

 Citation
Citation Print
Print


Introduction
Background
Dengue fever is a mosquito-borne disease caused by dengue virus (DENV). DENV comprises four antigenically related, but distinct serotypes: DENV-1, DENV-2, DENV-3, and DENV-4 [1]. A newly discovered fifth serotype (DENV-5), closely related to DENV-4, was isolated in Malaysia in 2007 [2]. Genetic analyses revealed that the new serotype (DENV-5) is phylogenetically distinct from the other four serotypes [2,3]. Mild-to-severe infections can occur with one or more of the four serotypes. Infection with any of the four DENV serotypes provides lifelong immunity to that particular serotype, but only temporary immunity against other serotypes [4]. Epidemiological studies have shown that subsequent infections with different DENV serotypes increase the risk of developing severe dengue hemorrhagic fever and dengue shock syndrome [5-9].
The clinical manifestations of DENV infection depend on factors such as the DENV serotype and the immune status, age, and underlying medical conditions of the host [10]. Several studies have described the clinical characteristics of different dengue serotypes. DENV-1 and DENV-4 are associated with milder illnesses, whereas DENV-2 and DENV-3 have been reported as the most prevalent DENV serotypes and are commonly associated with more severe disease [11-14]. Narvaez et al. [15] reported that DENV-2 and DENV-4 cause severe dengue fever as secondary infections, whereas DENV-1 and DENV-3 cause more severe disease as primary infections. DENV-5 has been reported to be responsible for milder illness [2].
DENV is a positive-sense single-stranded encapsulated RNA virus comprising three structural proteins (capsid, membrane, and envelope) and seven nonstructural proteins (NS1, NS2A, NS2B, NS3, NS4A, NS4B, and NS5) [16]. Dengue fever is widely diagnosed using nonstructural protein 1 (NS1), a highly conserved glycoprotein among flaviviruses that is thought to be involved in viral RNA replication [17,18]. Clinical studies have shown that the dengue NS1 antigen is detectable early during the acute phase, up to 9 days after symptom onset, in primary and secondary DENV infections [19-22]. Serological tests using either enzyme-linked immunosorbent assays or immune chromatography-based rapid tests are commonly used to detect anti-DENV antibodies [10,23]. Molecular diagnostic tests, such as real-time reverse transcriptionpolymerase chain reaction (RT-PCR) are regarded as the gold standard for detecting DENV during the acute phase of the disease [24]. PCR-based techniques offer better sensitivity and more rapid turnaround times than viral isolation methods [24]. However, RT-PCR requires expensive equipment, reagents, and well-trained personnel [25], which is impractical in resource-limited settings.
Rapid diagnostic tests for detecting the DENV NS1 antigen have become commercially available and are widely used in countries with limited laboratory resources. Several studies have evaluated the clinical performance of NS1-antigen-based rapid diagnostic tests [26-30].
Objectives
This study aimed to evaluate the clinical performance, including sensitivity and specificity, of the recently developed ImmuneMed Dengue NS1 Ag Rapid I test (ImmuneMed, Inc.) in Korea. Additionally, we evaluated the sensitivity of the tests for different DENV serotypes and when used at different periods from symptom onset to sample collection.
Go to : 
Methods
Study design
It is a diagnostic accuracy study, using retrospectively collected identified serum samples. Index test was a rapid diagnostic test and the reference test was a RT-PCR. It was described according to the STARD2015: An Updated List of Essential Items for Reporting Diagnostic Accuracy Studies available at https://www.equatornetwork.org/reporting-guidelines/stard/.
Serum samples
DENV-positive serum samples were transferred from institutes in foreign countries, including the Instituto de Investigación Nutricional, Peru; the National Institute of Hygiene and Epidemiology, Vietnam; and the University of Health Science, Laos. One hundred DENV-positive samples were obtained, of which 27 were confirmed to be DENV-1 and 72 were DENV-2. The serotype of one of the samples was unknown. In the control group, 161 DENV-negative samples were collected from Koreans who underwent health checkups and did not travel overseas lately.
