

 Citation
Citation Print
Print


Introduction
Background
Mycoplasma and Ureaplasma (Up) species are the smallest bacteria with a diameter of 0.2–0.3 μm and are fastidious [1]. Mycoplasma hominis (Mh), Ureaplasma urealyticum, and Ureaplasma parvum are genital mycoplasmas that colonize up to 80% of sexually mature women and may cause genital infections from asymptomatic infections of the upper genital tract to endometritis, chorioamnionitis, and adverse pregnancy outcomes [1-4]. Therefore, it is important to differentiate true pathogens from colonizers when genital mycoplasmas are detected in nonsterile urogenital specimens [5,6]. Tetracyclines and fluoroquinolones are often used to treat patients. However, the resistance to common antimicrobial agents is increasingly reported [7,8]. The Mycoplasma IST assay (bioMérieux) is a culture-based diagnostic kit for species identification with enumeration and antimicrobial susceptibility tests (ASTs) to diagnose urogenital mycoplasma infections [9,10]. Since the introduction of the international standardization of antimicrobial breakpoints by the Clinical and Laboratory Standards Institute (CLSI) in 2011 [11], a novel version of IST, IST3, has been developed based on CLSI criteria for antimicrobial selection and concentration specific to Mh and Up. Unlike the previous version IST2 (bioMérieux), the IST3 assay is designed to independently test antimicrobial susceptibility for Mh and Up, even in mixed infections [10]. One publication on performance evaluation of the IST3 kit is available [12]; however, a parallel comparison study with IST2 is lacking.
Methods
Study design
It is a parallel study to verify the performance characteristics of the mycoplasma culture kit compared to the present version before introducing the new kit in the clinical laboratory. Therefore, diagnostic accuracy and precision were not evaluated.
Samples
Residual specimens from positive samples tested for cultures and AST of genital mycoplasmas at Asan Medical Center from September 2023 to January 2024, which were anonymized, were included in the study.
Test methods
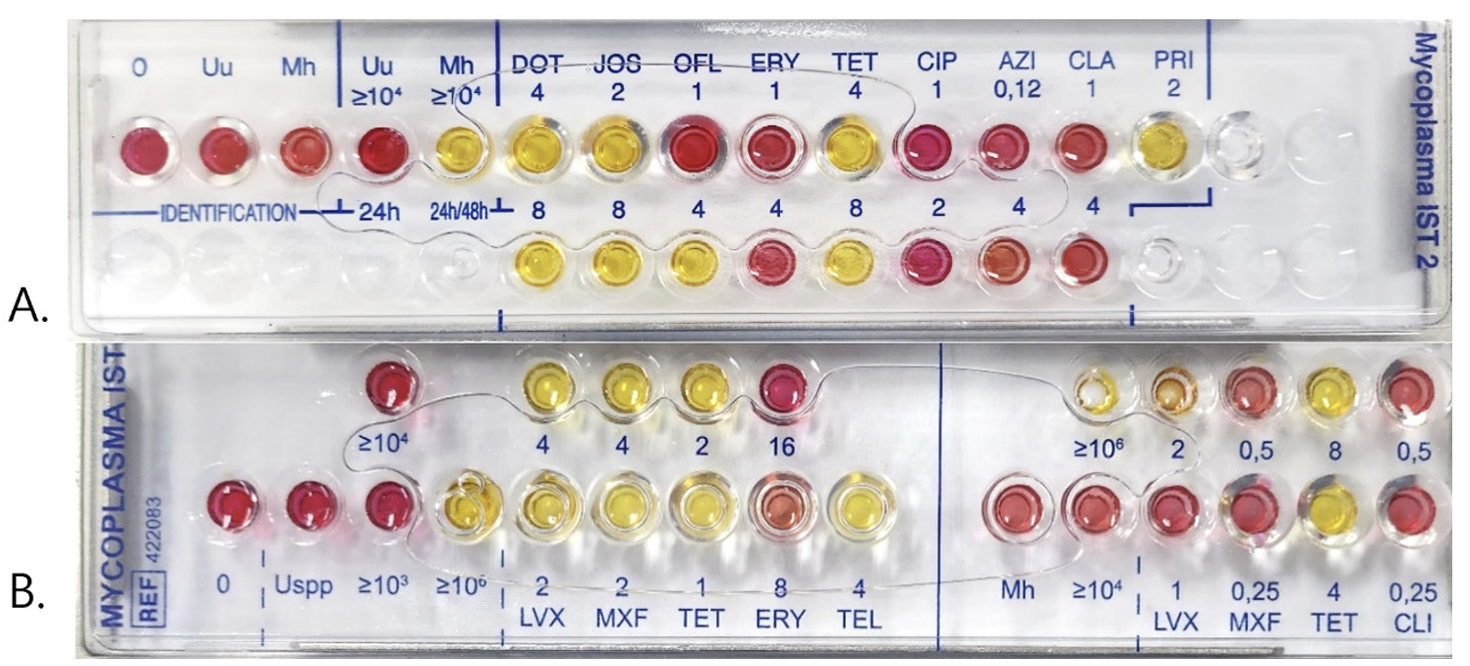
Residual R1 medium after inoculation with the IST2 kit was stored in a refrigerator until the following day, from September 2023 to January 2024. For the collection of culture-positive samples, in which LYO 2 broth became red after 24 h of incubation, 300 μL of residual R1 medium was inoculated into the IST3 kit at a 1:10 (R1:R2) dilution in R2 medium Both kits were read after 24 and 48 h of incubation, as recommended by the manufacturer [9,10]. IST2 