

 PDF
PDF Citation
Citation Print
Print



Introduction
Background
Distal radius fractures are among the most common fractures encountered in the
emergency room [1]. In the younger
population, these fractures typically result from high-energy trauma, whereas in
older adults, weakened, porous bones make them susceptible to fractures from
minor trauma. For stable distal radius fractures in both groups, the
conservative treatment approach is closed reduction followed by immobilization
using a plaster cast [2]. However, there
is still no clear guideline on the best method and immobilization period to
apply plaster cast.
One of the most debated aspects of plaster cast application involves the length
of the cast (above or below the elbow) and the duration of immobilization. Even
when an acceptable reduction is unattainable, previous studies have demonstrated
that well-established radiological parameters do not necessarily correlate with
a favorable functional outcome in older patients. Conversely, functional outcome
reflects the patient's satisfaction with the treatment and should be the
primary consideration [3].
Objectives
The aim of this study is to investigate the clinical and radiological outcomes of
various non-operative treatments for distal radius fractures, focusing on the
length of the cast and the duration of immobilization. We hypothesize that using
a short arm cast with a shorter period of immobilization will yield clinical and
radiological outcomes comparable to those achieved with a long arm cast and a
longer immobilization period (>4 weeks).
Methods
Ethics statement
This was a literature-based study; thus, neither institutional review board
approval nor informed consent was required.
Study design
This systematic review was performed in accordance with the PRISMA guidelines
[4]. A review protocol was registered
on PROSPERO (registration number: CRD42020212627).
Eligibility criteria
All types of randomized controlled trials (RCTs) published as full articles were
included in this study. The selection of articles was based on the stated
inclusion and exclusion criteria, following the PICO (population, intervention,
comparison, outcome) method as outlined in Supplement 1.
Information sources
We performed a systematic search of English-language literature from the past
five years on PubMed/MEDLINE, Cochrane Central Register of Controlled Trials
(CENTRAL), and ClinicalTrials.gov.
Search strategy
The search terms included, but were not limited to, "distal radius
fracture," “Colles fracture,” “management,”
“treatment,” “casting,”
“immobilization,” and “nonoperative.”
Selection and data collection process
The quality of the included RCTs was assessed by two independent reviewers using
the 13-item 2015 Updated Method Guideline for Systematic Reviews from Cochrane
[5].
Data items
The data were extracted using a standardized data collection form by a research
team, with each selected article being independently screened by two reviewers.
Disagreements between reviewers about whether to include or exclude a study will
be resolved through consensus, and if necessary, by consulting a third
reviewer.
Study risk of bias assessment
A critical appraisal of all potential studies was conducted to assess their
eligibility, utilizing a scoring system adapted from the Joanna Briggs
Institute. The evaluation criteria included study population, exposures,
confounding factors, outcomes, follow-up duration, and statistical analysis.
Effect measures
Data were extracted from study reports and under appropriate conditions for each
test to compare and identify associations.
Synthesis methods
The variables collected included patient age, sex, fracture classification,
interventions used, follow-up, Disabilities of the Arm, Shoulder, and Hand
(DASH) score, Patient-Rated Wrist Evaluation (PRWE) score, the Mayo Wrist Score,
the visual analog scale score, the complication rate, and radiological
parameters (volar tilt, radial inclination, radial length, ulnar variance). The
results were then tabulated into specific tables for drawing conclusions.
