

 PDF
PDF Citation
Citation Print
Print



Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer, accounting
for 75%–80% of primary liver malignancies [1]. HCC mostly develops in the background of chronic liver disease, the
most common etiologies being HBV or HCV infection, and chronic alcohol abuse. During
the recent year, metabolic syndrome has become another major risk factor for HCC,
even in Asian countries [2,3].
The clinical outcome of patients with HCC is generally poor, mainly due to
difficulties in early detection and limited treatment options for advanced disease
[4,5]. Currently, systemic therapy, such as receptor tyrosine kinase inhibitors
and immunotherapy, is the treatment of choice for the patients with unresectable HCC
[5]. However, the efficacy of systemic
therapy in HCC is still unsatisfactory with survival benefit of 1–3 months,
objective response rate less than 30%, and a high incidence of adverse events [6,7]. In
this context, understanding the heterogeneity of HCC will play a key role in
developing effective diagnostic and therapeutic strategies, by offering potential
predictive biomarkers and personalized approaches for HCC management.
Ethics statement
It is a literature database-based review; therefore, neither approval by the
institutional review board nor obtainment of informed consent was required.
Morpho-molecular heterogeneity of hepatocellular carcinoma
HCC is typically composed of tumor cells showing hepatocytic differentiation with
variable degrees of atypia [8]. While HCC
recapitulates the cytoarchitectural morphology of the liver to varying extents,
there are alterations in the hepatic microarchitecture such as loss of portal
tracts, reduction or loss of the reticulin framework, and thickening of the hepatic
plates. Neoangiogenesis occurs in HCCs, in the form of sinusoidal capillarization
and unpaired arteries [8]. These changes also
result in the characteristic imaging features, such as the early enhancement on
contrast enhanced CT/MRI.
However, there is considerable heterogeneity of HCC, in the microscopic growth
patterns, cytological features, and histological grade. About 50% of HCCs
demonstrate mixed patterns of growth: trabecular, pseudoglandular, solid, and
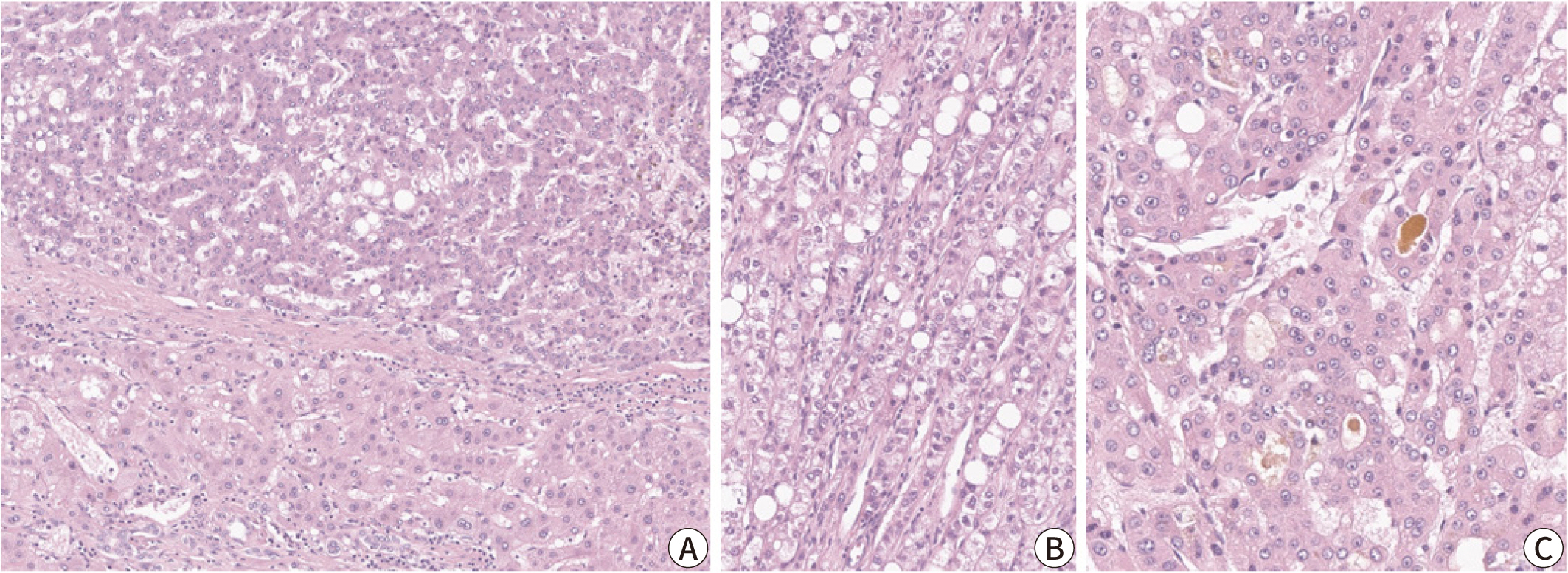
macrotrabecular (Fig. 1) [9]. In addition, while most HCCs demonstrate cytological
features that recapitulate those of normal hepatocytes (i.e. polygonal cells with
abundant eosinophilic cytoplasm), some HCCs show extensive areas with clear cell
change, fatty change, and cholestasis. Cytoplasmic inclusions (e.g., hyaline bodies,
Mallory-Denk bodies, and pale bodies) may also be seen in some tumor cells [8]. Histological grading is currently performed
according to either the four-tiered modified Edmondson and Steiner system or the
three-tiered World Health Organization (WHO) grading system [9–11].
Fig. 1.
