

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The efficacy of whitening systems prescribed by dental professionals has stimulated the development of several products with the premise of removing stains and whitening teeth without professional supervision [1]. The “over-the-counter” (OTC) products usually contain low concentrations of peroxides or have abrasives in their formulations to remove extrinsic stains [23]. These OTC products are easily available, less expensive, and do not require a prescription and guidance from a dentist. The objective is to achieve a change in the color of the teeth after 1 to 4 weeks of use [45]. OTC products are available in the form of toothpaste, mouth rinse, dental strips, gels, activated carbon powder, or oil extracts [6].
Mouth rinses have become popular because they are an easy and efficient therapy to aid oral hygiene and act against cariogenic biofilms [7]. Mouth rinses containing hydrogen peroxide have also appeared for whitening teeth. The process of tooth whitening occurs through an oxide-reduction reaction in which hydrogen peroxide decomposes and releases oxygen-free radicals. These radicals penetrate through the micropores of the enamel into the dentin, breaking down the pigments that cause tooth darkening [3]. In other words, tooth whitening alters the color and appearance of teeth that were previously discolored due to intrinsic or extrinsic pigments [4].
Karadas [8] compared the bleaching effect of mouth rinses and 10% carbamide peroxide and observed color changes for all treatment groups compared to the negative control, although the bleaching effects of rinses were significantly lower than those of the 10% carbamide peroxide. However, other studies demonstrated that the active ingredient did not cause substantial whitening because the peroxide mechanism of action depends on the application method, the concentration of the active agent, and the contact time with the dental enamel [9].
Bleaching mouth rinses containing hydrogen peroxide usually present an acidic pH, and some studies reported they can have significant adverse effects in the long term, such as alteration of the enamel surface, which facilitates pigment absorption and tooth sensitivity [1011121314]. The possible risks of their misuse in the oral cavity have stimulated proposals for new formulations containing alternative substances, such as sodium hexametaphosphate, tetrasodium pyrophosphate, phthalimido-peroxy-caproic acid, and natural extracts [515].
The use of natural extracts is a sustainable biotechnology. Natural extracts have been used for medicinal purposes for several decades and are a promising means of developing new drugs and cosmetics [161718]. An alternative method would be the use of enzymes for tooth whitening, the first of which appeared in 1960, using fungal proteolytic enzymes, and since then many patents have been created. Enzymes are excellent catalysts and act under ideal pH and temperature conditions, reducing the adverse effects of the environment [1920].
The mechanism of action of whitening enzymes is based on 2 hypotheses: 1- proteolytic enzymes capable of removing the acquired film, promoting a whiter appearance, and 2- specific action of enzymes capable of degrading the compounds present in the dental structure and altering the color [21].
The ligninolytic enzymes in fungi, such as the mushroom Pleurotus ostreatus (P. ostreatus), demonstrate great interest in science and industry because their enzymes can degrade and mineralize some compounds in dyes [17]. This fact inspired researchers to develop natural and milder teeth whitening formulations [19]. Thus, these enzymes may be a natural and promising alternative with fewer adverse reactions than commercially available whitening mouth rinses. To date, the use of mouth rinses containing natural extracts of autoclaved black shimeji mushrooms (P. ostreatus) for tooth whitening has not been studied, despite the fact that the extract of such mushroom has shown a tooth whitening activity [1718].
In this context, based on this preliminary evidence, this study aimed to develop whitening mouth rinses formulated with industrial mushroom residue, and compare them in vitro with OTC commercial whitening mouth rinses. The null hypotheses tested were: 1) the experimental mouth rinses would not differ from commercial mouth rinses in terms of color analysis (CIELAB [ΔE*], CIEDE 2000 [ΔE00], whiteness index for dentistry [ΔWID]); 2) The studied mouth rinses would not alter the physical property of surface microhardness (SMH; Knoop hardness number [KHN]) of dental enamel.