Results
Study selection
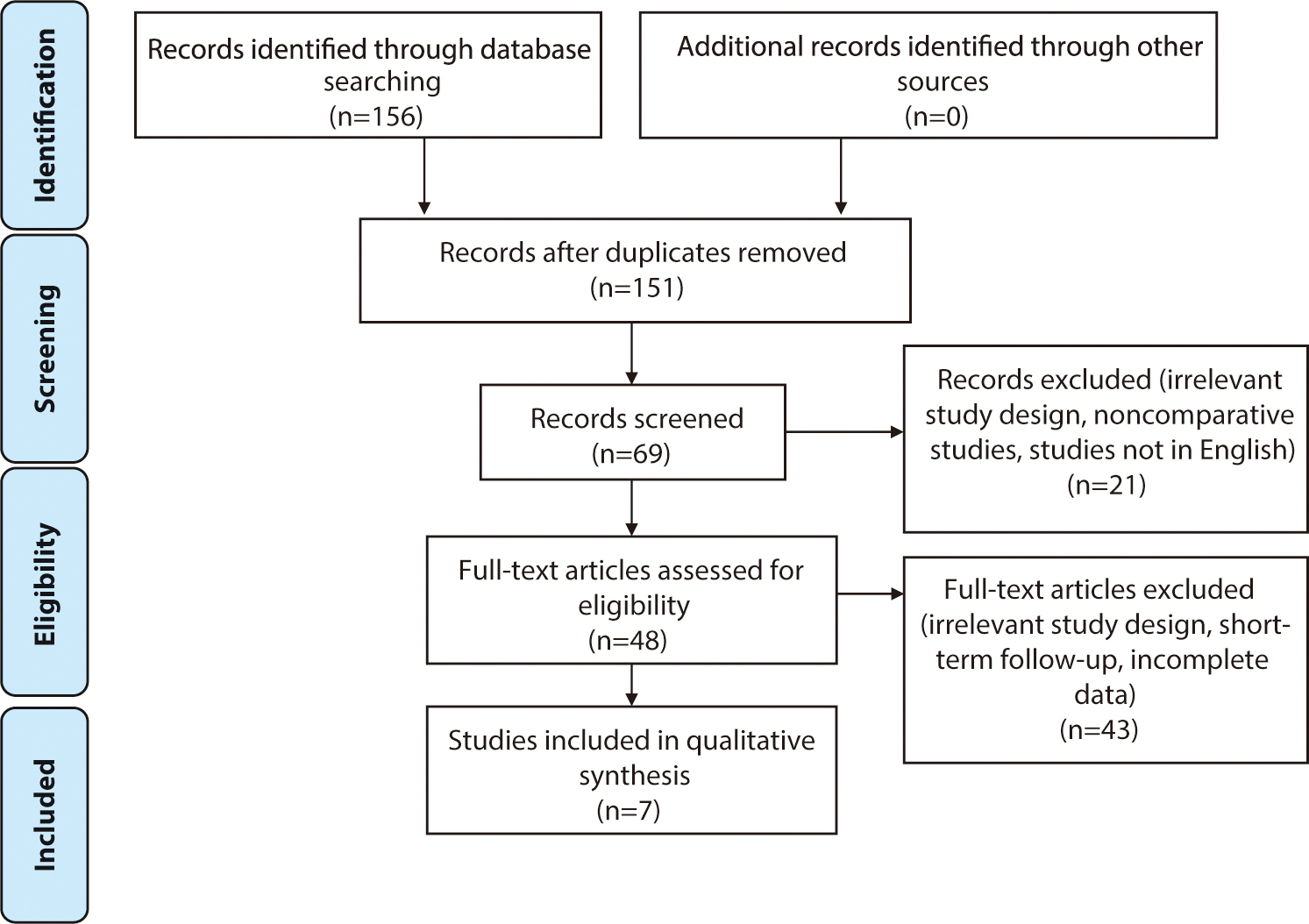
The identification of studies in the primary literature search and the flow
diagram of the selection process, according to PRISMA guidelines, are presented
in Fig. 1.
Study characteristics
The initial electronic search across all databases yielded 156 records. Following
a selection process, seven articles were included in the analysis.
Risk of bias in studies
All seven studies were confirmed to be of high quality, each receiving a
"yes" response for more than seven parameters, as shown in Supplement 2.
Results of syntheses
Baseline characteristics
A total of 542 distal radius fractures were analyzed. All studies reported a
higher proportion of female participants over the age of 50. Most of these
fractures were stable, extra-articular fractures with minimal displacement;
however, unstable fractures were also observed. The follow-up period ranged
from 3 to 18 months (Table 1).
Table 1.
