
Comparison of the weighted morphine equivalent daily dose score and narcotic use disorder high risk indexes in detecting diagnosed cases of narcotic use disorder
Table 1 compares the wt-MEDD scoring
system with NUD high-risk indexes for detecting diagnosed NUD. The optimal
cut-off value for the wt-MEDD score, which demonstrated the highest sensitivity
and specificity, was ≥10.5. This value was similar to the cut-off for
outlier wt-MEDD scores (P<0.001). The median wt-MEDD score among the 29
patients diagnosed with NUD was 52 (25th–75th quartiles=25–115),
indicating that most patients with NUD had multiple prescriptions with a high
MEDD ratio, exceeding the intended prescription level. When compared to other
NUD high-risk indexes, the wt-MEDD score exhibited the highest sensitivity and
specificity (100.0% and 99.6%, respectively; Table 1). The McNemar test revealed that the sensitivity and
specificity of the wt-MEDD score were significantly superior to those of other
indexes (P<0.001), with the exception of two indexes: the quarterly
number with a doctor number of ≥4 and the number of prescriptions
≥10 days earlier than the scheduled visit (Table 1).
Table 1.
Comparison of the performance of various indices for detecting patients diagnosed with NUD
| Indexes | Cut-off | Sensitivity (%) | Specificity (%) | Accuracy (%) | McNemar’s P-value |
|---|---|---|---|---|---|
| MEDD | |||||
| wt-MEDD score (*) | 10.5 | 100.0 | 99.6 | 99.6 | Reference |
| Highest overlapping MEDD (1) | 52.25 | 100.0 | 95.6 | 95.6 | <0.001 |
| Number of prescriptions with intended MEDD ≥50 | 10.5 | 93.1 | 99.3 | 99.3 | <0.001 |
| Number of prescriptions with intended MEDD ≥90 | 6.5 | 93.1 | 99.0 | 99.0 | <0.001 |
| Frequency & duration | |||||
| Total prescription number (2) | 15.5 | 100.0 | 98.8 | 98.8 | <0.001 |
| Total number of quarter | 5.5 | 89.7 | 98.4 | 98.4 | <0.001 |
| Highest prescription number per quarter1) for all prescription periods | 4.5 | 100.0 | 97.1 | 97.1 | <0.001 |
| Prescription day | |||||
| Number of prescriptions with ≥14 prescription days at once | 11.5 | 89.7 | 99.5 | 99.5 | <0.001 |
| ≥30 days at once (3) | 0.5 | 62.1 | 98.3 | 98.3 | <0.001 |
| ≥60 days at once | 1.5 | 27.6 | 99.7 | 99.7 | <0.001 |
| ≥90 days at once | 3.5 | 13.8 | 100.0 | 99.9 | <0.001 |
| Number of doctors | |||||
| Total number of doctors (4) | 6.5 | 96.6 | 98.7 | 98.7 | <0.001 |
| Quarterly number with doctor number of ≥4 | 0.5 | 93.1 | 98.3 | 98.3 | 0.107 |
| Highest number of doctors per quarter1) for all prescription periods | 2.5 | 96.6 | 96.3 | 96.3 | <0.001 |
| Early prescription | |||||
| Number of prescriptions ≥1 day earlier than the scheduled visit | 1.5 | 93.1 | 99.1 | 99.1 | <0.001 |
| ≥2 days earlier | 0.5 | 89.7 | 98.6 | 98.6 | <0.001 |
| ≥3 days earlier | 0.5 | 89.7 | 98.8 | 98.8 | <0.001 |
| ≥4 days earlier | 1.5 | 86.2 | 99.5 | 99.5 | <0.001 |
| ≥5 days earlier | 1.5 | 86.2 | 99.5 | 99.5 | <0.001 |
| ≥6 days earlier | 1.5 | 86.2 | 99.6 | 99.6 | <0.001 |
| ≥7 days earlier (5) | 0.5 | 86.2 | 99.1 | 99.1 | <0.001 |
| ≥10 days earlier | 1.5 | 82.8 | 99.7 | 99.7 | 0.548 |
| ≥14 days earlier | 0.5 | 82.8 | 99.5 | 99.5 | <0.001 |
| Combination of methods | |||||
| (1) ∩ (2) ∩ (4) (triple-test) | 96.6 | 99.5 | 99.5 | <0.001 | |