MATERIALS AND METHODS
Preparation of the formulation
The raw materials used in this study were harmless substances available and authorized for use and are in accordance with the International Nomenclature of Cosmetic Ingredients. For the formulations, black shimeji mushrooms (P. ostreatus), black shimeji mushroom substrate (residue from mushroom production, consisting of corn cobs and mushroom stalks), and black shimeji mushroom stalks were used, according to the technology reported in INPI (BR 10 2020 022728 9) [18]. The mushroom-containing samples were kindly supplied by Hochibra (http://hochibra.com.br/). Figure 1 shows the parts of each mushroom.
Figure 1
Representation of the parts of the mushrooms used in the development of 3 mouth rinses (black shimeji mushrooms; black shimeji mushrooms stalks; black shimeji mushrooms substrate), followed by the rinsing protocol and storage in artificial saliva.
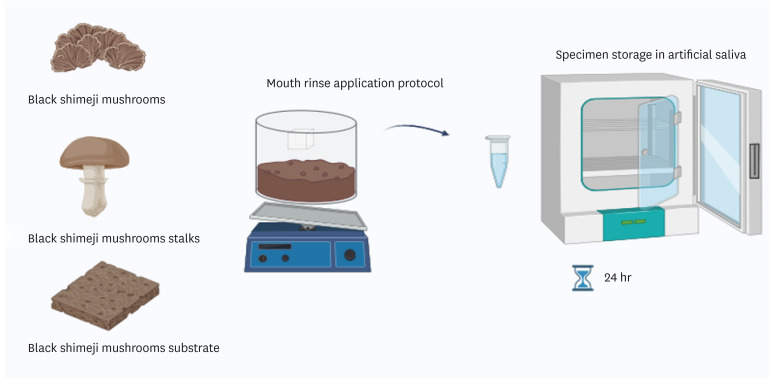
Initially, 70 g of the sample was weighed on an analytical balance (edible part of the mushroom, substrate, and stalk). The mouth rinse formulations consisted of autoclaved black shimeji mushroom (P. ostreatus), black shimeji substrate, and black shimeji stalk. After, reagents were added to this formulation, such as saccharin, sucralose, benzoate, sorbate, sodium metabisulfite, citric acid, sodium lauryl sulfate and R-carvone. After heat treatment, the samples were homogenized with 100 mL of 50 mM phosphate buffer (pH 7.0) using a homogenizer (Ultra-Turrax, T25 digital, IKA Works, Germany) and filtered through gauze. Finally, the solution was mixed in the magnetic stirrer at 600 rpm for 5 minutes second by BR 10 2020 022728 9 [18].
Specimen preparation
After extraction, the bovine teeth used in this study were stored in 0.1% thymol solution (Proderma, Piracicaba, SP, Brazil). Then, the teeth were visually examined to rule out stains and cracks that could interfere with this work.
The debris was removed by manual scraping with scalpel blades. The teeth received a prophylactic cleaning with rubber cups (KG Sorensen, Barueri, SP, Brazil) filled with pumice paste (SS White LTDA, Rio de Janeiro, RJ, Brazil) and water (2:1). Subsequently, the teeth were sectioned at the cervical portion, separating the crown and root, using a rigid double-sided diamond disk (KG Sorensen) under irrigation in a low-rotation micromotor (Kavo, Joinville, SC, Brazil). To obtain the specimens, cuts were made in the coronal portion, in the mesio-distal and inciso-cervical directions, using a metallographic cutter (Isomet, Buehler, Lake Bluff, IL, USA) with a high-precision diamond disk (4’’ × 0.012’’ × 0.5”, Buehler). Thus, the specimens had the dimensions 4.0 × 4.0 mm × 3 mm thickness (1 mm enamel and 2 mm dentin). The dentin surface was ground with #600 silicon carbide sandpaper, and the enamel surface was ground with increasing grain sizes (#600, #1200, #2500, and #4000) under constant water irrigation using a rotary polisher (Arotec, Cotia, SP, Brazil). Then, the blocks were polished with felt discs (TOP, RAM, and SUPRA: Arotec) with metallographic diamond pastes of decreasing grain size (1 µm and 0.25 µm). Between the use of sandpapers and after final polishing, the samples were placed in an ultrasonic cleaner (Marconi, Piracicaba, SP, Brazil) for 10 minutes to remove residual particles.