Microscopic features of a typical hepatocellular carcinoma (HCC). (A) Non-neoplastic hepatocytes (lower half) and HCC tumor cells (upper half) are separated by a fibrous capsule. (B) Trabecular pattern HCC with steatosis. (C) Pseudoglandular pattern HCC with cholestasis (Hematoxylin-Eosin stain, original magnification ×100 [A,B], ×200 [C]).
Recent advances in genomic techniques have unraveled the heterogeneity in the
mutational landscape of HCC [12,13]. The most frequently mutated genes include
TERT promoter, TP53, CTNNB1, ARID1A, ARID2, JAK1, ALB,
AXIN1, NFE2L2, and RPS6KA3 [12]. In addition, gene expression profiling studies have
suggested several molecular subclasses of HCC that correlate with the
clinicopathological features, providing the foundation for an integrated
morphological-molecular classification of HCC [14]. In the past two decades, there have been many efforts to establish
a subclassification system that better categorizes HCCs with distinct clinical,
histological, and molecular features (Table
1) [13,15–19]. HCC can be
subclassified into two major groups, the proliferative class and the
non-proliferative class. The proliferative class is characterized by high
chromosomal instability and TP53 mutations, and is associated with
poor histological differentiation, frequent vascular invasion, increased
alpha-fetoprotein (AFP) level, and overall poor clinical outcome [16,18].
On the other hand, the non-proliferative class displays chromosomal stability and a
well-differentiated phenotype with less frequent vascular invasion [16,18].
CTNNB1-mutated HCCs belong to the latter group: these
demonstrate frequent cholestasis and less immune cell infiltration on histology
[14,20].
Table 1.
Integrated morphological-molecular classification of hepatocellular carcinoma
| Classification system | Proliferative class | Non-proliferative class |
|---|---|---|
| Lee et al. [15] | Cluster A | Cluster B |
| Boyault et al. [16] | G1, G2, G3 | G4, G5, G6 |
| Chiang et al. [17] | Proliferation | Interferon, Poly7, CTNNB1 |
| Hoshida et al. [18] | S1, S2 | S3 |
| TCGA Research Network [13] | Immune high and intermediate | Immune excluded |
| Sia et al. [19] | iClust1, iClust3 | iClust2 |
| Clinical features | Poor clinical outcome, high AFP, HBV, frequent vascular invasion | Improved clinical outcome, low AFP, HCV, low vascular invasion |
| Histological features | Poorly differentiated | Well differentiated |
| Molecular alterations | Chromosomal instability, TP53 mutations, FGF19 amplification | Chromosomal stability, CTNNB1 mutations, TERT promoter mutations |
Currently, approximately 35% of HCC can be further subclassified into histological
subtypes with distinct morphological, clinicopathological and molecular
characteristics [9]. The following section
will summarize the clinicopathological and molecular features of these different
subtypes.