Test methods
Rapid diagnostic tests
Before the experiment, the positive and negative serum samples were randomized. The clinical performance was evaluated using these serum samples. The ImmuneMed Dengue NS1 Ag Rapid I test was performed according to manufacturer’s instructions. Briefly, two drops of serum were added to the device, and two drops of sample diluent were immediately added to the sample well. The results were interpreted visually after 20 min. If only the control band (‘C’) was stained, the test result was interpreted as negative, whereas if both the control and test bands (‘C’ and ‘T’) were stained, the test result was considered positive for DENV NS-1 antigen. Other staining patterns were considered invalid.
RT-PCR
The AccuPower® ZIKV (DENV, CHIKV) multiplex real-time RT-PCR kit (Bioneer) was used to confirm the presence of DENV. Briefly, viral RNA was extracted from serum samples using ExiPrep™ 48 Dx (Bioneer), according to the manufacturer’s instructions. RT-PCR was performed using the Exicycler™ 96 (Bioneer) and ExiStation™ Manager software (Bioneer).
Statistical analysis
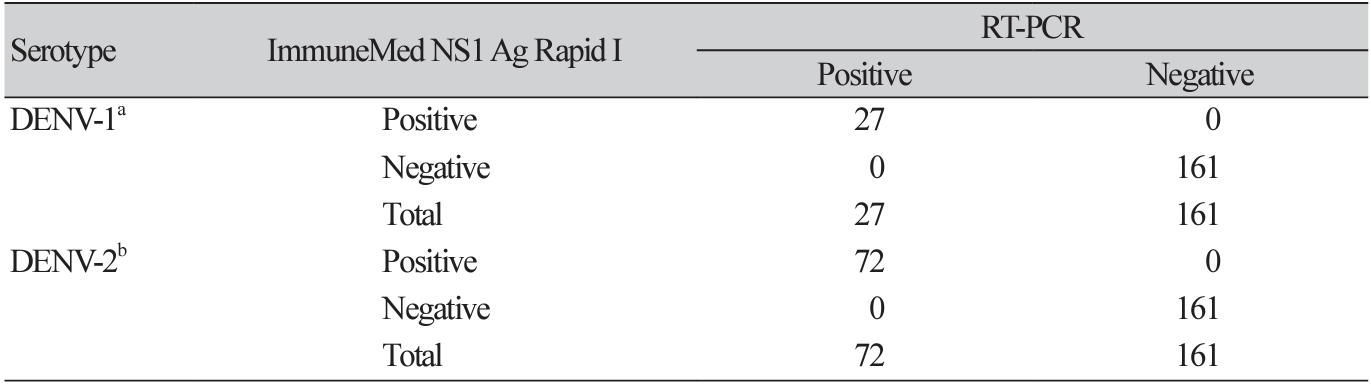
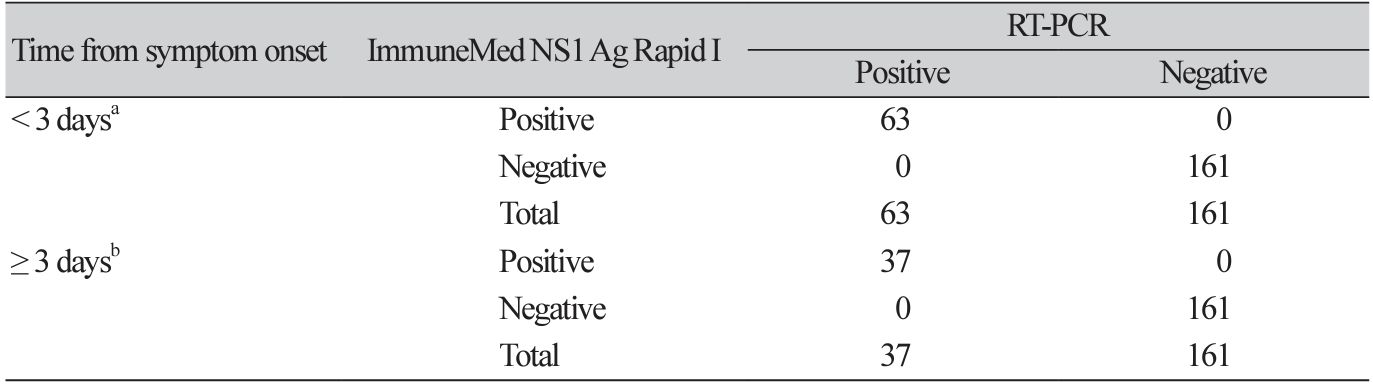
The results of the RT-PCR tests were defined as the gold standard. Standard diagnostic accuracy indices of sensitivity and specificity with corresponding 95% confidence intervals (CI) were calculated. We assumed that the serotypes of DENV and the period from symptom onset to sample collection might affect the performance of the ImmuneMed Dengue NS1 Ag Rapid I test. Therefore, we stratified the DENV positive samples according to serotypes (DENV-1 and DENV-2) and the period from symptom onset to sample collection (< 3 days and ≥ 3 days). We also calculated sensitivity and specificity in restricted subjects, including all negative and stratified positive subjects. All statistical analyses were performed using R software (R version 4.3.3).