Two sets of samples were prepared, 1 for color analysis and the other for microhardness analysis. Based on a previous pilot study, the optimum sample size for color analysis (effect size = 0.17; α = 0.05; β = 0.80; correlation = 0.5) and microhardness samples (effect size = 0.20; α = 0.05; β = 0.80; correlation = 0.3) was 10 samples per group. Considering the loss of 20% of the specimens, a total of 70 specimens were selected for each set of specimens (n = 140). For the allocation process, samples with similar SMH values (15% deviation from the total average: 338 KHN) were selected, while the color samples with similar L* values were selected. The specimens were allocated by stratification considering their initial KHN and L* values into 7 different groups.
Staining protocol
The lateral surfaces of the specimens were protected with colorless varnish on the dentin surfaces to not interfere with the whitening treatment of the dental enamel [20]. The tooth blocks were immersed in a solution of black tea, which was changed every 24 hours, for 6 days. The tea solution was prepared by mixing 100 mL of distilled water boiled for 5 minutes and infused with 1.6 g of black tea (Leão Junior S.A., Curitiba, PR, Brazil) for 5 minutes. After immersion in the tea solution, the specimens were stored in an artificial saliva with pH = 7.0 (Ca 1.5 mmol/L; P 0.9 mmol/L; 150 KCl mmol/L; 0.1mol/L TRIS buffer solution) solution for 14 days, with daily saliva changes for color stabilization [22]. Before measurement in the spectrophotometer, the black tea layer that formed on the enamel surface was removed with a pumice stone and water at low rotation. Samples were randomly allocated considering the initial values for the L* parameter [11].
Mouth rinse application protocol
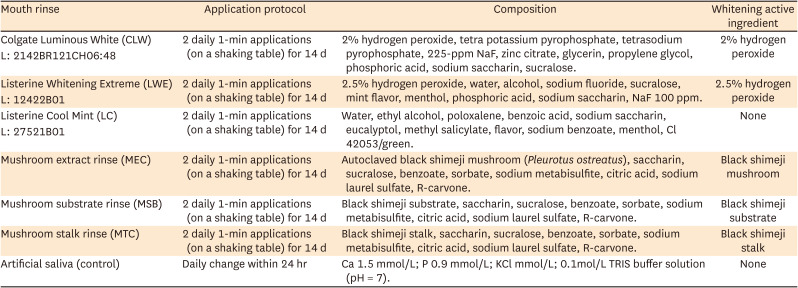
Enamel blocks were positioned in sample holders (20 × 20 mm) with sticky wax and were exposed to 100 mL of mouth rinse solution. Before use, all rinses were shaken (Table 1) [11]. They were used twice daily on a shaking table (SolidSteel, Città Sant'Angelo, Italy, SKU SSAGA10L-110) for 14 days with 10 mL per sample to simulate natural mouth rinse, then rinsed with distilled water for 10 seconds and returned to the artificial saliva (pH = 7) until the next protocol day [11]. Exposure frequency and times followed the Listerine Whitening Extreme (LWE) manufacturer's recommendations, as described in the product's instructions for use. The groups and information about the rinses used are described in Table 1.