Steatohepatitic hepatocellular carcinoma
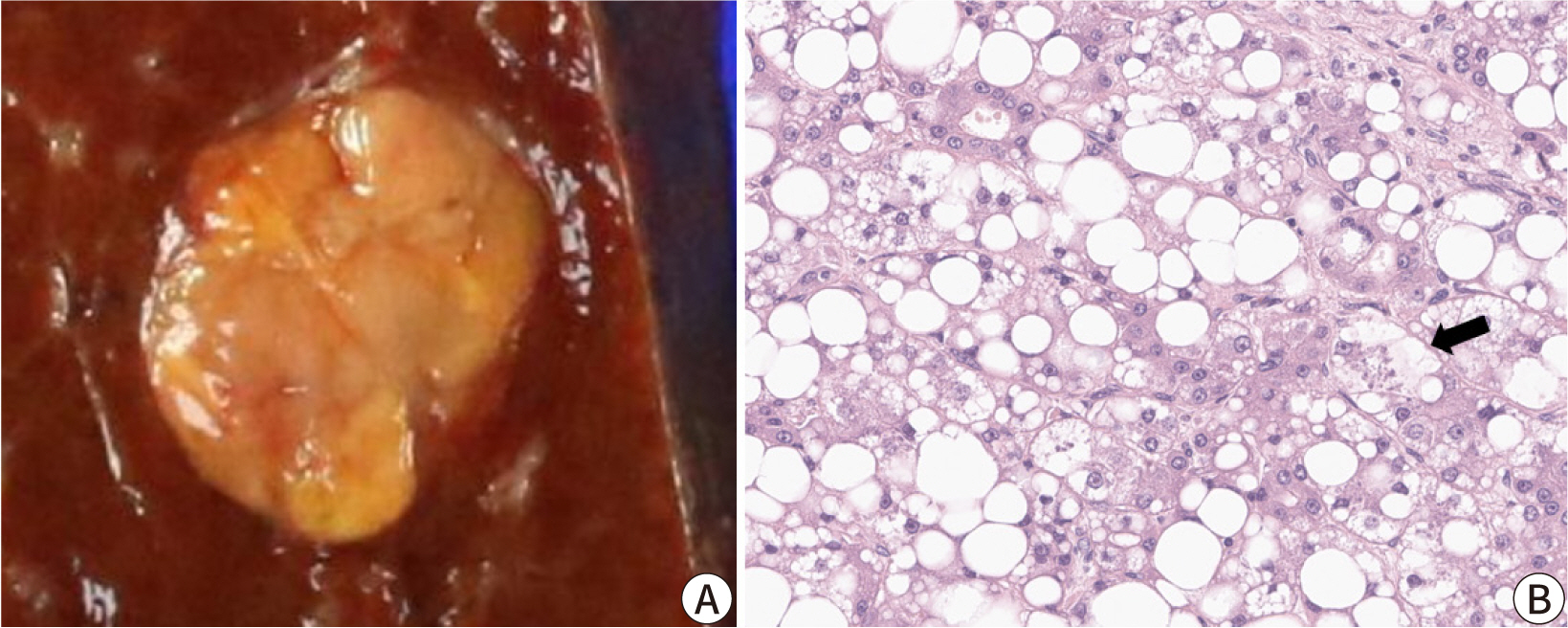
The steatohepatitic subtype of HCC demonstrates the key histological features of
non-neoplastic steatohepatitis, including steatosis, pericellular fibrosis, cell
ballooning, inflammation, and Mallory-Denk bodies, and these features occupy a major
portion (>50%) of the tumor (Fig. 2)
[21]. This subtype has been more
frequently identified in patients with underlying metabolic dysfunction-associated
steatotic liver disease and alcohol abuse, and its relative frequency has been
reported to be between 5% and 20% [3,21]. Steatohepatitic HCC has been associated
with less frequent vascular invasion and satellite nodules; however, its prognosis
appears to be similar to that of conventional HCC [14]. Key molecular alterations associated with steatohepatitic HCC
include IL-6/JAK/STAT activation, while CTNNB1, TERT promoter and
TP53 mutations have been found to be less frequent in these
tumors [14].
