

 PDF
PDF Citation
Citation Print
Print



Introduction
Background
Radiation oncology has seen significant advancements in recent decades, driven by
the introduction of several innovative technologies. These include
intensity-modulated radiation therapy, stereotactic radiosurgery, stereotactic
body radiation therapy, image-guided radiation therapy (IGRT), and respiratory
beam control. These technologies have increased the precision of treatments
[1], reduced side effects [2,3],
and improved patient outcomes [4–6]. Furthermore, the
advent of various imaging modalities such as CT, MRI, and PET scans, coupled
with significant developments in computational resources, has greatly expanded
the capabilities of radiation oncology. These imaging modalities provide
complementary information: CT scans deliver detailed anatomical information, MRI
offers exceptional soft tissue contrast, and PET scans provide metabolic
insights into tumors. By integrating these modalities, radiation oncologists can
achieve more accurate tumor localization, more precise treatment planning, and
better treatment adaptation, thereby further improving patient care and
outcomes.
Intensity-modulated radiation therapy enables the modulation of radiation beams
to conform more precisely to the shape of the tumor, thereby protecting
surrounding healthy tissues and reducing complications [7–9]. However,
this technique requires meticulous treatment planning and the implementation of
rigorous quality assurance protocols, which can be challenging [10,11]. Stereotactic radiosurgery and stereotactic body radiation
therapy administer high doses of radiation with sub-millimeter accuracy to treat
small, well-defined tumors in the brain and body, respectively. The primary
challenge in these therapies is managing patient movement and ensuring accurate
targeting. These issues can be addressed using advanced imaging technologies and
motion management techniques [12,13]. IGRT employs advanced imaging
technologies to enhance the precision of radiation delivery by compensating for
patient movement and anatomical changes during treatment [14]. The advantage of IGRT is its ability to adapt
treatment in real-time. However, challenges include integrating imaging and
treatment systems and maintaining consistent image quality [15]. Respiratory gating aligns radiation
delivery with the patient's breathing cycle, minimizing exposure to
moving organs such as the lungs and liver. The main challenges associated with
respiratory gating include the need for advanced equipment and software, as well
as requiring patient cooperation [16].
Integrating artificial intelligence (AI) into radiation oncology is becoming
increasingly important due to various social and healthcare trends [17]. The global population is aging, which
leads to a higher incidence of cancer in older age groups. As life expectancy
increases, so does the demand for effective and efficient cancer treatments,
placing significant burdens on healthcare systems worldwide [18]. To manage the increasing patient load
effectively, it is essential to adopt advanced technologies [19].
Moreover, healthcare systems are under pressure to improve patient outcomes while
controlling costs [20]. AI has the
potential to meet these challenges by improving the accuracy of radiation
therapy, shortening treatment durations, and reducing side effects. This can
result in better resource utilization and heightened patient satisfaction [21]. Additionally, AI supports personalized
medicine by offering treatments customized to the unique characteristics of each
patient. By analyzing extensive datasets from diverse sources, AI can assist in
creating more effective treatment plans that are specifically tailored to the
genetic, phenotypic, and lifestyle factors of individual patients [22,23].
The necessity and justification for AI in radiation oncology extend beyond these
practical improvements. The complexity and variability inherent in cancer
treatments require sophisticated decision-making tools capable of analyzing vast
amounts of data in real time—capabilities that surpass human limits. AI
excels in integrating and interpreting multi-dimensional data from various
imaging modalities and patient records, significantly enhancing clinical
decision-making. This reduces errors and improves treatment outcomes.
Additionally, AI supports continuous learning and adaptation in treatment
protocols, allowing them to evolve with new medical insights and tailored to
individual patient responses. Therefore, the integration of AI not only enhances
efficiency but also elevates the standard of personalized patient care,
rendering it an essential component in contemporary radiation oncology.
Objectives
This review provides a comprehensive overview of the current state of AI
integration in radiation oncology, exploring both the benefits and challenges
associated with its implementation.
Go to : 
Ethics statement
As this study is a literature review, it did not require institutional review board
approval or individual consent.
Go to :
Opportunities for artificial intelligence integration
Treatment planning
AI offers significant opportunities in various facets of radiation oncology, such
as treatment planning, image analysis, adaptive radiation therapy (ART), and
predictive analytics. In these domains, AI can enhance clinical workflows,
shorten treatment durations, and deliver more personalized and effective
treatments.
