

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the 2023 statistics, the elderly population in South Korea accounts for 19.2% of the total population, making it one of the countries with a rapidly increasing elderly population on a global scale.12 Alzheimer’s Disease International has reported that an increase in the elderly population contributes to the increasing prevalence of dementia.3 Early diagnosis and early intervention is crucial for the prevention of dementia.
An objective neuropsychological test is essential for the early detection of cognitive decline. A comprehensive neuropsychological test evaluates the examinee’s multiple cognitive functions in areas such as attention, language, visuospatial function, memory, and executive/frontal function. Representative tests commonly used in South Korea include the Seoul Neuropsychological Screening Battery-II (SNSB-II) and the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD-K).45 These tests provide a thorough evaluation of the examinee’s cognitive function. However, due to their long duration of over 30 minutes, they often result in high levels of examinee fatigue. In addition, they require a high level of expertise and skill on the part of the examiner due to the high degree of examiner dependency (human bias) inherent in the assessment process.6 Furthermore, due to the pencil and paper format of the assessment, manual scoring and result analysis are required after the examination, resulting in a lengthy process to obtain results.
In recent years, there has been a growing trend in the development and research of digital neuropsychological tests to overcome various limitations associated with traditional neuropsychological tests. Digital neuropsychological tests allow for more precise control of instructions and stimuli, thereby reducing rater dependence. They allow for more accurate measurements of respondent reaction times and often require less time for scoring and interpretation than traditional paper-and-pencil formats, making them cost-effective.78 In addition, the nature of digital assessments allows for remote testing, facilitating large-scale data collection. Depending on the nature of the task, repeated assessments are possible, which increases the reliability of the assessments and allows for long-term tracking of cognitive function.
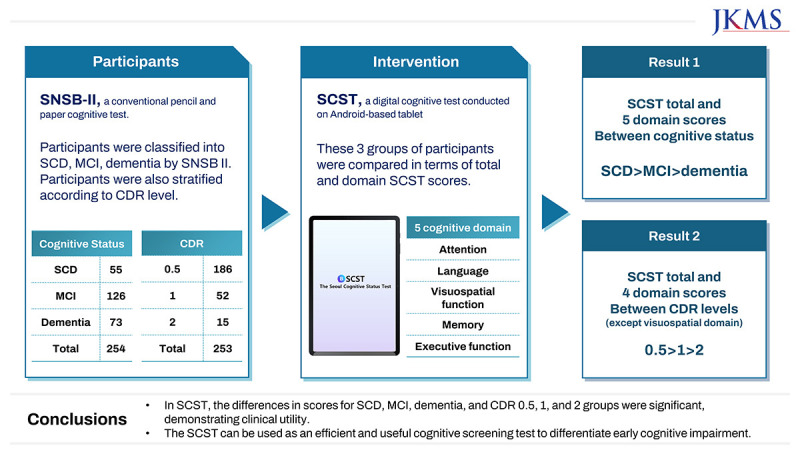
To capitalize on these advantages, a digital neuropsychological test called the Seoul Cognitive Status Test (SCST), formerly called as the Inbrain Cognitive Status Test (CST), has been developed.9 The SCST measures five core cognitive domains (attention, language, visuospatial function, memory, and frontal/executive function) and takes approximately 30 minutes to complete. The test is tablet-based, and respondents answer using voice and a touch screen. Upon completion, most subtests can be scored and analyzed automatically, with the exception of the verbal response. Due to the nature of the digital test, collected data are automatically stored on a server, allowing for the long-term monitoring of participant cognitive function. The economic efficiency, including ease of data storage and reduction of personnel, is expected to be high, especially when conducting large-scale sample studies in hospital and community settings.
