

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endodontically treated teeth are more prone to fractures compared to vital teeth [1]. This increased vulnerability can be attributed to factors such as dentin dehydration resulting from the loss of pulp vitality and structural damage during the removal of carious tissue, access surgery, root canal preparation, and the use of irrigants and intracanal dressing during treatment and also retreatment systems [23]. The long-term outlook for endodontically treated teeth depends not only on the quality of the endodontic treatment but also on the choice of restorative technique employed [4]. Depending on the degree of tooth substrate loss, both direct and indirect techniques can be used for restoring endodontically treated teeth. Direct techniques, which involve resin composite restorations, offer advantages such as shorter treatment duration and the possibility of completing the procedure in a single visit, thus reducing costs for the patient [5]. However, it is important to note that the clinical outcomes of resin composite restorations can vary significantly, highlighting the importance of selecting the most appropriate restorative material [14].
To streamline the restorative process, materials designed for larger increments have been developed. Examples of such materials include bulk-fill resin composite restorations and single-fill bioactive composites [46789]. Among bioactive composites, a specific material known as alkasite stands out. Its composition includes inorganic glasses such as calcium fluorosilicate glass, Ba-Al silicate glass, and Ca-Ba-Al fluorosilicate glass [10]. Additionally, it contains non-reactive silanized particles called “IsoFillers,” which consist of pre-polymerized particles containing dimethacrylates [8]. The liquid component of this material comprises conventional monomers commonly found in resin composites. Importantly, it is devoid of acids or water and contains photopolymerizers and chemopolymerizers [11]. When the powder and liquid are mixed in a 1:1 ratio, they create a restorative material that releases fluoride and calcium ions [12].
This material exhibits a high remineralization capacity, attributed to the presence of alkaline charges (glass particles) in the powder. These particles can release acid-neutralizing ions when the pH of the oral cavity decreases [111314]. The dual polymerization reaction, involving both chemical and light curing processes, enables its use in a single increment for large restorations [1115]. The inclusion of IsoFiller in its composition helps alleviate the stress caused by polymerization shrinkage, making it feasible to use single increments even in extensive cavities [16].
Restorations using the alkasite restorative material have displayed lower microleakage rates compared to conventional resin composite and glass ionomer cement (GIC) [17]. Additionally, they exhibit good marginal sealing, especially when combined with adhesive application [1418]. Moreover, this material has demonstrated favorable mechanical performance, particularly when subjected to light curing, owing to the cross-polymerization reaction between the monomers [81214]. It also possesses excellent radiopacity and dimensional stability [1215].
Considering the advantageous properties of bioactive composite resins and the limited number of in vivo investigations, this study aimed to assess the clinical performance of an alkasite restorative material in endodontically treated mandibular molars. The null hypothesis tested was that treatment with alkasite restorative material has no impact on the clinical performance of restorations in root canal-treated molars after 7 days (baseline), 6 months, and 17 months.
MATERIALS AND METHODS
Experimental design
This study was conducted as a randomized clinical trial involving 33 patients (with a mean age of 38) who had previously undergone endodontic treatment on their first or second lower molars and required direct adhesive restoration on either the occlusal (Class I) or occlusal-proximal (Class II) surfaces. Seventeen teeth were restored with an alkasite restorative material (Cention N, Ivoclar Vivadent, Barueri, SP, Brazil - experimental group), while the remaining 16 teeth were restored with a bulk-fill resin composite (Tetric N Ceram Bulk Fill, Ivoclar Vivadent - control group). The response variables included clinical assessments (retention, secondary caries, and marginal adaptation) and photographic evaluations (restoration color, marginal pigmentation, and anatomical form). Radiographic examinations of the restorations (contact point, presence of radiolucent lines, and gaps or excess material) were also conducted.
Ethical aspects
The project received approval from the Research Ethics Committee (CAAE: 46526321.4.0000.5419) and was registered in the Brazilian Registry of Clinical Trials – ReBEC (RBR-97kx5jv). Patients were informed about the study’s objectives and voluntarily signed the Informed Consent Form to participate in the research. To maintain the participants’ confidentiality and anonymity, the authors replaced personal identifiers with consecutive numbers in the databases and meticulously organized the data in Excel tables.