AI can optimize radiation treatment planning by automating complex tasks,
reducing planning time, and enhancing accuracy [24]. Machine learning algorithms can analyze extensive datasets to
identify optimal treatment parameters, potentially leading to personalized
treatment plans that maximize efficacy while minimizing side effects [25]. Over the past few decades, AI has been
progressively integrated into radiation treatment planning. Initially, simple
rule-based systems supported clinical decision-making. As computational power
and data availability have increased, more sophisticated machine learning
algorithms, including artificial neural networks, have been developed. These
algorithms, which initially supported basic tasks, have now evolved to handle
complex treatment planning scenarios. Current research in AI for radiation
treatment planning focuses on developing algorithms that can analyze large
datasets to identify optimal treatment parameters. Machine learning models are
trained using historical treatment data, patient outcomes, and imaging data to
enhance the precision and accuracy of treatment plans [26]. Studies have demonstrated that AI can significantly
reduce the time required for planning while maintaining or improving the quality
of the plans. Research is also exploring how to integrate AI with ART to
continuously update treatment plans based on real-time patient data [27]. The automated generation of radiation
fluence is a critical component of treatment planning, determining the intensity
and distribution of radiation beams to achieve the desired dose distribution
within the target area while sparing healthy tissues. AI has played a crucial
role in improving the accuracy and efficiency of fluence map optimization. Deep
learning techniques can predict optimal fluence patterns based on
patient-specific anatomical and dosimetric data, reducing the complexity and
time required for manual adjustments [28,29].
Several commercial products have incorporated AI into radiation treatment
planning. For example, Varian's Ethos Therapy [30,31] and
Elekta's MOSAIQ Plaza [32] utilize
AI to improve treatment planning and adaptive therapy. These systems automate
aspects of the planning process, optimize dose distribution, and adjust
treatment plans in response to anatomical changes or variations in tumor size
during treatment.
Image analysis
AI-driven image analysis can significantly enhance the accuracy of tumor
detection and segmentation [33]. Deep
learning algorithms are capable of processing imaging data from various
modalities, including CT, MRI, and PET scans, to provide precise tumor
delineation, which is crucial for effective radiation targeting [34,35]. The journey of AI-based image analysis in radiation oncology is
marked by significant milestones. Initially, basic image processing techniques
were employed to improve image quality and enhance tumor visualization. With the
advent of machine learning, more advanced algorithms were developed to automate
tumor detection and segmentation tasks. Early methodologies heavily relied on
handcrafted features, but they were soon surpassed by deep learning algorithms
capable of autonomously learning features from data [36]. Current research in AI-based image analysis focuses on
increasing the precision and efficiency of tumor detection and segmentation
[37,38]. Deep learning models, particularly convolutional neural
networks, are widely used to analyze imaging data from CT, MRI, and PET scans
[39]. These models have demonstrated
an exceptional ability to distinguish tumors from adjacent healthy tissues,
often surpassing the accuracy and consistency of human experts [40]. Additionally, research in multimodal
image analysis indicates that AI can combine data from various imaging
modalities to enhance diagnostic accuracy and inform treatment planning [41].
The segmentation of tumors and surrounding normal organs is a critical task in
radiation therapy, requiring accurate delineation of tumor boundaries and normal
tissues to ensure effective treatment planning [42]. Manual segmentation is traditionally labor-intensive and prone
to inter-observer variability. However, AI-based segmentation techniques
streamline this process, providing consistent and rapid results. Advanced
algorithms, such as U-Net and its variants, have become the standard for medical
image segmentation, known for their ability to accurately identify tumor
boundaries [43]. These models utilize an
encoder-decoder architecture to capture the complex spatial hierarchies within
images, ensuring precise segmentation. Commercial applications of AI-based image
analysis in radiation oncology are already making an impact. For example, IBM
Watson for Oncology leverages AI to analyze medical images and provide insights
for treatment planning [44]. Similarly,
Varian's ARIA oncology information system integrates AI to enhance
treatment planning and execution [45].
Siemens Healthineers also offers AI-based tools for advanced image analysis and
interpretation within its syngo.via platform [46].