Fig. 2.
Steatohepatitic hepatocellular carcinoma (HCC). (A) The tumor demonstrates a yellow hue on macroscopy reflecting the lipid component. (B) High power magnification showing the diffuse steatosis of tumor cells, tumor cell ballooning (arrow), some inflammatory cells, and pericellular fibrosis (Hematoxylin-Eosin stain, original magnification ×400).
Clear cell hepatocellular carcinoma
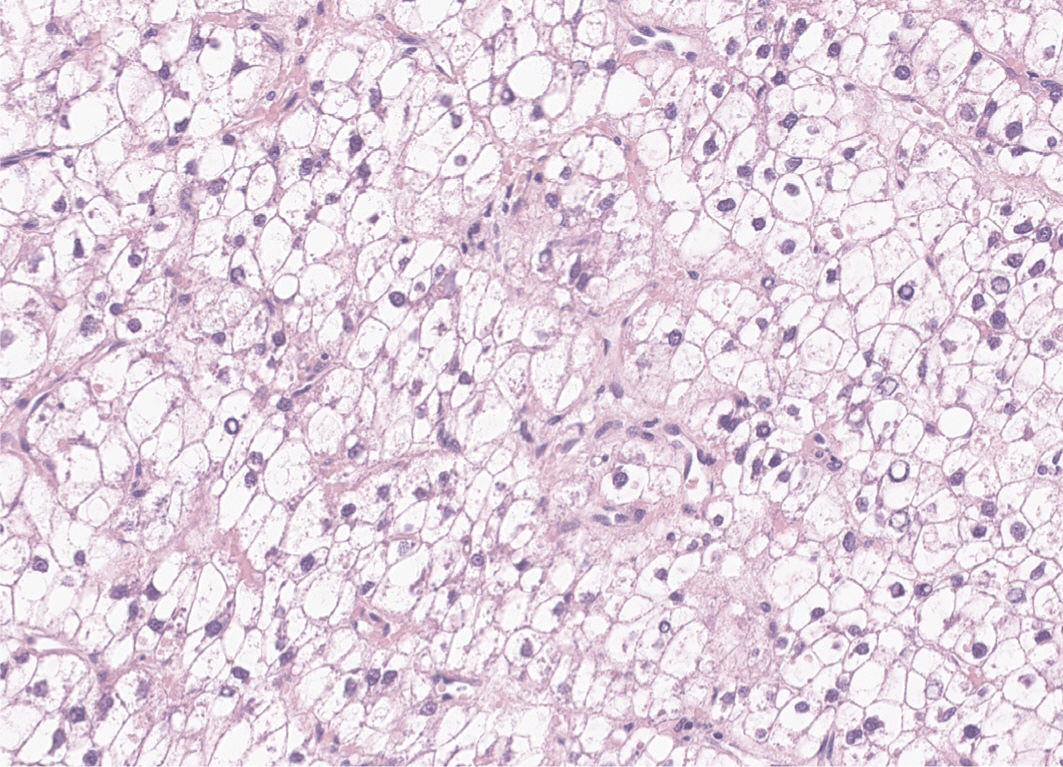
By definition, in clear cell HCCs, more than 80% of tumor cells demonstrate abundant
clear cytoplasm (Fig. 3). The clear cytoplasm
is a result of glycogen accumulation; however, some tumor cells may appear clear due
to lipid droplets, and some degree of steatosis is acceptable for this diagnosis
[22]. The relative frequency of clear
cell HCC has been estimated to be around 3%–7%. Clear cell HCCs are generally
well-differentiated tumors with a favorable prognosis [23]. One study has reported that clear cell HCCs demonstrate
higher frequency of IDH1 mutation, although this mutation is not
sufficient to define the subtype [24].