Basic characteristics of studies
| No | Author | Intervention | Control | Sample size (n) | Gender (male/female) | Mean age (yr) | Fracture classification | Follow-up (mo) |
|---|---|---|---|---|---|---|---|---|
| Immobilization methods | ||||||||
| 1 | Park et al. [6] | PC SAC | PC LAC |
I: 36 C: 33 |
I: 2/34 C: 4/29 |
I: 66.1 C: 67.5 |
Stable fracture | 6 |
| 2 | Caruso [7] | PC SAC | PC LAC |
I: 37 C: 37 |
I: 3/33 C: 4/32 |
I: 72.3 C: 69.5 |
Extra-articular and dorsal displacement (type 2R3A2.2) | 3 |
| 3 | Okamura et al. [8] | PC SAC | PC LAC |
I: 64 C:64 |
I: 23/41 C: 17/47 |
I: 60.52±14.74 C: 62.97±13.03 |
2R3A2/2R3A3/2R3C1 /2R3C2/2R3C3 |
6 |
| Immobilization periods | ||||||||
| 1 | Christersson et al. [9] | PC 10 d | PC 10 d+3 wk |
I: 54 C: 55 |
I: 7/47 C: 4/51 |
I: 67 C: 64.7 |
2R3A3/2R3C2/2R3C3 | 12 |
| 2 | Bentohami et al. [10] | PC 3 wk | PC 5 wk |
I: 36 C: 36 |
I: 10/26 C: 13/23 |
I: >60 yr in 41.67% of
patients C: >60 yr in 50% of patients |
Stable fractures | 12 |
| 3 | Boersma et al. [11] | PC 1 wk | PC 4–5 wk |
I: 26 C: 14 |
I: 7/19 C: 4/10 |
I: 52.3±16.2 C: 56.5±9.6 |
2R3A/2R3B/2R3C | 12 |
| 4 | Olech et al. [12] | PC 4 wk | PC 6 wk |
I: 26 C: 24 |
33 women+17 men |
I: 71.34±4.99 C: 72.2±5.46 |
Stable fractures | 12–18 |
![]()
Outcomes of plaster casting
The seven RCTs discussed plaster casts in terms of the cast length (short
versus long arm cast; n=3) and the length of the immobilization period
(n=4). Three RCTs concluded that the clinical outcomes were comparable
between short arm casts and long arm casts (Table 2). Long arm casts and short arm casts demonstrated
comparable radiological outcomes, as measured by volar tilt, radial
inclination, radial height, and ulnar variance (Table 3).
Table 2.
Comparison of clinical outcomes
| No | Author | Conclusion | DASH | PRWE | Mayo Wrist Score | VAS | Complication |
|---|---|---|---|---|---|---|---|
| Immobilization methods | |||||||
| 1 | Park et al. [6] | SACs were as effective as LACs for stable distal radius fractures in older patients. Furthermore, they were more comfortable and introduced fewer restrictions on daily activities. |
SAC: 30±15 LAC: 26.8±14.3 |
NA | NA |
SAC: 2.5±1.2 LAC: 2.1±0.84 |
NA |
| 2 | Caruso et al. [7] | Patients treated with SACs had comparable radiological and functional scores to those treated with LACs, with fewer complications secondary to immobilization of the elbow joint. |
SAC: 0.8
(0–2.1) LAC: 1.7 (0–2.5) |
NA | NA | NA | NA |
| 3 | Okamura et al. [8] | SACs demonstrated no difference in DASH outcomes, comparable reduction maintenance, and fewer adverse effects than LACs. |
6 mo: SAC: 9.88 LAC: 9.44 |
NA | NA |
6 mo (wrist): SAC: 4.89 LAC: 7.03 6 mo (shoulder): SAC: 2.69 LAC: 3.52 |
SAC: 9 LAC: 19 Most common: shoulder pain, malunion |
| Immobilization periods | |||||||
| 1 | Christersson et al. [9] | PC removal 10 d after reduction in moderately displaced DRFs is not recommended. | NA | NA | NA | Insignificant pain difference at 12 mo (P=0.92) | NA |
| 2 | Bentohami et al. [10] | Equal patient-reported outcomes between 3 wk and 5 wk of plaster cast immobilization. |
I: 0 C: 12.5 |
I: 5.0 C: 8.8 |
NA |
I: 3.1 C: 2.6 |
No complication in fracture healing, no non-union or CRPS |
| 3 | Boersma et al. [11] | 1 wk of PC treatment for nonreduced DRFs resulted in comparable functional outcomes, pain scores, complication rates, and secondary displacement. |
I: 4.6±9.5 C: 3.5±4.1 |
I: 2.9±6.6 C: 2.1±3.3 |
NA |
4 wk: I: 2.2±1.7 C:1.9±2.0 |
I: 1 C: 4 Most common: ulnar sided wrist pain, DRUJ pain, CRPS |
| 4 | Olech et al. [12] | Similar VAS and Mayo Wrist Scores between the two groups. The greatest volar tilt angle occurred after 6 wk of PC. No significant differences in other radiological parameters between the two groups. | NA | NA |
I: 58.46 ±21.24 C: 61.87 ±22.97 |
VAS pain: I: 2.53±3.06 C: 3.58±2.56 VAS activity: I: 7.61 ±1.83 C: 7.58 ±2.3 |
NA |
DASH, Disabilities of the Arm, Shoulder, and Hand; PRWE, Patient-Rated Wrist Evaluation; VAS, visual analog scale; SAC, short arm cast; LAC, long arm cast; NA, not available; PC, plaster cast; I, intervention; C, control; DRF, distal radius fracture; DRUJ, distal radioulnar joint; CRPS, complex regional pain syndrome.