Adaptive radiation therapy
In ART, treatment plans are adjusted based on changes in patient anatomy and
tumor size throughout the course of treatment. AI improves ART by swiftly
analyzing imaging data and making real-time adjustments to the treatment plan,
thus increasing the accuracy and effectiveness of the treatment. The concept of
ART has significantly evolved over the past few decades. Initially, radiation
treatment plans were static and did not accommodate anatomical changes during
the treatment course. As technology progressed, the necessity for more adaptive
approaches became apparent, leading to the development of ART [47]. Early implementations of ART involved
periodic imaging and manual adjustments, which were time-consuming and could not
be performed in real-time. Current research and development in ART focus on
utilizing AI to automate and improve the adaptability of treatment plans [48]. AI-based ART systems employ advanced
imaging technologies, such as daily cone-beam CT scans, to monitor tumor size
and anatomical changes in patients. Machine learning algorithms then analyze
these imaging data to predict anatomical changes and adjust radiation dose
distributions accordingly. This capability for real-time adaptation ensures that
radiation doses are precisely targeted to the tumor, minimizing exposure to
surrounding healthy tissues and enhancing overall treatment outcomes [49–51].
Several commercial products have integrated AI to improve ART. Notably,
Varian's Ethos Therapy system and Elekta's Unity system stand out.
Varian's Ethos utilizes AI to analyze daily imaging and dynamically
adjust treatment plans, offering personalized therapy for each session [49]. Similarly, Elekta's Unity
combines a high-field MRI scanner with a linear accelerator to provide real-time
imaging and adaptation during treatment sessions [52]. These systems mark significant progress in the field
of commercial ART, facilitating more accessible and practical real-time adaptive
therapy. As we look to the future, ART is poised to continue its evolution
through the further integration of AI and advanced imaging technologies.
Predictive analytics
AI can analyze historical patient data to predict treatment outcomes and
potential complications. Predictive analytics can guide clinical
decision-making, allowing for more informed and personalized treatment
strategies [53,54]. The application of predictive analytics in radiation
oncology has advanced significantly over the years. Initially, treatment
decisions were primarily based on empirical data and clinical experience. With
the advent of data collection and storage technologies, large databases became
available, enabling the identification of patterns and correlations through
statistical methods. However, traditional methods were limited in handling
complex, high-dimensional data. Current predictive analytics research focuses on
leveraging AI to analyze large-scale historical patient data [55]. Machine learning algorithms, including
deep learning and ensemble methods, are used to predict various clinical
outcomes, including tumor response, survival rates, and potential side effects.
These models process diverse data types, including demographic information,
genetic profiles, imaging data, and treatment histories, to provide
comprehensive predictions. Studies have shown that AI-based predictive models
can outperform traditional statistical methods in terms of accuracy and
robustness [56].
Several commercial products have integrated AI-based predictive analytics to
support clinical decision-making in radiation oncology. For instance, IBM Watson
for Oncology utilizes AI to analyze patient data and provide evidence-based
treatment recommendations [57].
Similarly, the RayStation treatment planning system employs machine learning
models to predict patient-specific treatment outcomes and optimize treatment
plans [58]. Looking ahead, predictive
analytics is poised to revolutionize clinical practice in radiation oncology.
Researchers are focusing on improving the interpretability of AI models, which
will enable clinicians to better understand and trust their predictions.
Furthermore, the integration of predictive analytics with other AI-based
technologies, such as image analysis and ART, is expected to streamline
treatment workflows and improve efficiency. The adoption of federated learning,
which allows AI models to be trained on data from multiple institutions without
the need to share patient data, is anticipated to improve the generalizability
and reliability of predictive models. The elements discussed in the
"Opportunities for AI Integration" section are depicted in Fig. 1.