Macrotrabecular-massive hepatocellular carcinoma
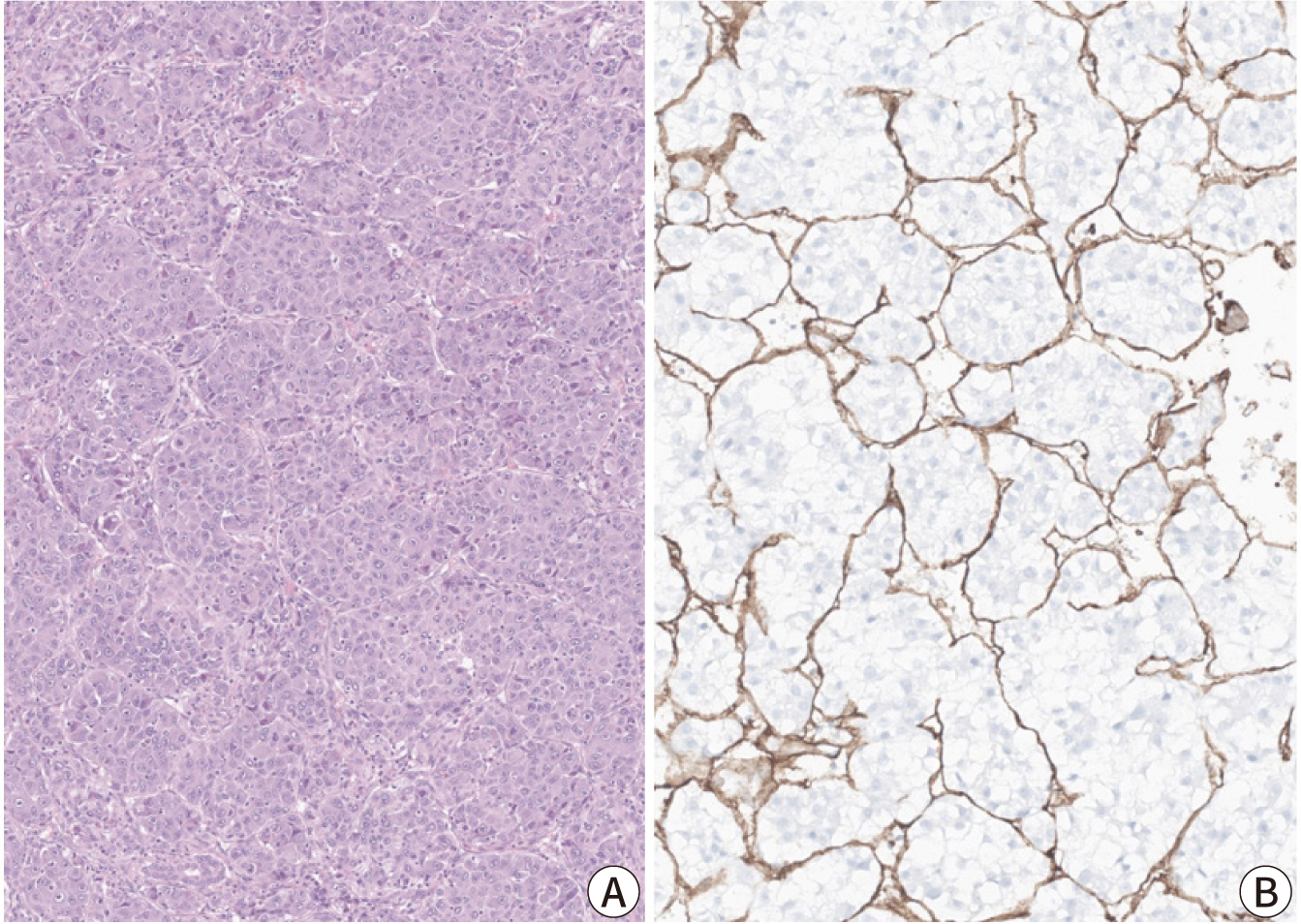
The macrotrabecular-massive subtype of HCC is an HCC in which more than 50% of the
tumor cells assume a macrotrabecular growth pattern, defined as large trabeculae
that are more than 6–10 cells thick (Fig.