| (1) ∩ (2) ∩ (3) ∩ (4) | 58.6 | 99.8 | 99.8 | <0.001 | |
| (1) ∩ (2) ∩ (3) ∩ (5) | 82.8 | 99.8 | 99.8 | <0.001 | |
| (1) ∩ (2) ∩ (3) ∩ (4) ∩ (5) | 58.6 | 99.9 | 99.9 | <0.001 | |
| ((1) ∩ (2) ∩ (3) ∩ (4)) ∪ ((1) ∩ (2) ∩ (3) ∩ (5)) | 82.8 | 99.8 | 99.8 | <0.001 | |
| (1) ∩ (2) ∩ (4) ∩ (*) | 96.6 | 99.7 | 99.7 | <0.001 | |
| (1) ∩ (2) ∩ (3) ∩ (4) ∩ (*) | 58.6 | 99.9 | 99.9 | <0.001 | |
| (1) ∩ (2) ∩ (3) ∩ (5) ∩ (*) | 82.8 | 99.8 | 99.8 | <0.001 | |
| (1) ∩ (2) ∩ (3) ∩ (4) ∩ (5) ∩ (*) | 58.6 | 99.9 | 99.9 | <0.001 | |
| (((1) ∩ (2) ∩ (3) ∩ (4)) ∪ ((1) ∩ (2) ∩ (3) ∩ (5))) ∩ (*) | 82.8 | 99.8 | 99.8 | <0.001 |
To improve the ability to detect NUD, we combined the NUD high-risk indexes with
the wt-MEDD score and assessed their sensitivity and specificity. A combined
model that included the highest overlapping MEDD, total number of prescriptions,
and total number of doctors (triple-test) demonstrated excellent sensitivity and
specificity, at 96.6% and 99.5% respectively. When the wt-MEDD score was used in
conjunction with the triple-test, the sensitivity and specificity further
improved to 96.6% and 99.7%, respectively. These results suggest that the
wt-MEDD score, when combined with other NUD high-risk indexes, is effective for
screening patients with NUD (Table
1).
Comparison of time points of reaching the weighted morphine equivalent daily dose score cut-off value and that of the narcotic use disorder diagnosis
In all 29 patients diagnosed with NUD, the time point at which the wt-MEDD
cut-off score was reached occurred earlier than the time point of the
doctor's initial diagnosis of NUD. The average time to reach the wt-MEDD
cut-off score was 1,024 days (median [quartile 1–quartile 3], 361
[192–2,323]) from the first narcotics prescription. In contrast, the
average time until NUD diagnosis was 2,578 days (median [quartile
1–quartile 3], 2,342 [1,396–4,030]). This resulted in an average
difference of 1,554 days (95% CI, 1,096–2,010 days, paired t-test,
P<0.001).
Patient case report
To provide an example of the clinical application of the new methodology (wt-MEDD
score) in identifying cases of NUD, we selected a patient diagnosed with NUD who
employed multiple strategies to obtain a higher number of narcotics
prescriptions. We retrospectively observed the time-sequential changes in the
wt-MEDD score and the NUD high-risk indexes for this patient up until the NUD
diagnosis was made (Fig. 4). Fig. 4A demonstrates a gradual increase in
the patient's wt-MEDD score over time. Initially, the score was 10 in
November 2011, and the patient received a diagnosis of NUD in October 2017. If
the wt-MEDD score had been utilized as a screening tool for this patient, it
could have potentially led to a diagnosis of NUD 6 years earlier.
Fig. 4.
Temporal changes in various NUD high risk indices for patients diagnosed with NUD. (A) wt-MEDD, (B) highest actual and intended MEDD every 3 months, (C) highest prescription days every 3 months, (D) total number of prescriptions every 3 months, (E) total number of prescribing doctors every 3 months, (F) number of early receipt of narcotics before ≥7 days for every 3 months. MEDD, morphine equivalent; wt-MEDD, weighted MEDD; NUD, narcotic use disorder.