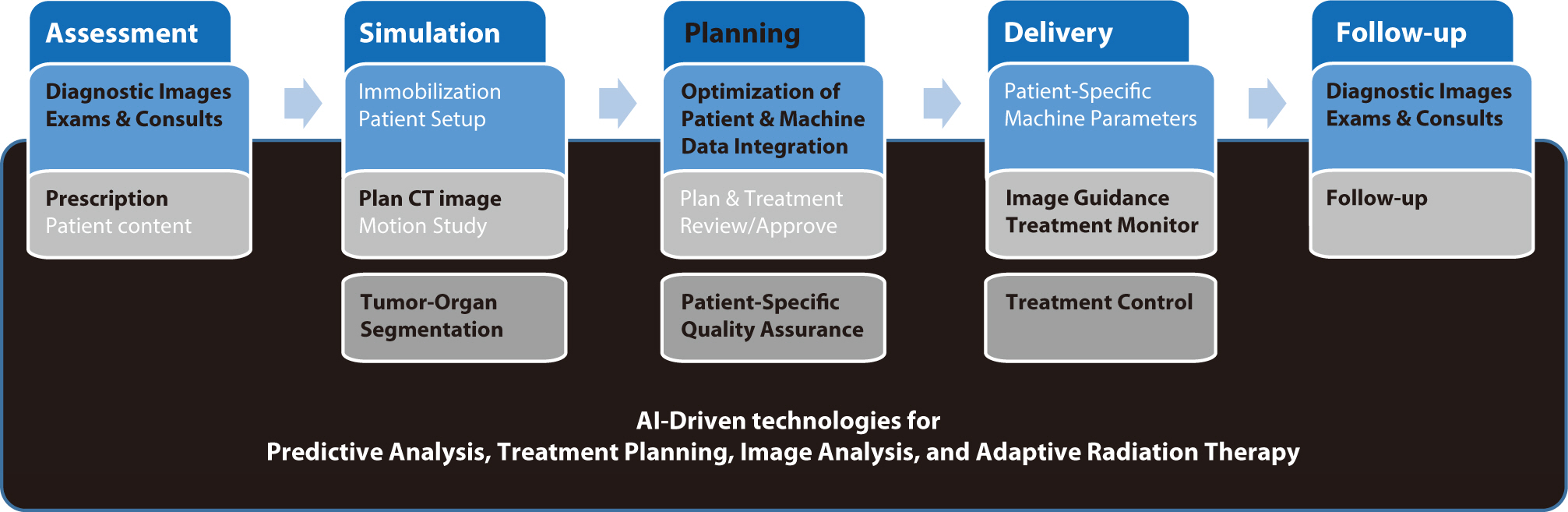 | Fig. 1.The radiation therapy procedures, tasks performed during the procedures, and subsequent related tasks. The black background signifies the aspects related to opportunities for AI integration, indicating that these AI integrations are influencing the entire radiation therapy process. The tasks within the radiation therapy process that are expected to change or be affected by AI in the near future are presented in black text. AI, artificial intelligence.
|
Go to :
Challenges in artificial intelligence integration
Integrating AI into radiation oncology involves multiple challenges that need to be
addressed to fully harness its potential. These challenges encompass technical,
clinical, and ethical aspects, necessitating collaboration among researchers,
clinicians, and policymakers.
Data quality and quantity
The effectiveness of AI models is heavily influenced by the quality and quantity
of the data used for training [59–61]. Challenges
such as inconsistent data quality, missing data, and limited access to large
annotated datasets are significant obstacles [62]. AI algorithms depend on robust datasets that accurately reflect
diverse patient populations and clinical scenarios. However, acquiring such
datasets is often challenging due to privacy concerns, variations in data
collection protocols, and the absence of standardized data formats. Research has
indicated that biases in training data can result in AI models that fail to
generalize effectively across different patient groups. It is crucial to ensure
data quality and to develop techniques for managing missing or incomplete data
to build dependable AI systems. Moreover, large datasets from multiple
institutions are necessary to train models that are effective in various
clinical environments. Collaborative initiatives to share data while
safeguarding patient privacy are vital for the progress of AI in radiation
oncology [63].
Interoperability and standardization
Radiation oncology systems frequently utilize various software and data formats,
which can lead to interoperability issues [64]. To facilitate the seamless integration of AI tools across
different platforms and institutions, it is crucial to standardize data formats
and protocols [65]. The lack of
interoperability may impede the efficient deployment of AI technologies, as it
poses challenges in integrating and analyzing data from disparate systems. These
interoperability challenges are further exacerbated by the use of diverse
imaging modalities, treatment planning systems, and electronic health records in
radiation oncology. Developing common data standards, such as Digital Imaging
and Communications in Medicine (DICOM), is essential for enabling data exchange
and integration [66,67]. Encouraging the widespread adoption of these standards
throughout the industry will help surmount obstacles to AI implementation and
enhance the effectiveness of AI tools in clinical settings.
Regulatory and ethical considerations
Integrating AI into radiation oncology introduces several regulatory and ethical
challenges, including concerns about patient privacy [68], data security, and the necessity for rigorous
validation of AI models. Regulatory frameworks need to adapt to address these
issues and ensure AI is used safely and effectively in clinical settings.