Table 1
Mouth rinses treatment groups according to application protocol and composition application
Color analysis
The color was analyzed using a spectrophotometer (CM-700 d, Konica Minolta, Osaka, Japan), calibrated to white and black light before each measurement. To quantify color, the specimens were positioned on a Teflon device (sample holder) and the equipment was fixed so that the readings were always taken at the same point and the device did not move. The readings were taken inside a light chamber (GTI Mini Matcher MM 1e, GTI Graphic Technology Inc., Newburgh, NY, USA) using the "daylight" option to standardize the readings. The color values were obtained according to the Commission Internationale de l’Eclairage (CIE) L* a* b* system which defines the color of an object within the 3-dimensional (3D) color space. The L* coordinate represents the luminosity (white–black) axis, a* the green–red axis, and b* the blue–yellow axis. The differences in the L*, a*, and b* values were read 3 times: before treatment (T1), 24 hours after treatment (T2) and 7 days after treatment (T3), and were expressed as ΔL*, Δa*, and Δb*. The general color change was calculated using the following equation:
For ΔE00, ΔL', ΔC', and ΔH' represent the differences in values in light, chroma, and hue, respectively. SL, SC, and SH are parameters for adaptation coordinate values as a function of color difference variation. KL, KC, and KH are correction parameters concerning experimental conditions, and RT is a parameter that considers the interaction of differences between chroma and hue in the blue region, using the following formula:

ΔWID variation was calculated according to the following formula ΔWID = 0,511L* − 2,324a* − 1,100b*. ΔWID has been used as a measurement of the CIELAB-based whiteness level to analyze the whiteness of dental materials [23].
Surface microhardness assessment
The microhardness of all the specimens was measured initially (baseline) to standardize the groups before they were randomly divided. After the teeth were exposed to the different formulations and treatments, each block was submitted to SMH analysis 24 hours and 7 days after treatment. The SMH was evaluated using a microhardness tester with a Knoop indenter (FM 100, Future-Tech, Kawasaki, Japan). Five indentations (50 gf/5 s) were made in the central area of the specimens with a distance of 100 μm. The mean values of the 5 values obtained from the specimen’s KHN for the time period [24].
Scanning electron microscopy
Surface analysis of the specimens in each group was performed with scanning electron microscopy (SEM) after the in vitro experimental period. Three specimens were randomly selected for each treated group.
The specimens were prepared by dehydration with immersion in ethanol solutions at increasing concentrations (50%, 70%, 90%, 100%, and 100%). After that, they were vacuumed in a cathodic sprayer (SCD 050, Balzers Union Aktiengesellschaft, Balzers, Liechtenstein) to deposit a thin layer of 24K gold on the surface. Then, 4,000× magnitude images of representative areas were obtained using SEM (JSM-5600LV, JEOL, Tokyo, Japan) [24].
Measurement of pH
The pH of the mouth rinse solutions was measured in triplicate after preparation and after treatment. The pH readings of each solution were obtained from 3 measurements taken over a 30-minute interval, and their mean was considered the final value [24]. This analysis aims to determine whether the solutions were acidic, neutral, or alkaline. The pH was measured with a digital pH meter (PHS-3B; Phtek, São Paulo, SP, Brazil).
Statistical analysis
Color and microhardness data did not meet the assumptions of a parametric analysis, non-parametric tests were employed subsequent to descriptive and exploratory analyses. These analyses included assessments for homogeneity of variance, quantile–quantile plots, and the Shapiro–Wilk tests. Next, a generalized linear mixed model for repeated measures in time was fitted to analyze SMH. ΔE*, ΔE00, and ΔWID were analyzed by generalized linear models considering the group effects in T1 (before treatment), T2 (24 hours after the application), and T3 (7 days after the application) via the R program (R Core Team; Computing, Vienna, Austria), with a significance level set at 5%.
RESULTS
Color analysis
CIELAB values are presented in Table 2. When comparing T1 × T2, it was observed that the mean ΔE* values were significantly higher in the mushroom substrate rinse (MSB) and LWE groups than in the Colgate Luminous White (CLW), Listerine Cool Mint (LC), and artificial saliva groups (p = 0.0355), which demonstrated variation considering the 3D parameters “L*”, “a*”, and “b*”. When comparing T1 × T3 ΔE* the highest values were found for LWE and MSB (p = 0.0076).