contained one concentration well each of ≥ 104 color-changing units (CCU) for quantitation of Up and Mh. AST cupules contained doxycycline, josamycin, ofloxacin, erythromycin, tetracycline, ciprofloxacin, azithromycin, clarithromycin, and pristinamycin and did not distinguish between Mh and Up when mixed. IST3 contained three concentration wells of ≥ 103 CCU, ≥ 104 CCU, and ≥ 106 CCU for quantitation of Mh and two concentration wells of ≥ 104 CCU and ≥ 106 CCU for quantitation of Up. Susceptibilities to levofloxacin, moxifloxacin, tetracycline, erythromycin, and telithromycin were tested for Up and to levofloxacin, moxifloxacin, tetracycline, and clindamycin for Mh (Fig. 1). Because Mh possesses intrinsic macrolide resistance and was mostly mixed with Up, cumulative susceptibility was calculated by dividing the positive samples into two groups: all Mh-positive (Mh+) samples, including Mhonly positive samples, and Up-only positive (Up-only) samples. The AST results of IST2 were interpreted the manufacturer-recommended breakpoints except for the macrolide-intermediate, which was shifted to a susceptibility category, in line with current standard guidelines [11]: ofloxacin ≤ 1 μg/mL, ciprofloxacin ≤ 1 μg/mL, doxycycline ≤ 4 μg/mL, tetracycline ≤ 4 μg/mL, erythromycin ≤ 8 μg/mL, azithromycin ≤ 2 μg/ mL, clarithromycin ≤ 4 μg/mL and pristinamycin ≤ 2 μg/mL, and josamycin ≤ 2 μg/mL [9]. With the IST3 test, the cumulative susceptibilities of Mh- and Up-positive samples were calculated based on the CLSI breakpoints [11]: for Mh, levofloxacin ≤ 1 μg/mL, moxifloxacin ≤ 0.25 μg/mL, tetracycline ≤ 2 μg/mL, and clindamycin ≤ 0.25 μg/mL and for Up, levofloxacin ≤ 2 μg/mL, moxifloxacin ≤ 2 μg/mL, tetracycline ≤ 1 μg/mL, erythromycin ≤ 8 μg/mL, and telithromycin ≤ 4 μg/mL [10]. The AST results were not interpreted if all cupules changed to red.
Analysis
We compared the species, counts, and AST results of the two kits. Because the tested antimicrobials and their concentrations differed between the two kits, very major errors (VME), major errors (ME), and minor errors in IST3 were assessed by comparing the susceptibilities of Mh among Mh+ samples of IST2 and by comparing the susceptibilities of Up among Up-only samples of IST2 at the antimicrobial class level. Therefore, the error rates were calculated for fluoroquinolone classes, tetracycline, and macrolide classes for Up and fluoroquinolone classes and tetracycline for Mh.
Results
Samples
A total of 48 IST2-positive samples were inoculated into IST3: 35 Up-only samples, 1 Mh-positive sample, and 12 samples positive for both Up and Mh.