Current regulations may not adequately capture the complexities of AI
technologies, necessitating updates to existing guidelines and the creation of
new standards. Ethical considerations are also paramount in the integration of
AI [69–71]. It is crucial to obtain patient consent and safeguard
data privacy, particularly when handling sensitive health information.
Additionally, the potential for AI to reinforce existing biases in healthcare
must be addressed, as biased algorithms could worsen health disparities.
Developing AI models that are transparent and explainable will foster trust
between clinicians and patients, facilitating their understanding and acceptance
of AI-driven decisions.
Clinical implementation and adoption
Adopting AI tools in clinical settings necessitates significant changes in
workflows and staff training. Resistance to change and skepticism regarding the
reliability of AI can impede adoption [72]. It is crucial to implement comprehensive training programs and
clearly communicate the benefits of AI to overcome these barriers. Research
indicates that involving clinicians in the development and implementation of AI
tools is essential for meeting clinical needs and ensuring seamless integration
into existing workflows [73–75]. Providing ongoing education and
support for healthcare professionals can foster trust in AI technologies and
promote their adoption. Demonstrating the clinical and economic advantages of AI
through pilot studies and real-world applications can also secure support from
stakeholders. The issues discussed in the section "Challenges in AI
Integration" are illustrated in Fig.
2.
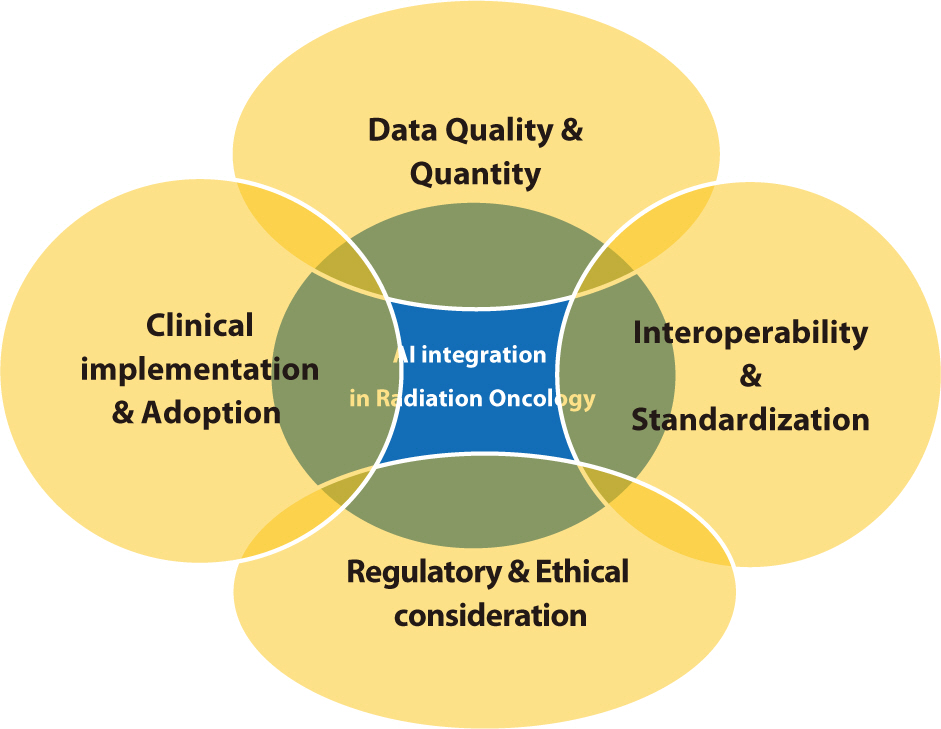 | Fig. 2.The challenges involved in integrating AI into radiation oncology, which are likely to be highly complex and closely interconnected. This indicates the need for careful planning and consideration at an early stage to address these issues before they become entangled. AI, artificial intelligence.
|
Go to :
Future directions
The future of AI in radiation oncology promises significant transformations in
patient care. As AI technologies advance, several critical areas are poised to
propel progress within the field. These areas encompass the creation of more
advanced AI models, the integration of AI with other emerging technologies, the
development of stringent standards and regulations, and a focus on collaborative and
multidisciplinary approaches.
Future AI development will concentrate on creating more sophisticated models that can
manage complex, high-dimensional data [76].