![]()
Table 3.
Comparison of radiological outcomes
| No | Author | Volar tilt (°) | Radial inclination (°) | Radial length (mm) | Ulnar variance (mm) |
|---|---|---|---|---|---|
| Immobilization methods | |||||
| 1 | Park et al. [6] |
3 mo: - SAC: –0.2±6.0 - LAC: 3.9±6.2 6 mo: - SAC: –3.6±5.6 - LAC: 2.3±6.2 |
3 mo: - SAC: 13.4±6.5 - LAC: 15.4±6.1 6 mo: - SAC: 10.1±7.1 - LAC: 12.4±6.9 |
3 mo: - SAC: 5.0±3.7 - LAC: 6.2±2.6 6 mo: - SAC: 3.1±3.9 - LAC: 4.5±2.9 |
NA |
| 2 | Caruso et al. [7] |
3 mo: SAC: 0 ([–4.5]–8) LAC: 0 ([–4]–7.5) |
3 mo: SAC: 22 (19–24.5) LAC: 21 (17.5–23) |
3 mo: SAC: 9 (7–10) LAC: 8 (6–10) |
3 mo: SAC: 0 (0–1) LAC: 0 ([0.5]–2.25) |
| 3 | Okamura et al. [8] |
SAC: –1.04 LAC: –1.27 |
SAC: 18 LAC: 16.31 |
SAC: 7.89 LAC: 7.49 |
SAC: 1.41 LAC: 1.93 |
| Immobilization periods | |||||
| 1 | Christersson et al. [9] |
12 mo: the 10-d group exhibited 1.1° more redisplacement (P=0.48) than the 1-mo group |
12 mo: the 10-d group exhibited 3.2° more redisplacement (P=0.002) than the 1-mo group |
12 mo: The 10-d group demonstrated 0.7 mm more axial compression (P=0.02) than the 1-mo group |
NA |
| 2 | Bentohami et al. [10] | 1 Patient in each group showed secondary displacement | |||
| 3 | Boersma et al. [11] | NA | NA | NA | NA |
| 4 | Olech et al. [12] |
I: 9.13±7.12 C: 3.29±5.11 |
I: 1.9±1.62 C: 2.45±2.47 |
I: 0.55±2.84 C: 0.25±1.03 |
NA |
![]()
Ten days of immobilization has not been proven effective radiologically, as
it has been associated with redisplacement in terms of radial inclination
and radial height compared to 1 month of immobilization. However, these
findings remain controversial, as one study demonstrated similar outcomes
between 1 week and 4–5 weeks of plaster cast immobilization.
Generally, a minimum of 3 weeks of immobilization in a plaster cast is
sufficient to provide satisfactory clinical and radiological outcomes for up
to 18 months of follow-up.
Discussion
Interpretation
This study aimed to objectively compare conservative treatment methods for distal
radius fractures. The findings indicated that both long and short arm casts were
equally effective in preventing displacement and achieving satisfactory
functional outcomes. However, an immobilization period of less than three weeks
was associated with poorer radiological outcomes, which could potentially lead
to inferior final functional results.