The preliminary study of the SCST established norms based on 480 healthy individuals and verified both the validity and reliability of the test.9 It also demonstrated its clinical utility and diagnostic accuracy by confirming a high correlation between the subtests of the widely used comprehensive neuropsychological assessments, SNSB-II and CERAD-K, and those of the SCST.91011 While the preliminary study compared the performance of the SCST across SCD, MCI, and dementia, the sample size was limited. Therefore, the current study aims to increase the sample size and compare the performance of the SCST across SCD, MCI, and dementia, seeking to reaffirm its validity. In addition, this study aims to validate clinical utility by analyzing the variations in SCST scores according to the Clinical Dementia Rating (CDR) which is widely used as an indicator of cognitive impairment stages.12
METHODS
Participants
The study included participants aged 50 years and older who presented for dementia evaluation at a neurology clinic in Gangnam-gu, Seoul, South Korea. Participants underwent the SNSB-II during the dementia evaluation process and completed the SCST within six months. All participants underwent interviews with experienced neurologists and neurological examinations, which was followed by comprehensive neuropsychological testing (SNSB-II), blood tests, and brain magnetic resonance imaging (MRI). Blood tests were performed to rule out secondary causes of cognitive impairment, and brain MRI was performed to rule out structural abnormalities such as tumors, traumatic brain injury, and hydrocephalus.
Participants were classified into three groups (subjective cognitive decline [SCD], n = 55; mild cognitive impairment [MCI], n = 126; and Dementia, n = 73) based on the results of the SNSB-II and an activities of daily living scale, independent of the SCST results. SCD criteria, based on the definition of Molinuevo et al.,13 included continuous subjective cognitive decline compared with the past, normal performance on all neuropsychological tests, and absence of explanation by other psychiatric or neurological conditions. MCI criteria were based on Petersen’s diagnostic criteria, taking into account subjective cognitive complaints, objectively observed cognitive decline, preserved global cognitive function, normal activities of daily living, and absence of dementia.14 The MCI group consisted of 120 amnestic MCI (aMCI) and 6 non-aMCI participants. A diagnosis of aMCI required 1.0 standard deviation (SD) below appropriate norms on either verbal or visual memory tests in SNSB-II. Non-aMCI was those who scored within the normal range on the memory test but 1.0 SD below in any of a series of non-memory cognitive tests (language, visuospatial, executive function). Dementia was diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria, including participants with Alzheimer’s disease (AD) or subcortical vascular dementia.15 Subcortical vascular dementia followed the CREDOS diagnostic criteria.16 Participants with other degenerative diseases (frontotemporal dementia, idiopathic Parkinson’s disease, Lewy body dementia, progressive supranuclear palsy, corticobasal degeneration) and treatable or secondary dementia were excluded. The majority of participants were considered to have AD spectrum dementia or subcortical vascular cognitive impairment.
SCST
The SCST, formerly called Inbrain CST, is a digital cognitive function test based on a 12-inch Android tablet (Galaxy Tab S7Fe, SM-T733; Samsung, Suwon, Korea). SCST consists of seven subtests that assess five core cognitive domains (attention, language, visuospatial function, memory, executive function). The subtests include various tasks such as the Visual Span Test (VST): forward and backward tasks for attention; the Difficult Naming Test (DNT), the Semantic Word Fluency Test (SWFT) and the Phonemic Word Fluency Test (PWFT) for language; the Block Design (BD) for visuospatial function; the Word Place Association Test (WPAT): immediate recall (IR), delayed recall (DR), word recognition (WR), place recognition (PR) tasks and time orientation questions for memory; the Korean version Trail Making Test for the elderly (K-TMT-E): part A and B tasks for frontal/executive function. Participants respond to questions using touchscreen, drag-and-drop, and voice recording methods, and all subtests, except for verbal responses, are scored automatically. Verbal responses are also automatically recorded and used for scoring after the test is completed. The total test time is approximately 30 minutes. SCST scores are generated based on normative data, taking into account age, education level, and sex.9
The time interval between the SNSB-II and the SCST was limited to no more than six months. However, the order of the two tests was not controlled. We intended to confirm the diagnosis through the SNSB first, and then conducted the SCST to compare performance, which was why 94.88% (n = 241) of participants underwent the SNSB first. Meanwhile, 13 participants (5.12%) took the CST first because their SNSB was scheduled within a few weeks, and we conducted the CST in advance to avoid patient fatigue from taking both tests on the same day. Among those who took the CST first, the group distribution was 5 SCD (9.09%), 5 MCI (3.97%), and 3 dementia (4.11%) participants. A χ2 analysis showed no significant difference in the distribution of these three groups.