Advances in deep learning and reinforcement learning will enable the creation of
models capable of predicting treatment outcomes with greater accuracy and adapting
to new data in real time. These models will benefit from the ongoing expansion of
available data, including multimodal datasets that integrate imaging, genomics, and
clinical information. These comprehensive datasets will enable the development of
personalized treatment plans specifically tailored to individual patients [77,78].
The integration of AI with other emerging technologies, such as radiomics, genomics,
and wearable health devices, is expected to revolutionize radiation oncology [77]. Radiomics extracts a large number of
features from medical images, which AI then uses to predict disease progression and
treatment responses. Genomics offers insights into the genetic makeup of tumors,
facilitating more targeted and effective treatments [79]. Wearable health devices continuously monitor patients'
health indicators, supplying data that enables AI to dynamically adjust treatment
plans in real-time [80].
To fully realize the potential of AI in radiation oncology, it is crucial to
standardize and ensure interoperability across systems and institutions. The
development and adoption of common data standards, such as DICOM, will facilitate
the exchange and integration of data [81,82]. Additionally, it is
essential to establish standardized protocols for the development, validation, and
deployment of AI models to ensure that these tools are safe, reliable, and effective
[83]. The International Electrotechnical
Commission (IEC) is also working to establish standards that ensure the quality,
safety, and reliability of AI in medical devices [84].
Collaboration among researchers, clinicians, data scientists, and industry
stakeholders is essential for advancing AI in radiation oncology [76,85].
Multidisciplinary teams can leverage diverse expertise to create AI tools that
address clinical needs and integrate smoothly into current workflows [86]. Collaborative research initiatives and
shared databases facilitate the pooling of data and resources, which accelerates the
development of robust AI models [82].
Promoting open science and data sharing while ensuring patient privacy will foster
innovation and advance the field [87].
Developing explainable AI models is crucial for fostering trust between clinicians
and patients [88]. Explainable AI offers
insights into the decision-making processes of AI algorithms, thereby facilitating
clinicians' understanding and validation of AI-based recommendations [89]. Increasing the transparency of AI systems
will address concerns about bias and errors, ultimately encouraging the adoption of
AI technologies in clinical settings [90,91]. AI has the potential to
significantly improve the quality of clinical care while increasing efficiency. For
instance, studies have demonstrated that AI can reduce the time needed for treatment
planning and image analysis, allowing clinicians to devote more attention to patient
care [92,93]. AI-based predictive analytics can identify patients at high risk of
complications, enabling proactive interventions that improve outcomes [94,95].
Moreover, AI's capacity to continuously learn and adapt from new data ensures
that treatment strategies are consistently updated with the latest medical knowledge
and technological advancements [96]. In
clinical settings, AI technologies have the potential to drive several key
advancements in radiation oncology. These advancements include improving diagnostic
accuracy, enabling real-time adaptive therapy, enhancing patient monitoring, and
developing personalized treatment plans, all of which contribute to better patient
outcomes and operational efficiencies [97–101].
Improving diagnostic accuracy: AI-based image analysis increasing the accuracy of
tumor detection and segmentation, thereby improving the precision of radiation
targeting. This increased precision minimizes damage to surrounding healthy tissues
and increases treatment efficacy.
Enabling real-time adaptive therapy: AI rapidly analyzes daily imaging data and
adjusts treatment plans in real time, enhancing the effectiveness of ART. This
capability ensures that radiation doses are precisely targeted to the tumor,
accommodating anatomical changes or variations in tumor size throughout the
treatment course.
Enhancing patient monitoring: Wearable health devices coupled with AI analytics
enable continuous monitoring of patients' health indicators. This allows
timely interventions when adverse changes are detected. Such a predictive approach
aids in managing side effects and enhances overall treatment outcomes.
Developing personalized treatment plans: AI analyzes extensive datasets to identify
patterns and predict individual responses to different treatment modalities. This
capability allows clinicians to create treatment plans that are tailored to each
patient's unique genetic and clinical profile, thereby maximizing efficacy
and minimizing side effects.
Looking ahead, integrating AI into clinical practice in radiation oncology
necessitates careful consideration of ethical, regulatory, and practical issues.
However, the potential benefits, such as improved patient outcomes and operational
efficiencies, make it a worthwhile endeavor. Collaborative efforts among
multidisciplinary teams, the establishment of robust standards, and the continued
advancement of AI technologies will shape the future of radiation oncology,
ultimately transforming patient care. The themes explored in the "Future
Directions" section are visualized in Fig.