Test results
Evaluation of the performance of the Mycoplasma IST3 kit compared to the Mycoplasma IST2 kit
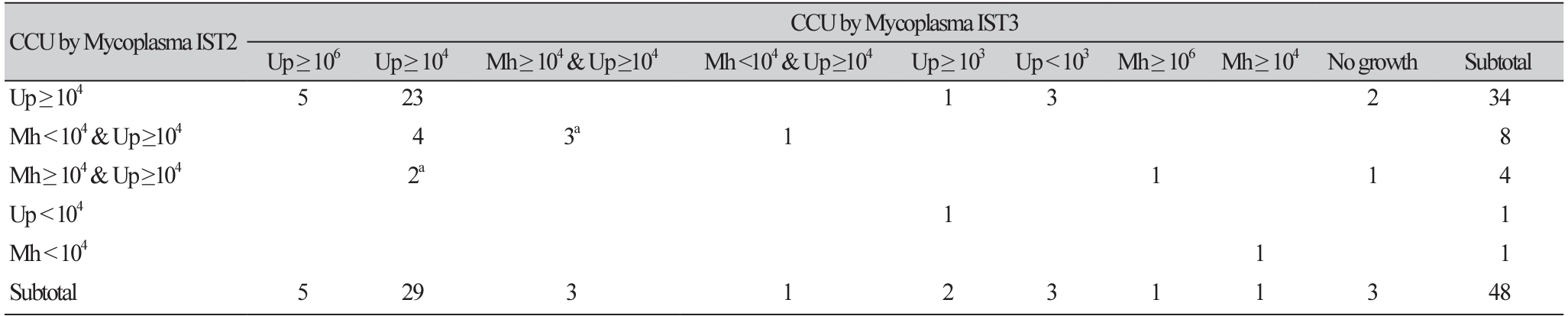
The concentration of all Up-positive samples except one was ≥ 104 CCU, whereas that of Mh was < 104 CCU in nine out of 13 positive samples (Table 1). In one of the samples positive for both Up and Mh, AST could not be interpreted because all the cupules had changed to red. Doxycycline, tetracycline, and pristinamycin were consistently active in 12 Mh+ and 35 Up-only samples, each showing greater than 90% susceptibility.
Cumulative antimicrobial susceptibility using the Mycoplasma IST2 and Mycoplasma IST3 kits
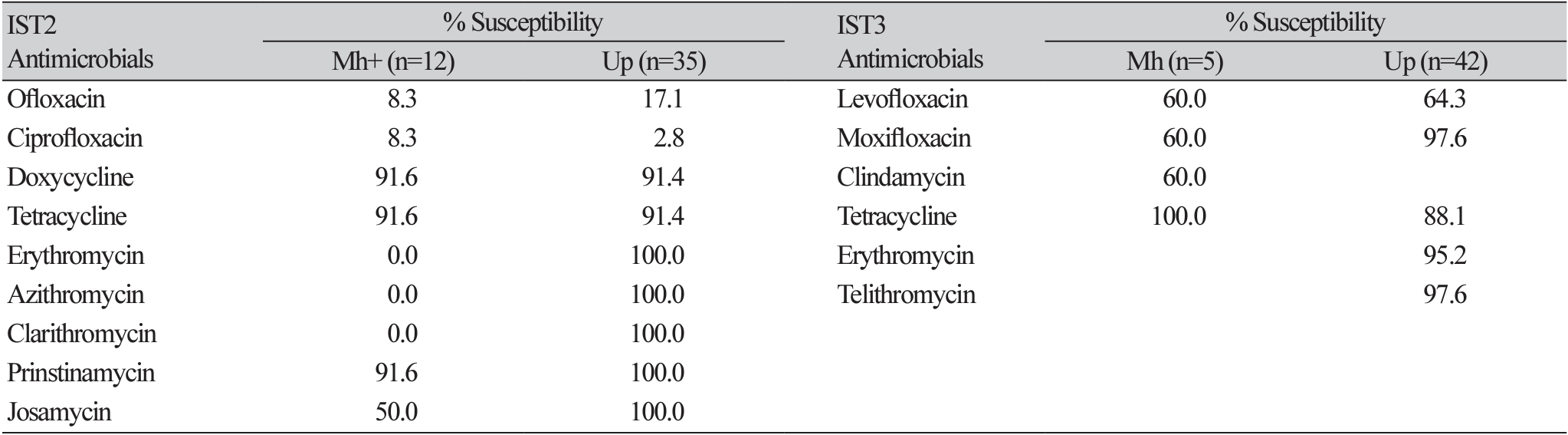
All Up-only samples had minimum inhibitory concentrations (MICs) of ≤ 8 μg/mL for erythromycin, ≤ 2 μg/mL for azithromycin, and ≤ 4 μg/mL for clarithromycin (Table 2). Among the 48 IST2-positive samples, 45 (93.8%) had genital mycoplasmas; 42 (89.4%) of the 47 Up-positive samples and 6 (46.2%) of the 13 Mh+ samples showed growth of the same organisms when tested with IST3. Among the Up-positive samples, 45 samples had Up ≥ 104 CCU with IST2 and 37 (82.2%) of these reproduced at a rate of Up ≥ 104 CCU with IST3. Three of the Up-only samples of ≥ 104 CCU changed to < 103 CCU. All seven Mh+ samples missed by IST3 were mixed with Up ≥ 104 CCU and four of these had Mh < 104 CCU (Table 1). No additional samples positive for Up or Mh were identified with IST3.