4) [25]. This subtype accounts for
approximately 5% of all HCCs and has been strongly associated with elevated serum
AFP levels, high-grade cytological atypia, extensive lymphovascular invasion, more
frequent distant metastasis, and a poor prognosis [25,26]. In addition, the
vessels-encapsulating-tumor-clusters (VETC) pattern of neoangiogenesis, which has
been associated with metastatic dissemination of HCC, is often enriched in this
subtype (Fig. 4) [27,28].
TP53 mutations and FGF19 amplifications have
been more frequently identified in the macrotrabecular-massive subtype of HCC [14].
Fig. 4.
Macrotrabecular-massive hepatocellular carcinoma (HCC; A) and vessels-encapsulating-tumor clusters (VETC) pattern (B). (A) Macrotrabecular-massive HCC demonstrating thick tumor cell trabeculae, of more than 10-cell thickness (Hematoxylin-Eosin stain, original magnification ×100). (B) CD34 immunostain highlighting the VETC pattern, where the CD34-positive endothelial cells completely surround tumor cell clusters.
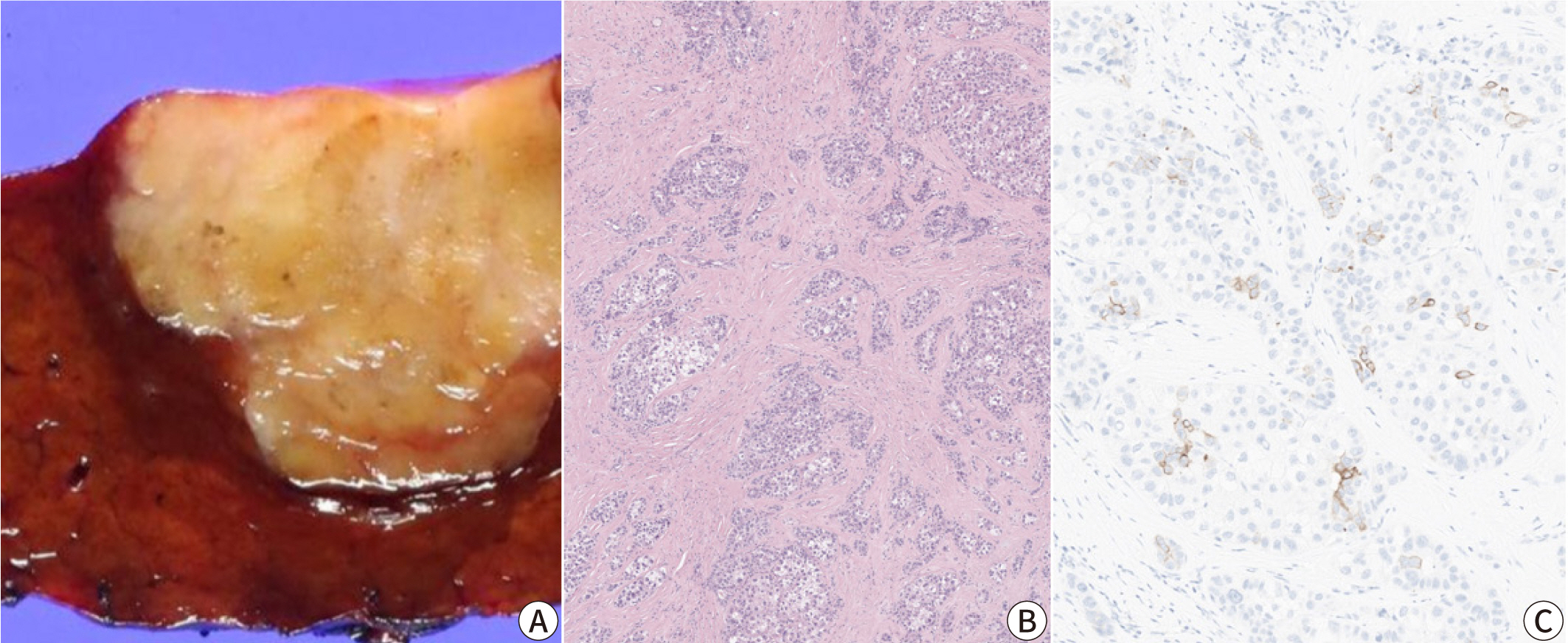
Scirrhous hepatocellular carcinoma
This subtype is characterized by dense intratumoral fibrous stroma (Fig. 5). The scirrhous subtype has a relative
frequency of 4% and often mimics intrahepatic cholangiocarcinoma on imaging [29]. Expression of immunohistochemical markers
associated with stemness (e.g., cytokeratin ([CK]) 7, CK19, and epithelial cell
adhesion molecule) is often seen in scirrhous HCCs, and increased expression of
cholangiocarcinoma-like and stem-cell-like genes have been identified by gene
expression profiling, consistent with the intermediate characteristic of this
subtype [30,31]. Furthermore, scirrhous HCC is associated with frequent
TSC1/TSC2 mutations and transforming growth factor-β
signaling activation [14,30].
Fig. 5.