SNSB-II
The SNSB-II is a comprehensive neuropsychological screening battery that assesses five cognitive domains: attention, language, visuospatial function, memory, and frontal/executive function. The SNSB-II includes the following subtests: the digit span test, the Korean version of the Boston naming test, the Rey-Osterrieth complex figure test, the Seoul verbal learning test, the digit-symbol coding, controlled oral word associated test, the K-TMT-E, and the Korean version of the color word Stroop test.17 SNSB-II scores were standardized with respect to the participant’s age and education level from a nationwide Korean sample population. Administered as a paper-and-pencil test, it takes approximately 1 hour and 30 minutes to 2 hours to complete.
CDR
The CDR is a validated measure to assess the impairment of cognition and function in AD. It assesses six areas of cognition or function: memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care. Scores range from 0 to 3, with 0 indicating no impairment, 0.5 indicating mild cognitive decline, 1 indicating early dementia, 2 indicating moderate dementia, and 3 indicating severe dementia. Participants’ CDR levels were assessed on the same day that the SNSB-II was administered.12
Statistical analysis
One-way analysis of variance (ANOVA) and Pearson’s χ2 were used to compare demographic information and SCST scores among the three groups (SCD, MCI, and Dementia). ANOVA was also used to compare the SCT scores based on the CDR levels. Receiver operating characteristic (ROC) curve analysis was performed to obtain the sensitivity and specificity of the SCST, confirming that it can be a useful tool for differentiating the three groups (SCD, MCI, and Dementia). All analyses were performed using SPSS 24 (IBM Corp., Armonk, NY, USA).
RESULTS
Clinical and demographic characteristics of participants according to SCD, MCI, and Dementia groups or CDR levels
The clinical demographic information of the three groups (SCD, MCI, and Dementia) was compared using ANOVA analysis for age and education. There were no significant differences in age or education between the three groups. However, the Pearson’s χ2 analysis revealed a significant gender difference among the groups, particularly with the highest proportion of females in the SCD group. In addition, there were significant differences in Korean version of the Mini-Mental State Examination (K-MMSE) scores among the groups, with scores decreasing in the order of SCD, MCI, and Dementia.
The same analysis was performed on the clinical demographic information of participants classified by CDR 0.5, 1, and 2. We used ANOVA to compare age and education, and Pearson’s χ2 to compare gender. There were no significant differences for age, education, and gender. Again, significant differences were observed in the K-MMSE scores. Demographic information and K-MMSE scores for the three groups and CDR levels are shown in Table 1.
Table 1
Clinical and demographic characteristics of participants

Comparison of SCST scores among SCD, MCI, and Dementia groups
Analysis of SCST scores using ANOVA revealed significant differences among the three groups (SCD, MCI, and Dementia) in total scores, scores on the five cognitive domains, and scores on individual subtests (Fig. 1). Post hoc analyses showed that performance on most tests followed the order of SCD, MCI, and Dementia. The only exceptions were language (PWFT) and frontal/executive function (K-TMT-part A), where there were no significant performance differences between the SCD and MCI groups. The mean and standard deviation of the SCST scores for the three groups are shown in Table 2.
Fig. 1
SCST total and domain scores in the SCD, MCI, and Dementia groups. (A) Attention score, (B) language score, (C) visuospatial function score, (D) memory score, (E) frontal/executive function score, and (F) total score.
The y-axis represents the raw score for each cognitive domain score and the total score.
SCST = Seoul Cognitive Status Test, SCD = subjective cognitive decline, MCI = mild cognitive impairment.