Compared to those of IST2, the AST results of 35 Up-only samples by IST3 showed two mismatches, including one ME and one VME in tetracycline and nine VME and one ME in fluoroquinolones. Because the two concentrations of tetracycline were 1 and 2 μg/mL for Up in IST3, which were lower than the 4 and 8 μg/mL contained in IST2, the VME does not account for the discrepancy between the two kits. One ME occurred in the samples where the enumeration of Up changed from ≥ 104 to ≥ 103 CCU and the MIC of tetracycline was 2 μg/mL with a weak color change observed in the tetracycline cupule of 1 μg/mL. All but 2 (95.1%) Up samples were susceptible to erythromycin, and one of the erythromycin-resistant Up samples was also resistant to telithromycin. The AST results for fluoroquinolones between the two kits were not directly comparable because the tested antimicrobials and their concentrations were inconsistent with the CLSI guidelines for IST2. Although 8.3% of the Mh+ and 2.8% of the Up-only samples were susceptible to ciprofloxacin in IST2, 60.0% of the Mh and 64.3% of the Up samples were susceptible to levofloxacin in IST3 (Table 2).
Mismatch for fluoroquinolone susceptibility using the Mycoplasma IST 2 and IST3 kits
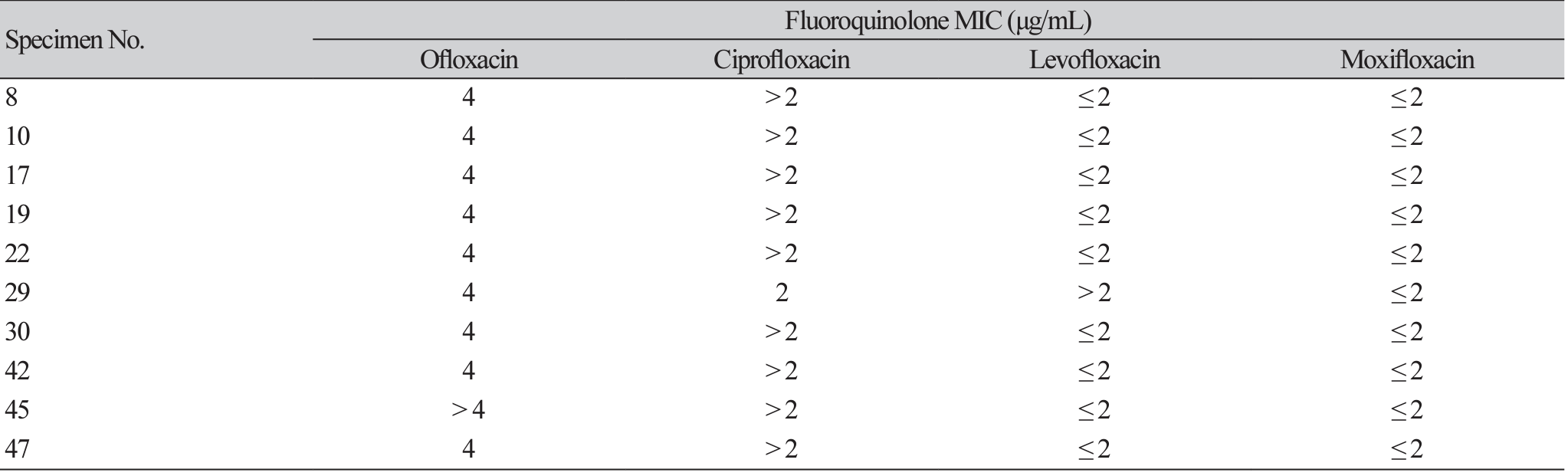
Eight of the nine VME for fluoroquinolones in IST3 occurred in the Up-only group, with an ofloxacin MIC of 4 μg/mL (intermediate). One Up-only sample showed an ME for an ofloxacin MIC of 4 μg/mL and ciprofloxacin MIC of 2 μg/mL, tested by IST2, but for levofloxacin > 2 μg/mL and moxifloxacin ≤ 2 μg/mL when tested by IST3 (Table 3). Two out of five Mh samples were resistant to fluoroquinolones and clindamycin and all were susceptible to tetracycline. There was no mismatch in AST of Mh between IST2 and IST3.