Patient selection and randomization
The study commenced by selecting patients from the Dental Clinic System database who met specific inclusion criteria: having a lower molar that required direct restoration on occlusal and/or interproximal surfaces following root canal treatment, and possessing an opposing tooth. Teeth with significant loss, chronic or aggressive periodontitis, or endodontic treatment performed over 6 months ago were excluded.
Initially, 481 patients were identified in the Dental Clinic System, of which 60 met the criteria for restorative treatment, and 33 agreed to participate in the study. Clinical examinations and digital periapical radiographs (CDR Elite, Fona, São Paulo, SP, Brazil) were conducted to assess the status of the root canal treatments. Following a 7-day follow-up, it was observed that 3 patients did not attend the follow-up session, leading to the loss of 2 patients from the alkasite restorative material group and 1 patient from the bulk-fill resin composite group. As a result, a total of 30 patients were included in the statistical calculations, with 15 patients receiving the alkasite restorative material (Cention N, Ivoclar Vivadent), and another 15 patients receiving the bulk-fill resin composite (Tetric N Ceram Bulk Fill, Ivoclar Vivadent). During the subsequent 6 months of follow-up, no additional losses occurred, and all 30 patients were retained for the statistical analysis.
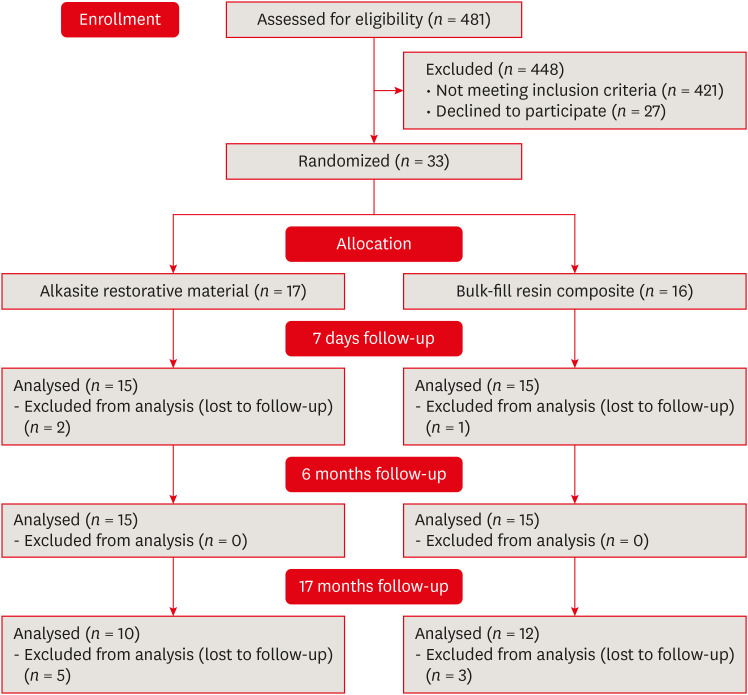
However, after a total of 17 months, it was discovered that 8 patients did not return for evaluation, with 5 losses observed in the alkasite restorative material group and 3 losses in the bulk-fill resin composite group. As a result, the final sample size for the statistical analysis consisted of 22 patients. Figure 1 depicts the CONSORT diagram, visually illustrating the distribution, allocation, follow-up, and analysis of the research subjects.
Figure 1
Consolidated Standards of Reporting Trials diagram, form of recruitment, allocation, follow-up and analysis of research subject.
The treatment randomization (experimental or control) was conducted using a computer spreadsheet available at http://randomnumbergenerator.intemodino.com/pt.
Restorative treatment
Prophylaxis was performed using a pumice paste (S.S. White, Rio de Janeiro, RJ, Brazil) and water, applied with a Robinson brush (Jon, São Paulo, SP, Brazil) at low rotation (Kavo, Joinville, SC, Brazil). Local anesthetic EMLA (AstraZeneca, Cotia, SP, Brazil) was administered to the buccal mucosa and gingival papilla.