Table 2
Color variation as a function of group and time (CIELAB [ΔE], CIEDE 2000 [∆E00], and whiteness index for dentistry [∆WID])
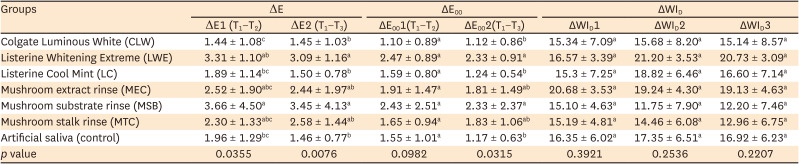
Values are presented as mean ± standard deviation.
Generalized linear models considering the group effects in T1 (before treatment), T2 (24 hours after the application) and T3 (7 days after the application).
Different letters indicate statistically significant differences vertically (within the time of treatment) (p > 0.05).
As for the analysis of ΔE00 (Table 2), when comparing the initial (T1) with 24 hours after treatment (T2), there was no significant difference for all groups (p = 0.0982), and there were also no differences compared to the artificial saliva group. In the comparison between T1 × T3, the highest values were found for LWE and MSB (p = 0.0315).
As for ΔWID, the highest numerical mean value was observed for mushroom extract rinse (MEC) in T1 (p = 0.3921). In T2 and T3, the group LWE showed the highest values, followed secondly by MEC (p = 0.2536; p = 0.2207, respectively). However, no significant differences were found between the groups for any of the times studied (Table 2). Mouth rinses with low concentrations of hydrogen peroxide (2%–2.5%) were ineffective in whitening the specimens, even when the manufacturers’ recommendations were followed. Thus, none of the groups tested significantly differed from each other, including their comparison with the artificial saliva (negative control) group.
Surface microhardness (Knoop hardness number)
The SMH values are given in Table 3 considering the interaction (p = 0.0007) between group and time (p < 0.0001). At T1, all the groups were allocated with similar values at the beginning of the treatment.
Table 3
Microhardness (Knoop hardness number) as a function of group and time and pH of groups
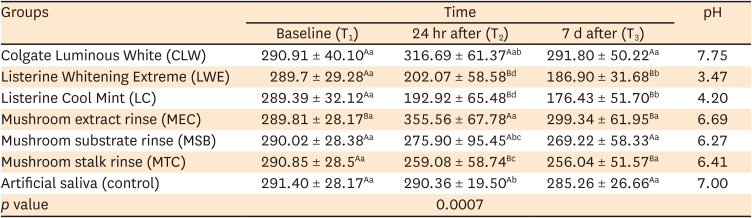
Values are presented as mean ± standard deviation or mean (pH).
Generalized linear models considering the group effects in T1 (before treatment), T2 (24 hours after the mouth rinse application), and T3 (7 days after the mouth rinse application).
Distinct letters (upper case horizontally and lower case vertically) indicate statistically significant differences within the group treatment over time (T1, T2, and T3) (p ≤ 0.05).
After 24 hours of mouth rinse application (T2), LWE, LC, and mushroom stalk rinse (MTC) groups showed a significant decrease in KHN compared to their initial values and similarity between themselves (p = 0.0007). The MEC group showed the highest KHN values compared to the other groups; and similarities with CLW. Moreover, the LWE and LC groups had the lowest values of microhardness when compared to the other groups (p = 0.0007). CLW group maintained its SMH at all times. LWE, LC, MSB, and MTC showed decreased microhardness after 14 days of mouth rinse application (p = 0.0007).
At T3 (7 days after the application), LWE and LC groups showed lower microhardness compared to T1 and T2. However, MSB did not differ from the artificial saliva group (p < 0.0001).
Measurement of pH
The mean pH values are shown in Table 3. The CLW group had an alkaline pH, higher than the pH of the artificial saliva solution, which was neutral (pH = 7). Meanwhile, LWE and LC had acidic pH values. The experimental mouth rinses MEC, MSB, and MTC had pH values closer to neutrality, similar to the artificial saliva.