Discussion
Interpretation and comparison with previous studies
The positive results for IST3 correlated well with those for IST2. The IST2-positive samples were also positive with IST3 in 93.8% of samples. The Up-positive samples (10.6%) in which Up failed to grow again, all contained initial concentrations of Up ≥ 104 CCU as enumerated by IST2. Possible causes for this failure in growth may be the loss of viability during storage or the one-tenth dilution of the specimens. Considering that the manufacturer recommends refrigerated storage of samples suspended in R1 media for up to 48 h for IST2 and up to 72 h for IST3 [9,10], the 24-h storage is unlikely to have resulted in deterioration in the viability of Up or Mh. Therefore, sample dilution is more likely to be the cause of the observed failure in growth. When tested with IST2, Mh tended to be identified as mixed with Up, and less than half of these samples were cultured successfully by IST3. A previous study evaluating IST3 showed high sensitivity and specificity for both Up and Mh [12]. In that study, the sensitivity and specificity for Mh was 95.7% and 100%, respectively, compared to that of the standard culture using A7 agar. The results of the present study raise the possibility of false positives for Mh in IST2, because it is difficult to explain the high rate of growth failure with IST3. After introducing IST3 into the laboratory, the overall culture positivity rate remained at 24%–25% over the previous 3 months without significant changes; however, mixed infections positive for both Up and Mh among all positive samples decreased from 14.4% to 1.9%, and the proportion of Mhpositive samples also decreased from 15.5% to 1.9% (unpublished data). Polymerase chain reaction (PCR)based kits detect genital mycoplasmas more than twice as frequently as with IST [13,14]. Up accounted for 30%, whereas Mh and Mycoplasma genitalium accounted for 3.1% of all PCR-positive sexually transmitted pathogens in Korea [13]. Considering the ratio of Up and Mh by PCR, a significant proportion of mixed infections of Mh and Up may be false positives for Mh owing to the high load of Up, which may overcome the inhibitory effects in Mh-enumerating cupules in IST2.
The enumeration of Up with IST2 was reproducible with IST3 as 82.2% of Up samples with a load ≥ 104 CCU were also identified as having a load ≥ 104 CCU in IST3. This result was comparable to that of a previous study that compared IST3 to standard agar culture and reported an agreement of 83.7% for M. hominis and 86.3% for Up [12]. The change in bacterial load in three Up-only samples from ≥ 104 CCU to < 103 CCU and growth failure in four Up samples can be explained by the sample dilution effect. To date, no studies have compared IST2 and IST3 in parallel, as most specimens are swabs transported in R1 medium, leaving no equivalent specimens for repeat testing. In the present study, the R1 broth refrigerated after inoculation was successfully used for parallel testing to compare the performance of the old and new versions of the IST assay kit. It is necessary to perform parallel tests using patient samples when a new culture system is introduced to assess the performance specifications of the new system in a clinical laboratory. The residual R1 transport broth is a reasonable alternative to the swab itself.