Scirrhous hepatocellular carcinoma (HCC). (A) The tumor appears as a firm, yellowish-white and lobulated mass on gross examination, mimicking an intrahepatic cholangiocarcinoma. (B) Dense intratumoral fibrosis is evident at low power magnification (Hematoxylin-Eosin stain, original magnification ×40). (C) Immunohistochemical expression of cytokeratin 19 is seen in a few tumor cells.
Lymphocyte-rich hepatocellular carcinoma
The lymphocyte-rich subtype demonstrates massive intratumoral infiltration of
lymphocytes, which outnumber the tumor cells in most microscopic fields. This
subtype is rare, accounting for less than 1% of all HCCs, but has received much
attention as it has been associated with a favorable clinical outcome [32]. The lymphocyte-rich subtype is associated
with increased programmed death-ligand 1 expression and focal amplification of
chromosome 11q13.3, which is related to the immune checkpoint signature (CD274,
PDCD1, BTLA, CTLA4, HAVCR2, IDO1, and LAG3) [32–35]. Interestingly,
although this subtype is also known as “lymphoepithelioma-like HCC”,
it is not associated with Epstein-Barr virus infection, unlike the
lymphoepithelioma-like tumors arising in other organs, such as the nasopharynx and
stomach [32].
Fibrolamellar hepatocellular carcinoma
Fibrolamellar carcinoma, or fibrolamellar HCC, consists of strands of large
eosinophilic tumor cells with abundant cytoplasm and prominent nucleoli, and
separated by dense intratumoral bands of fibrosis [36]. Fibrolamellar carcinoma accounts for approximately 1% of all HCC,
occurs in younger patients (median age of 25 years), and the background liver is
non-cirrhotic [37]. The prognosis of
fibrolamellar carcinoma appears to be better than that of conventional HCC arising
in cirrhotic livers, but similar to that of HCC in non-cirrhotic livers [37]. DNAJB1-PRKACA gene fusion
has been identified in >95% of cases, and fluorescence in
situ hybridization for PRKACA gene rearrangement is a
useful ancillary test in confirming the diagnosis [38]. Expression of CK7 and CD68 in the tumor cells is another
characteristic of fibrolamellar carcinoma [38].