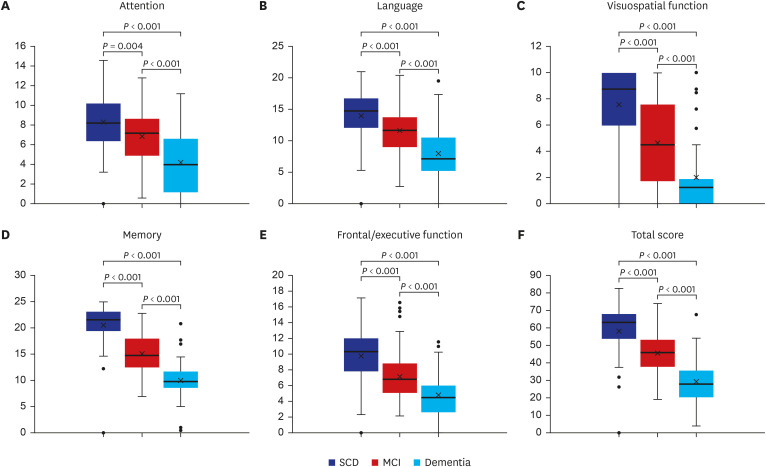
Table 2
SCST individual subtest scores, cognitive domain and total scores in the SCD, MCI and Dementia groups
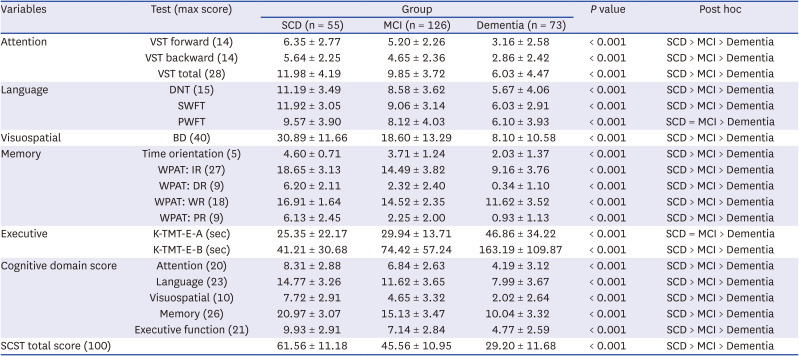
SCST = Seoul Cognitive Status Test, SCD = subjective cognitive decline, MCI = mild cognitive impairment, VST = Visual Span Test, DNT = Difficult Naming Test, SWFT = Semantic Word Fluency Test /fruit/, PWFT = Phonemic Word Fluency Test /’digeut’/, BD = Block Design, WPAT: IR = Word Place Association Test immediate free recall, WPAT: DR = Word Place Association Test delayed free recall, WPAT: WR = Word Place Association Test word recognition, WPAT: PR = Word Place Association Test place recognition, K-TMT-E = Korean version Trail Making Test for the elderly.
Comparison of SCST scores across the groups with different CDR levels
Analysis of SCST scores based on CDR levels using ANOVA revealed significant between group differences in total scores, as well as scores in the five cognitive domains and individual subtests (Fig. 2). Post hoc analyses revealed significant differences between CDR 0.5, 1, and 2 for total score, attention, language, memory, and frontal/executive functions. However, no significant differences were found between CDR 1 and CDR 2 for visuospatial function. When comparing individual subtests, in DNT, PWFT, BD, WPAT-IR, DR, WR, PR, significant differences were found between CDR 0.5 and CDR 1 but the difference between CDR 1 and CDR 2 did not reach significance. PWFT showed no significant differences between CDR 0.5 and CDR 1. The mean and standard deviation of SCST scores based on CDR levels are presented in Table 3.
Fig. 2
SCST total and domain scores according to CDR 0.5, 1, and 2. (A) Attention score, (B) language score, (C) visuospatial function score, (D) memory score, (E) frontal/executive function score, and (F) total score.
SCST = Seoul Cognitive Status Test, CDR = Clinical Dementia Rating.
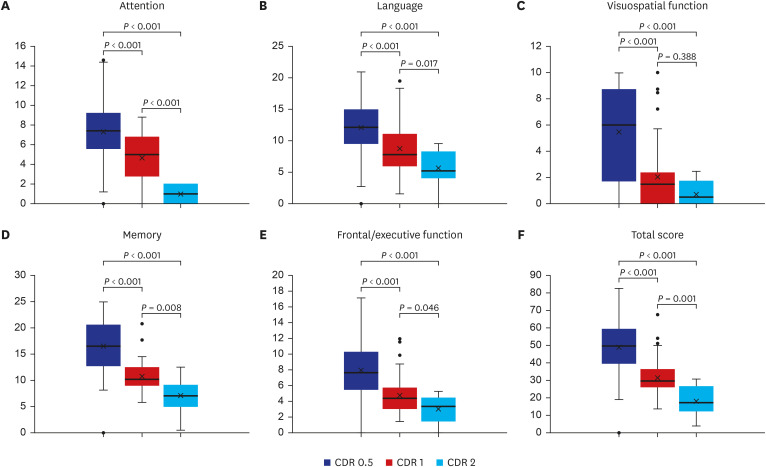
Table 3
SCST individual subtest scores, cognitive domain and total scores according to CDR level
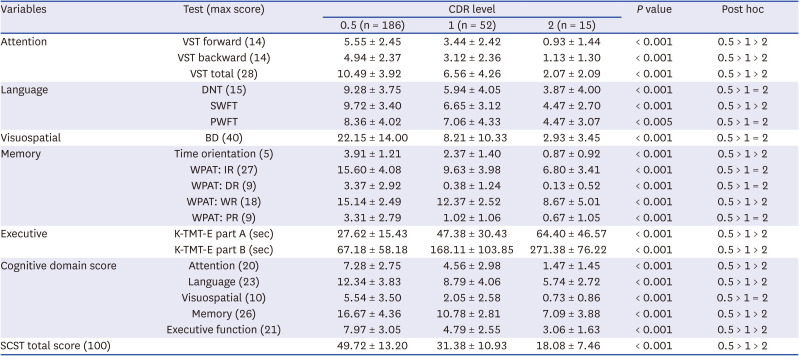