The teeth were isolated with a rubber dam (Madeitex, São José dos Campos, SP, Brazil) and clamps of various sizes (Duflex, S.S. White), depending on the tooth’s morphology. Temporary restorations were removed using a high-speed handpiece (Kavo) and spherical burs (KG Sorensen, Cotia, SP, Brazil). A low-speed handpiece (Kavo) with spherical burs (KG Sorensen, Barueri, SP, Brazil) was utilized to refine and smooth the cavity walls.
The cavities were rinsed with a water spray and dried using air jets. The canal entrance was sealed with GIC (Ionoseal, DFL, Rio de Janeiro, RJ, Brazil). Matrices (Unimatrix, TDV, Pomerode, SC, Brazil) were placed for teeth that required restoration of the proximal surface.
Subsequently, the enamel was selectively etched with 37% phosphoric acid (Dentsply Sirona, Pirassununga, SP, Brazil) for 30 seconds. Afterward, the cavity was rinsed with water and dried using absorbent paper. A layer of universal adhesive (Tetric N-bond Universal, Ivoclar Vivadent) was applied to all surfaces of the cavity. This was accomplished with the aid of a disposable applicator (KGBrush, KG Sorensen), actively brushing the product for 20 seconds. Light air jets were then applied to ensure uniform coverage of the adhesive on both enamel and dentin surfaces. Finally, the material was light-cured (Grand Valo, Ultradent, Indaiatuba, SP, Brazil) for 10 seconds at 1,500 mW/cm2.
For cavities restored with bulk-fill resin composite (Tetric N-Ceram Bulk Fill, Ivoclar Vivadent), increments of up to a maximum of 4 mm were applied, measured with a periodontal probe, and resin spatulas were used to restore the tooth’s anatomy. Each increment up to 4 mm was then light-cured for 20 seconds. In proximal cavities, the resin composite in the buccal and lingual regions was polymerized for an additional 10 seconds after removing the matrix and wedge.
In the case of teeth restored with the alkasite restorative material (Cention N, Ivoclar Vivadent), the application followed the manufacturer’s recommendations. This process involved using one measuring spoon of powder to 1 drop of liquid, and in larger cavities, 2 or 3 spoons of powder were used for 2 or 3 drops of liquid, respectively. The powder and liquid were dispensed onto a glass plate in the specified proportions. The liquid was dripped onto the surface with the flask held perpendicular to it, and excess powder was removed by scraping the spoon against the plastic fin on the flask's mouthpiece. Subsequently, the powder was divided into 2 equal portions using a plastic spatula, and the liquid was spread across the plate to increase the surface area. With the same spatula, the first half of the powder was mixed into the liquid until a thoroughly blended consistency was achieved. The second half of the powder was then incorporated for 45 to 60 seconds until a homogeneous mixture was obtained. This material was applied and adapted to the cavity with a resin spatula and condenser, and occlusal excesses were removed. Due to the extent of the cavity, an additional 20-second light-curing (Grand Valo, Ultradent, South Jordan, UT, USA) was performed to complement the polymerization process.
After completing the restorations, the rubber dam was removed, and occlusal adjustments were performed using carbon paper (AccuFilm, Parkell, Farmingdale, NY, USA) and diamond finishing tips (KG Sorensen). Sandpaper strips (3M ESPE, Sumaré, SP, Brazil) and flexible abrasive discs (Sof-lex pop-on, 3M ESPE) were also employed during the finishing process. Patients returned after 7 days for the final polishing of the restorations using silica points (Enhance, Dentsply Indústria e Comércio Ltda, Petrópolis, RJ, Brazil) and polishing paste (Universal, Ivoclar Vivadent).