Comparison with previous studies
Immobilization with casting is the common initial treatment for a distal radius
fracture. Although the final radiographic alignment may not be optimal,
long-term motion and patient-reported outcomes from casting are similar to those
of surgical treatments [1,13,14]. To optimize the effectiveness of casting, the brachioradialis
was identified as a major deforming force, necessitating the use of a long-arm
brace in supination to neutralize its action [15]. However, based on three RCTs analyzed in this systematic
review, there is no significant difference in DASH scores between long-arm and
short-arm casts. We also discuss the results of studies on various periods of
immobilization.
Patient-reported outcome measures for the upper extremity
Patient-reported outcome measures are crucial in short-term follow-up because
recent evidence suggests they do not correlate with radiological measures
[3,16,17]. However, it is
important to use a consistently reliable measurement tool to ensure valid
comparisons between different treatments. Previous studies have shown that
the DASH and PRWE scales are reliable, valid, and responsive tools for
assessing upper limb injuries, making them superior to other outcome
measures [18,19].
When to place a long arm cast and how long to immobilize the patient in a plaster cast?
The main disadvantage of a long arm cast is that it restricts forearm
rotation and elbow flexion-extension. It is also heavy and cumbersome, which
can increase the incidence of shoulder pain [6] and limit daily activities [20]. Conversely, a short arm cast may offer the advantage of
causing less temporary disability and inconvenience, as it allows for elbow
motion. However, a long arm cast is known to better maintain reduction
because it prevents the long wrist flexors and extensors from deforming the
fracture [20]. Some surgeons
recommend using a long arm cast for unstable fractures, generally defined by
the Lafontaine criteria, which include at least three of the following:
dorsal angulation of more than 20 degrees, dorsal comminution,
intra-articular radiocarpal fracture, associated ulnar fracture, and age
over 60 years [21]. In these cases,
it is believed that the long arm cast prevents elbow motion and forearm
rotation, minimizing the risk of fracture displacement. However, this
approach remains a matter of debate, as some surgeons still prefer short arm
casts regardless of fracture stability [6].
The current systematic review revealed no significant differences in
functional scores between short arm casts and long arm casts for stable or
extra-articular distal radius fractures. Tolerance for functional loss
appears to be influenced by age and activity level, with younger individuals
demonstrating better DASH scores after short-term follow-up. Additionally,
many authors have noted that older populations are more accepting of
functional deficits or imperfect outcomes due to their lower functional
demands [22].
The immobilization period is a significant factor in the non-operative
treatment of distal radius fractures. Removing the plaster cast early is
aimed at facilitating quicker functional recovery and enhancing clinical
outcomes. However, our literature review indicates that removing the plaster
cast before 1 month leads to poorer functional [9] and radiological outcomes [23]. It was also recommended to immobilize the arm in a
functional position [23].
Strengths and limitations of the study
In previous systematic reviews, van Delft et al. [24] and de Bruijn et al. [25]
explored the duration of cast immobilization for distal radius fractures.
However, these reviews did not set a time restriction for the inclusion of
studies, which could introduce bias. Additionally, their focus was limited to
the duration of casting, without considering other relevant parameters. Saka et
al. [26] compared the effectiveness of
below-elbow and above-elbow casts for treating this condition, yet the evidence
provided was of low certainty. Similarly, Raj et al. [27] investigated various immobilization techniques, but the
significant variation in mean follow-up periods raised concerns about potential
bias in their findings.
This study aims to objectively compare clinical and radiological parameters
concerning conservative treatment methods for distal radius fractures, focusing
on the technique of application and the duration of immobilization. All included
studies are recently published RCTs with a minimum follow-up period of three
months, which should provide a high-quality overall analysis. However, our study
has several limitations. The number of RCTs investigating non-operative
treatment methods for distal radius fractures remains limited. Among the
available studies, the strength of evidence is insufficient, with notable
heterogeneity, particularly in terms of fracture types. Future studies should
consider pooling outcomes from RCTs that involve similar fracture types. Despite
these limitations, this study provides evidence supporting conservative
treatment for distal radius fractures.
 XML Download
XML Download