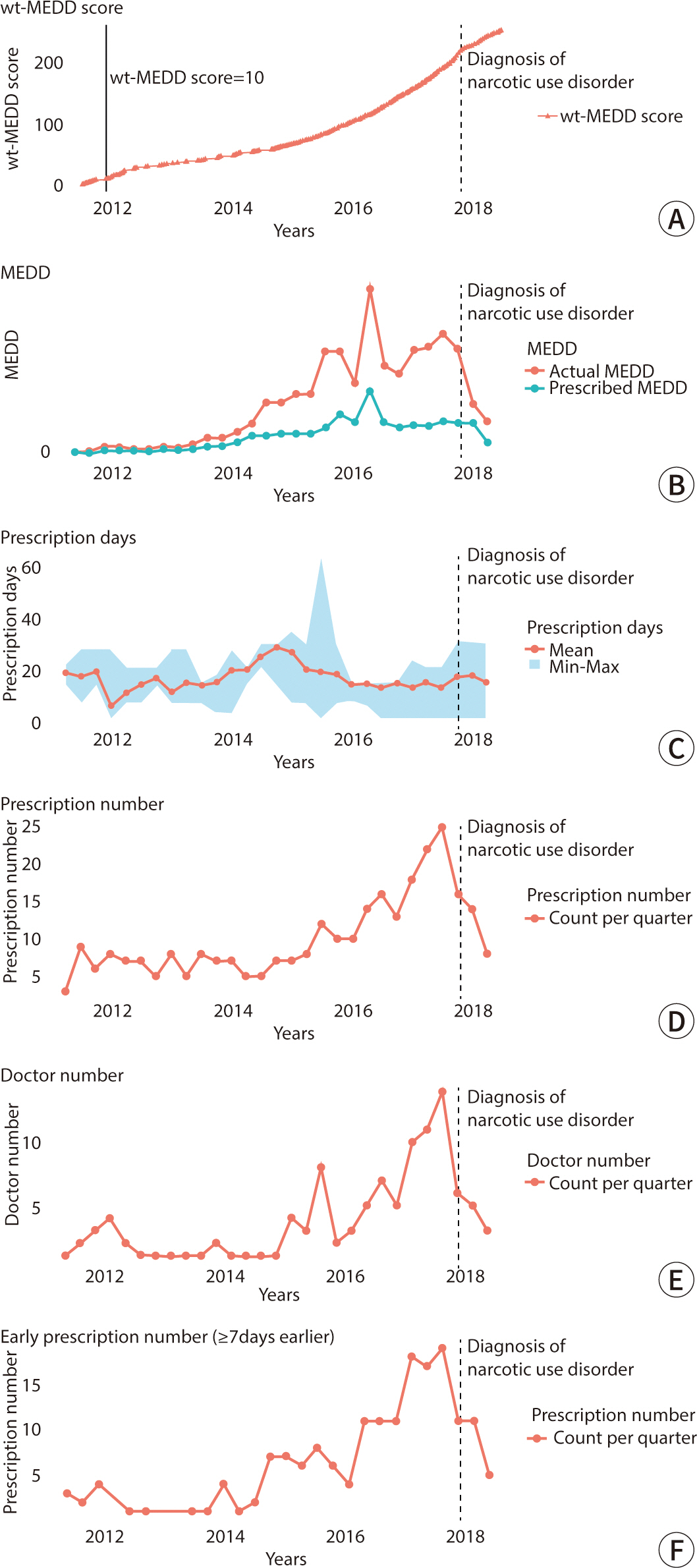
The difference between the actual MEDD and the intended MEDD (MEDD ratio)
continued to increase until the diagnosis of NUD was made (Fig. 4B). Concurrently, the number of prescription days
(mean, minimum, and maximum) showed an increase just prior to the rise in the
MEDD ratio (Fig. 4C). Similarly, the
patterns of increase in the number of prescriptions (Fig. 4D), the number of prescribing doctors per 3-month
period (Fig. 4E), and the instances of
early receipt of narcotics for more than 7 days (Fig. 4F) mirrored the trend observed in the MEDD ratio. These
findings suggest that employing multiple strategies can elevate the MEDD ratio,
potentially leading to a diagnosis of NUD. Despite the use of various strategies
to obtain more narcotics, it is possible to effectively screen for NUD at an
early prescription stage using only the wt-MEDD score, without the need for
multiple indicators.
Discussion
Key results
The wt-MEDD score demonstrated remarkable effectiveness in identifying early
patterns of narcotic prescriptions in patients who were later diagnosed with
NUD. This score reflects the number of prescription dates with a high MEDD
ratio. A wt-MEDD score greater than 10.5 marked patients as significant
outliers, aligning with the optimal cut-off value used by physicians to detect
NUD. With a sensitivity of 100% and a specificity of 99.6%, a wt-MEDD score of
10.5 proved highly effective in identifying patients diagnosed with NUD. These
results indicate that a wt-MEDD score of 10.5 could serve as a screening tool to
detect patients with NUD, particularly those engaging in behaviors like
"doctor shopping" to obtain excessive amounts of narcotics.