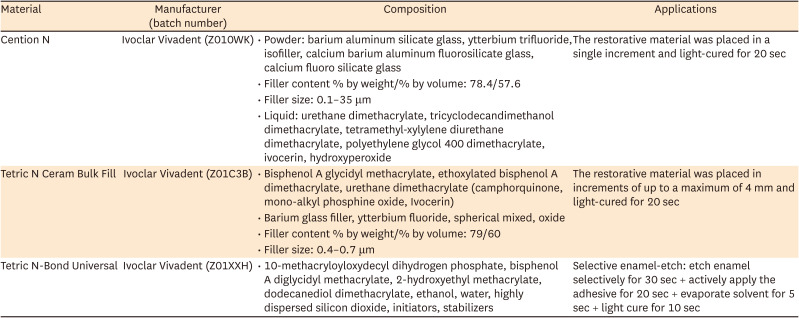
All restorative treatments for the patients included in this study were performed by the same operator. The materials used for restoration and relevant information about each material are described in Table 1.
Table 1
Presentation of the materials used for restoration in the study
Clinical, radiographic and photographic evaluations
The teeth underwent clinical, photographic, and radiographic evaluations at 3 time points: 7 days, 6 months, and 17 months after restoration.
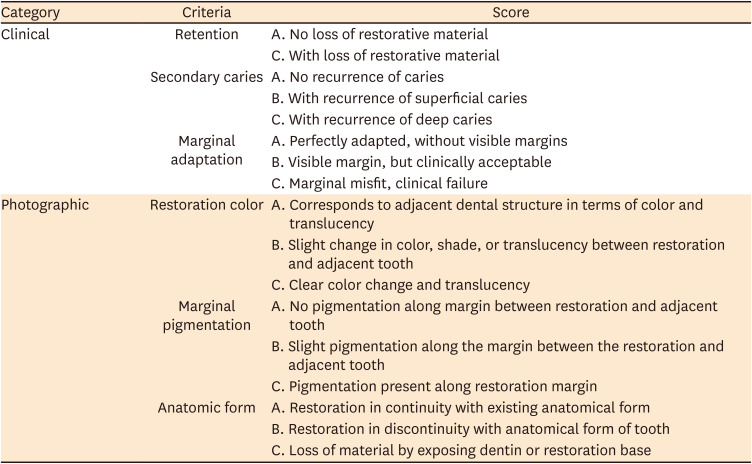
The clinical and photographic assessments of the restorations were performed by 3 trained and experienced examiners, following the modified United States Public Health Service criteria [19]. These criteria categorized the restorations into 3 classes: Alpha - indicating no issues with the evaluated criterion, and the restoration is in perfect condition; Bravo - denoting minor imperfections that are still clinically acceptable, and Charlie - representing significant flaws requiring restoration replacement. Detailed specific criteria can be found in Table 2.
Table 2
Modified United States Public Health Service criteria used to evaluate the restorations
Intraoral photographs were taken using a digital camera (Canon EOS Rebel T5i 18.0 Megapixels, Canon, Tokyo, Japan) and a mouth mirror for photography. These photographs captured the palatal surface of the restored teeth from mesial, distal, and palatal perspectives, resulting in a total of 3 images. A blind and simultaneous assessment of the photographs was conducted by viewing the images on a notebook screen in a controlled environment with uniform lighting.
Interproximal radiographs were taken using a digital radiography sensor (CDR Elite, Fona), with a specialized positioner designed for this technique. The patient was positioned at a 90° angle with their head in a neutral position for the radiographs, and they wore a protective apron and a lead thyroid shield. The X-ray machine head was positioned with a 10° vertical angulation. Multiple radiographs with interproximal overlays were captured.
The radiographic evaluation was performed by 3 examiners in a blinded and simultaneous manner. They viewed the images on a notebook screen in a controlled environment with consistent lighting. The assessment followed specific criteria, which included the analysis of the radiographic adaptation of the restoration. This analysis considered the presence or absence of a radiolucent line at the tooth-restoration interface, the presence or absence of excess or insufficient restorative material, the adequacy of the contact point, and the presence of caries recurrence. A restoration was considered radiographically adequate when it displayed proper adaptation (no radiolucent line at the tooth-restoration interface, absence of excess or insufficient restorative material, and a satisfactory contact point) and was free from caries recurrence [20].