SCST = Seoul Cognitive Status Test, CDR = Cognitive Dementia Rating, VST = Visual Span Test, DNT = Difficult Naming Test, SWFT = Semantic Word Fluency Test /fruit/, PWFT = Phonemic Word Fluency Test /’digeut’/, BD = Block Design, WPAT: IR = Word Place Association Test immediate free recall, WPAT: DR = Word Place Association Test delayed free recall, WPAT: WR = Word Place Association Test word recognition, WPAT: PR = Word Place Association Test place recognition, K-TMT-E = Korean version trail making test for the elderly.
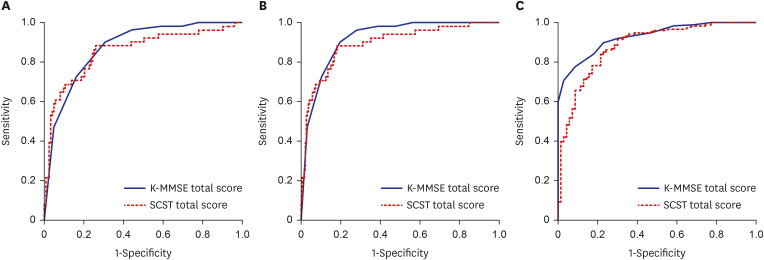
ROC curve analysis of the SCST total score
To determine the power of the SCST total score to discriminate between cognitively impaired individuals (MCI and Dementia groups) and cognitively normal individuals (SCD group), we performed ROC curve analysis and calculated the area under the curve (AUC) (Fig. 3). First, in the comparison of the SCD and MCI groups, the SCST total score had a sensitivity of 0.814 and a specificity of 0.885 with a cut-off total score of 52.07. The AUC of the SCST was 0.854, indicating good discriminatory power. Second, when distinguishing between the cognitively impaired (MCI + Dementia) and the cognitively normal (SCD) groups, the AUC of the SCST total score was 0.894. Using a cut-off total score of 52.07, the SCST total score had a sensitivity of 0.814 and a specificity of 0.885. Lastly, comparing the dementia and non-dementia (MCI + SCD) groups, the AUC for the SCST total score was 0.884, with a sensitivity of 0.786 and specificity of 0.841 when the cut-off total score of 36.47 was applied.
Fig. 3
Compare ROC curves for the SCST total and K-MMSE scores between (A) SCD and MCI, (B) SCD and cognitively impaired group (MCI + Dementia), (C) Dementia and non-dementia group (SCD + MCI).
ROC = receiver operating characteristic, K-MMSE = Korean version of the Mini-Mental State Examination, SCST = Seoul Cognitive Status Test, SCD = subjective cognitive decline, MCI = mild cognitive impairment.
DISCUSSION
The primary aim of this study was to compare SCST scores between SCD, MCI, and Dementia groups as defined by the SNSB-II. Our study of 256 participants showed that the SCST total and five cognitive domain scores were significantly different in the order of SCD, MCI, and dementia, replicating the previous study with a smaller sample size (n = 97).9 Therefore, these results suggest that the SCST, a digital cognitive test that takes only 30 minutes to complete, can discriminate elderly individuals with MCI from those with either normal cognition or dementia.