Go to :
Results
Overall, the results of the ImmuneMed Dengue NS1 Ag Rapid I and RT-PCR tests showed strong agreement. The sensitivity and specificity were 100% (95% CI, 96%-100%) and 100% (95% CI, 98%100%), respectively. Analyses of the clinical performance of the ImmuneMed Dengue NS1 Ag Rapid I and RT-PCR test are shown in Table 1. The samples were then grouped based on DENV serotype. The clinical performance of the ImmuneMed Dengue NS1 Ag Rapid I test for the DENV-1 and DENV-2 serotypes was also excellent (Table 2). We further evaluated the performance of the ImmuneMed Dengue NS1 Ag Rapid I test at different periods, from symptom onset to sample collection (< 3 days and ≥ 3 days). The sensitivity and specificity were 100% for each subgroup, as defined by clinical presentation at the time of sampling (Table 3).
Go to :
Discussion
Key results
Present study proves that the rapid diagnostic tests are useful for the detection of DENV, as they allow for the quick identification and isolation of suspected patients before RT-PCR results are available, especially in low- and mid-income countries or resource-limited settings.
Interpretation/comparison with previous studies
Rapid diagnostic tests, which can be performed near a patient’s point-of-care, are widely adopted because of their practicality in preliminary diagnosis of dengue fever. Rapid assays that offer results within 15–30 min of sampling are highly desirable, particularly in cases where resources are limited or in remote settings. Several studies have evaluated the clinical performance of NS1 rapid diagnostic tests [31,32]. In this study, we evaluated the clinical performance of a commercial rapid diagnostic test, the ImmuneMed Dengue NS1 Ag Rapid I test, using sera collected from patients with confirmed dengue fever abroad and from healthy controls in Korea. Statistical analysis showed 100% sensitivity and 100% specificity, which is comparable to a previous study, in which the sensitivity and specificity were 97.4% (95% CI, 95.5%–99.5%) and 96.6% (95% CI, 93.2%–98.4%), respectively [30]. The agreement between the Immune-Med Dengue NS1 Ag Rapid I and RT-PCR test results was excellent. Both the ImmuneMed Dengue NS1 Ag Rapid I test and the RT-PCR test exhibited similar sensitivities (100%) for the detection of different serotypes of DENV and for serum samples collected either less than or more than 3 days after symptom onset. The strength of this study is that we performed the rapid NS1 Ag and RT-PCR tests simultaneously, which is practical for clinical practice.
Limitations
This study has several limitations. First, we did not evaluate the sensitivity or specificity of the ImmuneMed Dengue NS1 Ag Rapid I test at detecting primary or secondary DENV infections. In addition, 72% (n = 72) of the samples were from DENV-2-infected patients. Owing to the limited number of DENV-1 samples and the absence of DENV-3 and DENV-4, the performance of the ImmuneMed Dengue NS1 Ag Rapid 1 test in detecting all DENV serotypes requires further investigation. Although we attempted to transfer the serum samples at a stable temperature in a frozen state, there might have been a temperature issue during storage or transportation. Nonetheless, the clinical performance of these serum samples was excellent. Furthermore, due to the limited volume of serum available, we were unable to compare with other rapid Ag tests.
Go to :
Conclusion
Above results suggest that the sensitivity and specificity of the Immune-Med Dengue NS1 Ag Rapid test are comparable to those of the RT-PCR test. These results support the use of the ImmuneMed Dengue NS1 Ag Rapid test as a fast, inexpensive, and reliable point-of-care antigen-detection test for the diagnosis of dengue fever.
Go to :

 XML Download
XML Download