Scanning electron microscopy
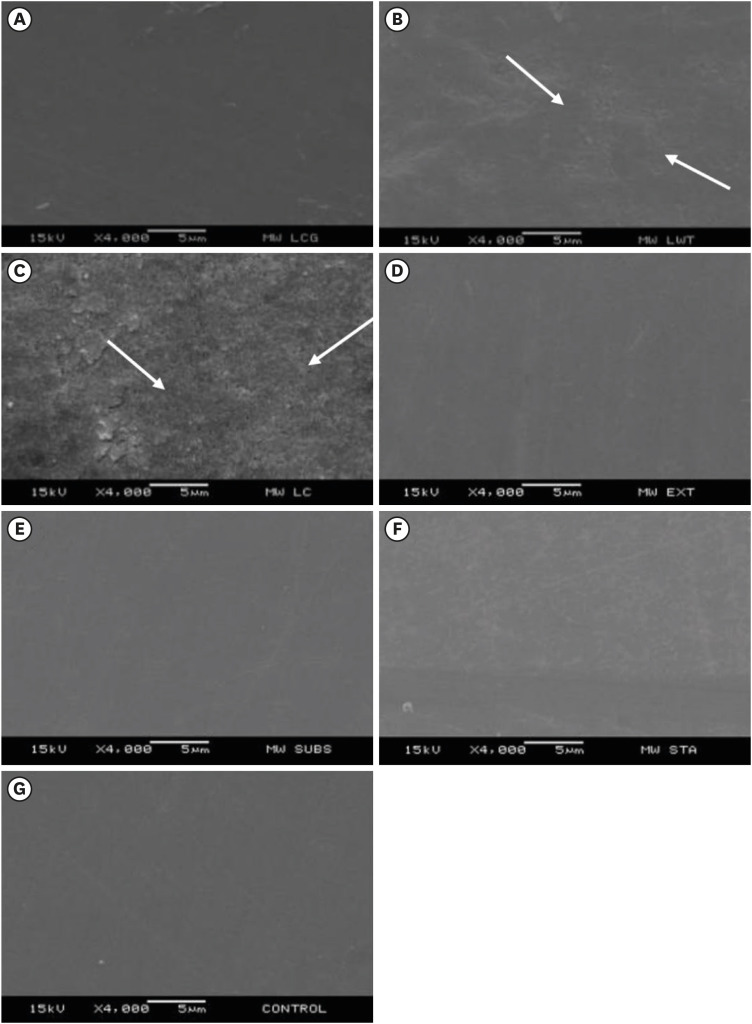
The SEM images of the enamel surface are presented in Figure 2. The enamel treated with CLW for 14 days (Figure 2A) showed surface irregularities. The groups treated with LWE (Figure 2B) and LC (Figure 2C) showed pores and surface irregularities with intermittent depressions in all analyzed samples. The arrows indicate the most irregular locations on the samples after 14 days of treatment with commercial rinses. The experimental groups MEC (Figure 2D), MSB (Figure 2E), and MTC (Figure 2F) showed no mineral loss or surface irregularities, resembling the control group (Figure 2G) that was stored for 14 days in artificial saliva with daily replacement.
Figure 2
Representative scanning electron microscopy images ×4,000, 5 μm. Arrows point to irregularities or pores on enamel surface after mouth rinse treatment. (A) 2% hydrogen peroxide, pyrophosphates and 225 ppm sodium fluoride (Colgate Luminous White). (B) 1.5% hydrogen peroxide, Listerine Whitening Extreme. (C) Alcohol/ethyl alcohol, Eucalyptol-Listerine Cool Mint (LC). (D) Mushroom extract rinse. (E) Mushroom substrate rinse. (F) Mushroom stalk rinse. (G) Artificial saliva, 14 days storage (control).
DISCUSSION
Historically, the whitening efficacy of mouth rinses has been little discussed; there are conflicting reports of their effects in the literature [1011]. However, few of these reports describe OTC products containing natural extracts [202526]. In this study, the effect of commercial whitening rinses was compared with experimental mushroom residue-based rinses (Table 1). The first null hypothesis tested was rejected because there was a significant difference in the ΔE* between the groups studied. The LWE and MSB groups differed from the artificial saliva group at T3.