When the performance of IST3 for ASTs in comparison to that of IST2 was evaluated for tetracycline and macrolide susceptibility of Up-only samples, two mismatches were observed: one ME and one VME in tetracycline. The occurrence of one VME was defined by the categorical interpretation results of each of the two systems; however, the MIC results were not discordant because the tetracycline concentrations tested were different. The result of one ME was from a sample that was diluted from ≥ 104 to ≥ 103 CCU, and the tetracycline MIC changed from > 8 μg/mL to 2 μg/mL. This ME was probably caused by a decrease in the bacterial load, which was inadequate to detect tetracycline resistance. Therefore, parallel testing using the residual R1 medium carries the risk of VME owing to sample dilution when the bacterial load in the original sample is close to 104 CCU. All five Mh samples tested were susceptible to tetracycline, which is consistent with the results of IST2. Tetracycline and doxycycline susceptibilities vary geographically [7,8], and in Korea, tetracycline susceptibility is reported to be 71.4%–100% and 81.0%–96.2% for Mh and Up, respectively [3,15-17]. The tetracycline susceptibilities in this study were consistent with those reported in previous studies. However, two erythromycin-resistant Up samples were found in two mixed infection samples with IST3. Macrolide resistance is often considered as a contributor to Mh in mixed cultures. Furthermore, one of the erythromycin-resistant Up samples was also resistant to telithromycin, which suggests acquired resistance to macrolide-lincosamide-streptogramin-ketolide class drugs, because telithromycin has not been used in Korea. Erythromycin is the primary drug for AST of Up, but macrolide resistance due to mutations in 23 rRNA and L22 ribosomal proteins is not rare in Korea [15]. The erythromycin AST is essential, especially in neonatal infections, as shown by a fatal case of erythromycin-resistant Ureaplasma meningitis in a premature infant treated with erythromycin in Korea [18]. The IST2 kit overestimates resistance in a mixed cultures containing Mh, which is inherently resistant to macrolides, and Up, which is inherently resistant to lincosamides [12]. Therefore, IST3 has a great advantage in that it can be used to independently test the AST of Mh and Up, even in mixed infections. IST2 also lacks the ability to determine whether the bacterial load, internationally set between 104 and 105 CCU, is compliant with the resistance threshold concentrations validated by the CLSI [11]. Therefore, nine VME and one ME of fluoroquinolones appeared to occur because IST2 used drugs that are less active than the standardized fluoroquinolones to test for levofloxacin and moxifloxacin. The susceptibility rates for ofloxacin and ciprofloxacin (17.1% and 2.8%, respectively) were similar to those of a previous study that collected the largest-scale data using IST2 over 3 years from 2016 to 2018 in Korea, showing susceptibilities of 18.7% and 6.0% for ofloxacin and ciprofloxacin, respectively [17]. Sequence analysis of gyrA, gyrB, parC, and parE detected amino acid mutations in only half of the ciprofloxacin-resistant Ureaplasma parvum isolates tested using IST2 [15]. Therefore, susceptibility of Up to fluoroquinolone seems to be biased toward greater resistance with IST2 [8,17]. Unlike conventional AST, which uses cultured bacteria, IST uses direct samples. Standardized AST for genital mycoplasmas is needed not only for patient care but also for monitoring the regional epidemiology of acquired antimicrobial resistance [17].
Limitations
First, this study was designed as a parallel test using residual R1 broth instead of swab specimens. Furthermore, R1 broth was stored at 4℃ for 24 h and then used with a one tenth dilution. Therefore, when the culture was repeated with IST3 using residual R1 medium, the reason for missing four Up- and six Mhpositive samples was inferred to be the dilution effect or false-positive Mh testing by IST2. Viability loss of genital mycoplamas in R1 medium after sample inoculation is unlikely because it should be stable for 72 h at 4℃ [10]. Second, a relatively small number of specimens were included in this study, and the lack of resistant specimens can be a challenge for the validation of AST. However, the aim was to verify the culture performance of IST3, and not to verify or validate the performance of AST. In this study, decreased resistance to fluoroquinolone was anticipated with IST3. Third, this study did not include negative samples from IST2, and no standard agar cultures were performed; therefore, clinical sensitivity and specificity could not be determined. Given these limitations, this study is the minimum verification required to demonstrate non-inferior performance to IST2 for the introduction of an updated version of the IST. This study presents a reasonable design for verifying a new method for genital mycoplasma culture and AST in clinical laboratories, considering that it has already been thoroughly validated for approval as an in vitro diagnostics [12].
 XML Download
XML Download