Data analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences software (SPSS version 25.0, IBM, Chicago, IL, USA) at a significance level of 5%. The data analysis was non-parametric. The Mann-Whitney test was applied to compare the 2 groups concerning the independent variable of material comparison. The Friedman test was employed to analyze the dependent variable across different time periods (baseline, 6 months, and 17 months). The Cohen Kappa test was utilized to assess intra- and inter-examiner agreements.
RESULTS
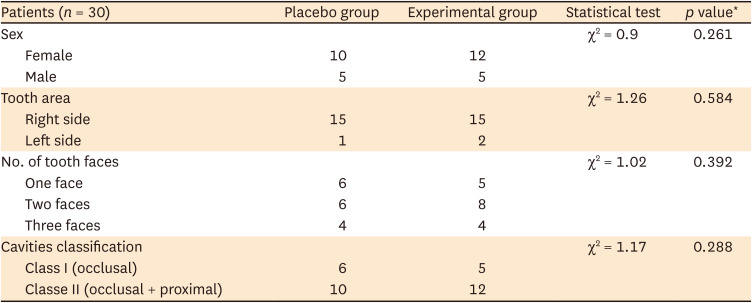
The study encompassed 33 patients, consisting of 13 males and 20 females, with ages spanning from 18 to 58 years and an average age of 38. The restored teeth (n = 33) were comparably positioned in the dental arches, and there was a similarity in the number of tooth faces involved and the type of cavity for both groups (p > 0.05) (Table 3).
Table 3
Demographic aspects of patients
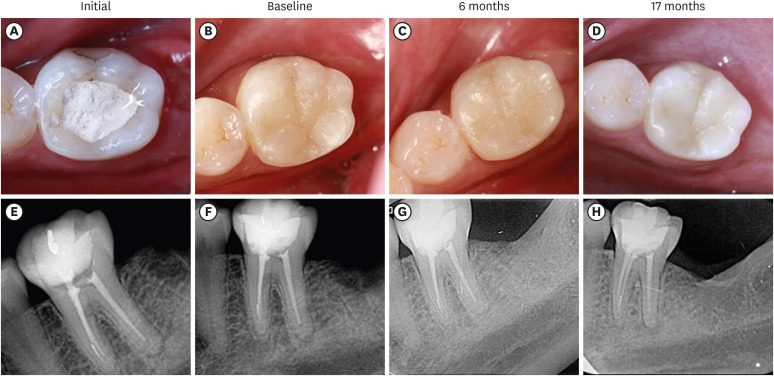
Alkasite restorative material was applied in 17 restorations (Figure 2), while bulk-fill resin composite was utilized in 16 restorations (Figure 3). Three patients did not return for clinical evaluations; 1 had a restoration using bulk-fill resin composite, and 2 had received alkasite restorative material.
Figure 2
Restorations made with alkasite restorative material (Cention N, Ivoclar). The figures illustrate teeth at: (A) Initial condition; (B) Baseline (after polishing); (C) 6 months after restoration; (D) 17 months after the restoration; (E) Initial radiography; (F) Baseline radiography; (G) 6 months radiography; (H) 17 months radiography.
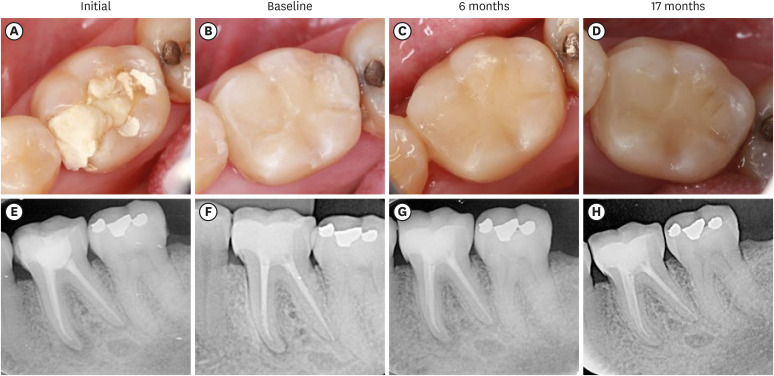
Figure 3
Restorations made with bulk-fill resin composite (Tetric N Ceram Bulk Fill, Ivoclar). The figures illustrate teeth at: (A) Initial condition; (B) Baseline (after polishing); (C) 6 months after restoration; (D) 17 months after the restoration; (E) Initial radiography; (F) Baseline radiography; (G) 6 months radiography; (H) 17 months radiography.