Interpretation
Our hospital undertook an analysis of abnormal patterns in narcotic prescriptions
to prevent NUD in patients by providing feedback to prescribing doctors.
Initially, we consulted the CDC guideline [7], which proved both reasonable and useful, as evidenced by its
alignment with the optimal cut-off values identified in our study for detecting
patients with NUD. However, adherence to the CDC guideline alone was
insufficient for categorizing a patient with NUD. To provide prescribing doctors
with clearer information reflective of NUD, we took into account scenarios that
could be problematic without exception. For instance, a patient receiving high
doses of narcotics inconsistent with the prescribing doctor's intentions
was identified as a problematic situation and thus was considered appropriate
for defining NUD.
Comparison with previous studies
In the United States, the PDMP system automatically calculates the MEDD for
prescribed narcotics. It provides the total MEDD for multiple prescriptions on
the date they are issued; however, it does not calculate the overlapping MEDD
that results from multiple prescriptions on a specific intake date [17]. Although the Ohio Automated Rx
Reporting System displays daily MME for prescribers, this information is not
stored, making it challenging to reconstruct later [17]. Previous studies have examined overlapping
prescriptions, focusing either on concurrent benzodiazepine and narcotic
prescriptions [18] or on overlapping
prescriptions without considering the overlapping MEDD [19]. To our knowledge, this study is the first to evaluate
the wt-MEDD score, which is based on the number of days with a high MEDD ratio,
as a tool for identifying abnormal prescription patterns.
The wt-MEDD score is effective in identifying abnormal prescriptions,
irrespective of the methods patients employ to obtain more narcotics.
Additionally, a graph depicting the MEDD ratio over time can be made available
for each patient in the outpatient clinic. The capability to quickly observe
temporal changes through the graph can significantly reduce the time required to
detect unusual prescription patterns.
An opioid-risk tool, previously reported and based on fixed patient
characteristics such as a history of alcoholism, has been shown to have a
primary prevention effect on NUD [20].
However, it does not contribute to secondary prevention. In contrast, monitoring
the wt-MEDD score facilitates screening prior to an increase in the number of
abnormal prescriptions.
Limitations
Calculating the wt-MEDD score based on overlapping MEDD could lead to an increase
in data volume, as each intake date—rather than just the prescription
date—adds an additional row to the table. In our study, the data size for
tables based on each intake date was five times larger than those based on each
prescription date. However, limiting the analysis to patients who have been
prescribed narcotics, rather than including all hospital patients, could
alleviate the burden of data analysis. Additionally, our study only included a
small number of patients diagnosed with NUD, possibly due to physicians'
reluctance to diagnose NUD. This issue is particularly acute for patients who
have received narcotics prescriptions from more than one department, where
cross-departmental liability issues may complicate the diagnosis of NUD.
Consequently, there could be a larger number of undiagnosed NUD cases,
especially among those categorized as wt-MEDD outliers. Moreover, our analysis
did not include narcotic prescriptions for cancer patients, inpatients, or those
receiving relatively low doses of narcotics such as codeine and tramadol. These
groups are expected to be analyzed using different criteria. This study was
retrospective, suggesting that a prospective trial might be necessary to
determine if monitoring the wt-MEDD score can reduce the incidence of NUD.
Additionally, since our study population was limited to a single hospital, it
did not account for narcotics prescribed to patients at other facilities. Given
that patients with NUD are likely to receive narcotics prescriptions from
multiple hospitals, an integrated system to monitor narcotic prescriptions
nationwide becomes essential. In the United States, for example, the PDMP
manages all narcotic prescriptions at the state level [21]. However, the variation in narcotic policies between
different hospitals and countries could complicate such analysis [22]. Nonetheless, if the system can
effectively detect NUD through hospital prescriptions, a method for confirming
the wt-MEDD score might prove universally beneficial.
Conclusion
We defined the wt-MEDD score as the number of prescription days with a high MEDD
ratio, based on the definition of narcotic abuse. The wt-MEDD score identified
patients diagnosed with NUD with greater sensitivity and specificity than other
metrics. Therefore, monitoring the wt-MEDD score could enable early
interventions for irregular narcotics prescription patterns by doctors and help
prevent the development of NUD in patients.
 XML Download
XML Download