3.
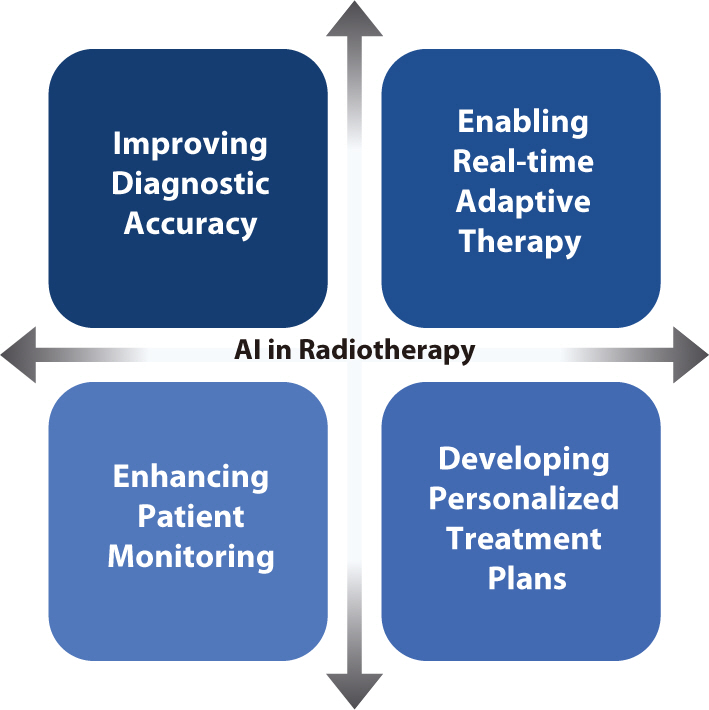 | Fig. 3.Advancements anticipated to result from the integration of AI into radiation therapy. These significant advancements are expected to lead to enhanced diagnostic accuracy, seamless patient monitoring, real-time therapeutic adaptations, and the delivery of highly personalized treatment, thereby substantially improving outcomes for many cancer patients. AI, artificial intelligence.
|
Go to :
Conclusion
The integration of AI into radiation oncology offers significant opportunities to
enhance the precision, efficiency, and outcomes of treatments. As AI technologies
continue to advance, their potential to transform various aspects of radiation
therapy becomes increasingly apparent. This review has highlighted key areas where
AI can make substantial contributions, including treatment planning, image analysis,
ART, and predictive analytics. Each area showcases AI's ability to improve
clinical workflows, shorten treatment times, and deliver more personalized and
effective treatments.
Despite these promising advancements, several challenges must be addressed to fully
realize the potential of AI in radiation oncology. Data quality and quantity are
critical issues because robust and comprehensive datasets are necessary for
effective AI models. Ensuring interoperability and standardization across different
systems and institutions is also essential to facilitate seamless integration and
data exchange. Additionally, regulatory and ethical considerations must be carefully
addressed to protect patient privacy and ensure the safe deployment of AI
technologies in clinical environments.
Collaboration among researchers, clinicians, data scientists, and industry
stakeholders is essential for overcoming these challenges. By forming
multidisciplinary teams, diverse expertise can be harnessed to create AI tools that
not only meet clinical needs but also integrate seamlessly into existing workflows.
Initiatives that promote collaborative research and shared databases will facilitate
the pooling of data and resources, thereby accelerating the development of robust AI
models. Encouraging open science and data sharing, while simultaneously protecting
patient privacy, will drive innovation and advance the field. Moreover, the
development of explainable AI models is crucial for promoting trust between
clinicians and patients. Explainable AI offers insights into the decision-making
processes of AI algorithms, enabling clinicians to more easily understand and
validate AI-based recommendations. Increasing the transparency of AI systems will
address concerns about bias and errors, ultimately encouraging the adoption of AI
technologies in clinical practice.
The future of AI in radiation oncology is bright, and ongoing research and
development are poised to overcome current challenges and unlock new opportunities.
AI-driven improvements in diagnostic accuracy, real-time adaptive therapy, patient
monitoring, and personalized treatment plans are poised to revolutionize the field,
enhancing patient care and operational efficiencies. By emphasizing collaborative
research, continuous learning, and patient-centric approaches, the field can
surmount these challenges and realize transformative advancements in radiation
therapy.
Go to :
 XML Download
XML Download