The CIE standardizes the 3D L*a*b* color scale used in aesthetic research in dentistry. The system has 3 coordinates: L* refers to the luminosity value from 0 (black) to 100 (white), a* corresponds to the red (+a) or green (−a) values, and b* indicates the yellow (+b) or blue (−b) variation [25]. In this study, analysis was performed with these coordinates according to the parameters of ΔE*, ΔE00, and ΔWID. The LWE and MSB groups showed a color alteration for ΔE*. When determining whether tooth whitening was visible to the human eye, the ΔE00 was used (Table 2), and, in this study, no group differed significantly from the control group. Thus, mouth rinses with low concentrations of hydrogen peroxide (1.5%–2%) were ineffective in whitening the specimens, even when the manufacturers’ recommendations were followed.
According to Pérez et al. [27] the acceptability values of the whiteness level of all the experimental mushroom rinses were all below the reference values ΔWID = 2.90. However, the commercial rinses LWE, LC, and MSB reduced enamel microhardness, and MEC showed the highest microhardness 24 hours after treatment, suggesting that these treatments may be ineffective in terms of whitening teeth, but may result in desirable side effects, such as no change in enamel microhardness. Although MEC did not result in significant whitening activity, further studies with a similar formulation should be encouraged, as its numerical increase in WID may become significant in other specific circumstances (e.g. higher mushroom concentration), while also avoiding the unwanted side effects of conventional rinses or as auxiliary products during tooth whitening treatment.
Vieira et al. [11] have reported that using bleaching mouth rinses did not promote color change, in agreement with this study. Torres et al. [28], Oliveira et al. [29], and Karadas and Duymus [30] have reported that mouth rinses containing hydrogen peroxide were capable of promoting enamel whitening. According to the coordinates of CIELAB (ΔL*, Δa*, and Δb*); the LWE group tested in that study also showed variation in ΔE*. However, there are no reports regarding the parameters ΔE00 and ΔWID, specifically whether there is a noticeable difference in the human eye in the whiteness level after using whitening rinses.
The contact time in each protocol studied is an important factor for tooth whitening results. In Oliveira et al. [29], the specimens were subjected to 12 weeks of treatment with Listerine Whitening mouth rinse, which had a whitening effect on the ΔE*. However, Nahsan et al. [31] evaluated whitening rinses and showed that the whitening mouth rinses did not improve the color after 14 and 30 days of daily use. The 14-day period may have influenced the study, as no significant difference in the whiteness index (ΔWID) was observed in any of the groups studied. More recently, the WID has been developed to more accurately quantify the whiteness achieved by tooth whitening products [2]. OTC products are known to contain low concentrations of peroxides because they are used without professional supervision, and high concentrations of peroxides can cause injury to the oral mucosa [25].
The level of whiteness achieved by a bleaching technique depends on the exposure time and concentration of the active ingredient [1]. In Jaime et al. [32], the bleaching rinses tested in vitro were less effective than the house carbamide peroxide gel but had intermediate values compared to those of the artificial saliva group. This result may relate to the removal of extrinsic pigments, as it showed a different brightening capacity than on unstained enamel. However, Torres et al. [28] showed similar results for 10% carbamide peroxide used for 14 days compared to bleaching rinses used for 12 weeks. Several methods of color evaluation used in in vitro studies contribute to the divergence in results on the whitening efficacy of OTC products [31].
The second null hypothesis was also rejected because changes in the SMH of the dental enamel were detected. LWE and LC treatments resulted in lower surface enamel microhardness after 7 days of treatment, even with stabilization in artificial saliva.
Regarding the results of the physical properties of this study, the enamel microhardness decreased in the groups treated with LWE, LC, MSB, and MTC. The commercial groups LWE and LC also had an acidic pH (Table 3). This contributed to the enamel surface alteration because these solutions were acidic, and the absence of remineralizing agents and the presence of an alcoholic vehicle promoted greater alteration of the dental enamel surface [11]. CLW was more alkaline, and its microhardness was maintained after 24 hours and 7 days of treatment.