CTNNB1-mutated hepatocellular carcinoma
CTNNB1 mutations have been reported in approximately 20%–40%
of HCCs [39]. CTNNB1 encodes
β-catenin, which plays a key role in the WNT signaling pathway that regulates
liver function and zonation [40]. In
addition, bile salt transporter expression is dysregulated in these tumors,
histologically manifested by frequent intratumoral cholestasis. Some
CTNNB1-mutated HCCs may be diagnosed by gadoxetic acid-enhanced
MRI, due to the upregulation of the organic anion transporting polypeptide 1B3
(OATP1B3) [41]. Histologically,
CTNNB1-mutated HCCs are typically well-differentiated tumors
with microtrabecular and/or pseudoglandular growth patterns, intratumoral
cholestasis, and less immune cell infiltration compared to
non-CTNNB1-mutated HCCs [14,20]. However,
CTNNB1-mutated HCCs are not morphologically homogeneous, with
approximately 40% not demonstrating the “classic CTNNB1
morphology” [42]. Immunohistochemical
studies for β-catenin (nuclear expression) and glutamine synthetase (diffuse,
strong and homogeneous expression) may serve as useful surrogate markers for
CTNNB1 mutation.
Hepatocellular carcinoma with stemness-related marker expression
HCC with stemness-related marker expression, or progenitor HCC, is defined as HCC
expressing stemness-related markers, e.g., CK19, in >5% of the tumor cells
[15]. This subset of HCCs differ from
combined hepatocellular-cholangiocarcinoma, as they are morphologically compatible
with HCC, and there is no evidence of glandular differentiation or mucin production
in these tumors. They are associated with increased serum AFP levels, frequent
vascular invasion, poor histological differentiation, high recurrence rate,
resistance to systemic chemotherapy and locoregional treatment, and overall poor
prognosis [43]. HCCs with stemness-related
marker expression more frequently demonstrate TP53 mutations and
chromosomal instability, and increased PD-L1 expression [33,34].
Hepatocellular carcinomas with vessels-encapsulating-tumor-clusters pattern
The VETC phenotype is defined by the presence of VETC pattern in more than 55% of the
tumor area, characterized by CD34-positive vessels that encapsulate and isolate
individual tumor clusters, forming a cobweb-like pattern (Fig. 4) [27,28,44].
The VETC pattern is often found in the macrotrabecular-massive subtype of HCC (7.8%)
and is associated with aggressive behavior and metastatic dissemination [27,28].
It has been reported that VETC pattern is related to a novel mechanism of
metastasis, independent of epithelial-to-mesenchymal transition [44]. Furthermore, patients with VETC-positive
HCC have shown greater survival benefits from sorafenib therapy compared to those
with VETC-negative HCC, suggesting that the VETC pattern may serve as a potential
predictive marker for sorafenib response [28]. Correlation between the VETC pattern on histology and a rim arterial
phase hyperenhancement in arterial phase imaging suggests a role for imaging in the
prognostication of HCC [45].
Other rare histological subtypes of HCC have been described. The chromophobe subtype
of HCC has tumor cells with clear to pale cytoplasm and mainly bland nuclei with
focal areas of striking nuclear atypia [46].
Chromophobe subtype is strongly associated with alternative lengthening of
telomeres, a telomerase-independent mechanism of telomere maintenance, which can be
detected by fluorescence in situ hybridization [46]. Its prognosis is currently known to be
similar to that of conventional HCC [47].
Neutrophil-rich HCC is characterized by marked intratumoral neutrophilic
infiltration, granulocyte colony-stimulating factor production by tumor cells, and a
poor prognosis [47]. The tumor cells are
often poorly differentiated, and focal sarcomatoid differentiation can be observed
[48].
Conclusion
Recent molecular studies have significantly enhanced our understanding of the
morphological and molecular heterogeneity of HCC, providing the foundation for more
effective and personalized treatment strategies. Pathologists are becoming
increasingly aware of the histomorphological heterogeneity of HCC, and the
specification of the various subtypes of HCC has helped pathologists understand the
histology of HCC in more detail and the various differential diagnoses and
diagnostic pitfalls for each variant. The correlation between the histomorphology
and the molecular and biological features suggests the role of histology in the
prediction of therapeutic response and prognosis. This may be further facilitated by
the recent advances in digital pathology and artificial intelligence-based biomarker
research.
 XML Download
XML Download