Furthermore, of the 14 individual subtests that make up the SCST, 12 subtests were able to discriminate the three cognitive groups in the order of SCD, MCI, and dementia. There were two exceptions. First, the phonemic word fluency test showed no significant difference between the SCD and MCI groups. Previous studies have suggested that phonemic word generation is associated with the frontal lobe, whereas semantic word generation is more likely to involve the temporal lobe.181920 MCI, especially the amnestic type of MCI, is known to be a prodromal stage of Alzheimer’s dementia. Therefore, individuals with aMCI in our study may have more pronounced atrophy in the temporal lobe compared with the frontal lobe, suggesting that the relatively intact function of the frontal lobe may have resulted in the preservation of phonemic word generation. Previous studies have also found that participants with aMCI tend to be more impaired in semantic word fluency than in phonemic word fluency.21 Second, the K-TMT-part A did not show significant differences between the SCD and MCI groups. The K-TMT-part A simply requests participants to draw lines from one to fifteen, whereas the K-TMT-part B required participants to alternate between numbers and the days of the week, thus requiring more cognitive demand. Therefore, the low difficulty level of the K-TMT-part A may have resulted in little differentiation between SCD and MCI. Similar results have been reported in other studies as well.2223
The second objective of this study was to compare SCST scores between groups divided by CDR level. Results showed that the SCST total score, most domain scores (attention, language, memory, and executive function domain scores) were significantly higher in the order of CDR 0.5, 1, and 2 groups. Furthermore, most subtest scores also showed significant differences between CDR levels. However, in the visuospatial domain and some individual subtests (DNT, PWFT, BD, and WPAT), post hoc analysis revealed significant differences between CDR 0.5 and CDR 1, but not between the CDR 1 and CDR 2 groups. The reason for this lack of significance between the CDR 1 and 2 groups is largely unknown. However, some of these tests, if not all, may have higher difficulty levels compared to others, potentially resulting in a floor effect by the time cognitive decline reaches CDR 1 or 2.2425 Alternatively, the small sample size of the CDR 2 group (n = 15) in our study may have made the differences less significant.
Finally, in order to determine the power of the SCST total score to discriminate between cognitively impaired (MCI and Dementia groups) and cognitively normal (SCD group) individuals, we performed ROC curve analyses. The SCST total score demonstrated high sensitivity and specificity for differentiating among three patient groups: those with SCD from those with MCI or cognitive impairments, and those with dementia from non-dementia. Specifically, the SCST total score was particularly effective in distinguishing between MCI and SCD individuals, indicating its potential utility as an early-stage screening tool for cognitive decline in the elderly. However, the cut-off scores derived from these analyses should not be solely relied upon to determine whether an individual falls into the SCD, MCI, or Dementia group. When differentiating among SCD, MCI, and dementia, it is crucial to consider not only objective measures of cognitive decline but also impairments in activities of daily living as diagnostic criteria.141516 Therefore, while the proposed cut-off scores can provide a useful reference point for categorizing patients into these groups, they are not sufficient on their own to make definitive clinical diagnoses.
This study has several limitations. First, the cognitive status of the participants in this study was classified by the SNSB-II, which may limit the generalizability of the results. Therefore, future studies are warranted to evaluate the performance of the SCST in participants diagnosed by other widely used neuropsychological tests, such as the CERAD-K. Second, the relatively smaller sample size in CDR 2 compared to CDR 0.5 and CDR 1 may have influenced the results, thus future research should balance sample sizes across CDR levels to validate these findings. Third, we did not control the order of SNSB-II and SCST in a randomized manner. Therefore, practice effects cannot be excluded since participants first became familiar with neuropsychological test through the SNSB before taking the SCST. Future studies should verify the validity of the SCST by controlling for practice effects, such as between-person comparisons. Fourth, if we were to recruit a normal group, we should have recruited cognitively normal people with a CDR of 0 instead of SCD. However, since we recruited participants from a clinic where patients visited due to memory complaints or for dementia prevention, the group consisted of individuals with SCD. Consequently, even though they were diagnosed with SCD, their CDR scores were 0.5 or higher. Future studies should reconfirm the results of this study by recruiting an additional group of cognitively normal individuals with a CDR of 0 who do not complain of cognitive decline.
In conclusion, this study reaffirmed the SCST as a test capable of effectively discriminating between SCD, MCI, and Dementia groups. Furthermore, as the first study to compare SCST performance across CDR levels, it demonstrated that the SCST effectively discriminates between mild cognitive impairment and early to mid-stage cognitive decline, suggesting its utility in the sensitive detection of cognitive impairment.
 XML Download
XML Download