In addition, the surface topography did not differ from the untreated group due to the presence of agents such as pyrophosphate and sodium fluoride that have a high affinity with hydroxyapatite and contribute to enamel remineralization.
The experimental rinses containing mushroom residues (MEC, MSB, and MTC) showed a pH closer to neutral, and their enamel surface morphology did not differ from the untreated group. However, the microhardness of the MTC sample was reduced at the end of the treatment. The MEC group, in contrast, increased its microhardness 24 hours after the end of the rinsing protocol (Table 3). The MEC may have greater affinity through the enzymes in contains and promoted increased dental enamel microhardness. Using products based on natural extracts may be a good alternative to commercially available OTC products because they do not alter the physical properties of the enamel [15]. They also do not cause symptoms such as irritation of the oral mucosa and sensitivity [5].
Pauli et al. [17] have reported in a literature review that the use of biotechnologies with enzymes from mushroom residues in dentistry can interact with the tanases responsible for the extrinsic pigmentation of the tooth and promote the removal or control of stains. The enzyme tannase, also known as tannyl acyl hydrolase, is a hydrolytic enzyme, capable of promoting hydrolysis in ester or depsidic bonds in phenolic substrates, such as tannic acid, methyl gallate, ethyl gallate, propyl gallate and isoamyl gallate, and is promising in bleaching [19]. Another type of enzyme is peroxidases, a group of oxidoreductases that use peroxide as an electron acceptor instead of oxygen [19]. A recent study describing the action of peroxidases demonstrated that horseradish activation of high-concentration whitening gel accelerates the degradation of hydrogen peroxide, which could reduce adverse effects [26]. A limiting factor in our study was the use of enzymes not associated with hydrogen peroxide, which is the main component of tooth whitening.
The available literature suggests the use of natural agents in association with peroxide as an alternative to improve tooth whitening [20]. However, an increasing number of studies evaluating the action of products based on natural extracts show a trend in developing peroxide-free bleaching agents [15].
This study was designed to formulate natural whitening rinses with similar or better effects than commercially available OTC products because commercial rinses contain peroxides or alcohol and need to be extensively investigated, especially regarding the safety of these products. According to Consolaro [14], peroxide products are acidic and can make dental tissue more porous with uninterrupted use, since they are freely accessible. They can cause damage to soft tissue due to the caustic effect. It is therefore a good alternative to develop natural and edible products that do not cause any damage to oral health.
Thus, using sustainable and edible biotechnology in the oral cavity was investigated. In this study, the low concentration of mushroom residues used in the mouth rinses may have failed to enhance enamel whiteness. An important finding was that none of the experimental rinses affected the enamel surface morphology (Figure 2), and the application of MEC, increased enamel microhardness. Further research using natural extracts with higher concentrations and longer periods of time needs to be conducted to evaluate the performance of these formulations to determine if increased exposure to dental enamel has a possible whitening effect.
Another limiting factor in our study was the fact that the samples were not exposed to a longer exposure time with hydrogen peroxide and without in the formulations. However, the clinical use of a rinse does not exceed 2 minutes in the mouth, nor would the patient be able to prolong this time in the mouth. The study of enzymes in black mushrooms is still a little explored topic in the literature and deserves further studies to analyze the power of their enzymes in terms of dental surface benefits.
CONCLUSIONS
Considering the findings of this study, it can be concluded that none of the commercial mouth rinses nor the mushroom based rinses showed a significant whitening activity perceived by the human eye (ΔE00) and whiteness index (ΔWID) after the end of treatment and 7 days after of treatment. However, mouth rinses with mushroom extract showed the highest SMH 24 hours after treatment, suggesting that the use of a mouth rinse with mushroom extract may result in desirable effects on the microhardness of tooth enamel. The clinical relevance would be to use such products in conjunction with whitening therapy, since it has been proven that tooth structure does not recover immediately with saliva alone, so such material could recover mineral loss.
 XML Download
XML Download