The intra-examiner Kappa index was 1.0 for each examiner (A to A, B to B, and C to C). The inter-examiner index was 0.95 between A and B, 0.87 between A and C, and 0.98 between B and C.
Regarding the clinical criteria, for the retention factor, there was an 83% alpha score observed after 17 months in teeth restored with bulk-fill resin composite (n = 12) and a 90% alpha score with alkasite restorative material (n = 10). No significant difference was found between the 2 materials (p = 0.6933) or among the time periods (baseline, 6 months, and 17 months) (p = 0.0696). Marginal adaptation did not significantly differ between both materials (p = 0.693), but a notable difference was identified across different time periods (baseline, 6 months, and 17 months) (p = 0.00002). After 17 months, an 83% alpha score was observed with bulk-fill resin composite (n = 12), and an 80% alpha score was obtained with alkasite restorative material (n = 10). For secondary caries, both groups displayed a 100% alpha score.
For the photographic criteria analysis, a 75% alpha score was achieved after 17 months in teeth restored with bulk-fill resin composite (n = 12), whereas a 10% alpha score was observed in those restored with alkasite restorative material (n = 10) concerning color analysis. A significant difference emerged between the 2 materials (p = 0.0000), but no distinction was noted across different time periods (p = 0.4071). Since the baseline analysis, the restorations using alkasite restorative material showed a slight variation in color compared to adjacent teeth.
A noteworthy difference was observed in anatomical form (p = 0.0189), recording a 63% alpha score after 17 months for bulk-fill resin composite (n = 12) and a 20% alpha score for alkasite restorative material (n = 10). Restorations made with alkasite restorative material displayed minor wear over 17 months (p = 0.0006), affecting the anatomical form.
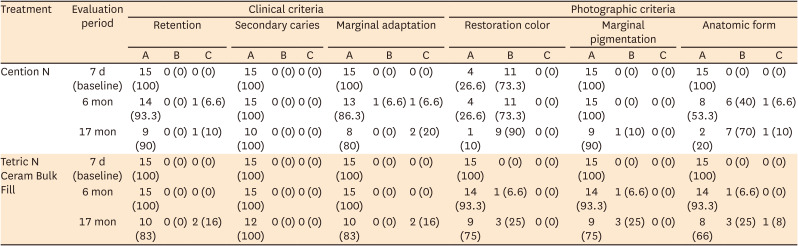
The difference between materials for marginal pigmentation was not significant (p = 0.587). After 17 months, a 75% alpha score was achieved for teeth restored with bulk-fill resin composite (n = 12), and a 90% alpha score was obtained with alkasite restorative material (n = 10). Both materials demonstrated success in the radiographic criteria. Table 4 presents the clinical and photographic analysis of the restorations.
Table 4
Clinical and photographic analysis of the restorations using the modified United States Public Health Service criteria
DISCUSSION
The alkasite restorative material consists of reactive glass particles that release ions and non-reactive silanized particles, which have shown bioactivity when combined with calcium fluoro-silicate glass in its composition [212223]. The initial analysis did not find a significant difference in restoring endodontically treated teeth with nanohybrid resin composite and alkasite [24]. Clinical assessments over a 2-year period also indicate acceptable clinical outcomes in Class I and II restorations restored with alkasite restorative material [25].
The null hypothesis was accepted for criteria such as retention, secondary caries, and marginal pigmentation. However, it was rejected concerning anatomical form and marginal adaptation criteria. Studies involving the alkasite restorative material reported sustained preservation of anatomical shape, indicating good retention, anatomical form, marginal adaptation, control of cariogenic activity, and reduced discoloration for 9 and 12 months [926]. Nevertheless, the clinical analysis in the current study revealed a change in scores for some evaluated criteria over time.
The group using alkasite restorative material displayed anatomical wear in the restoration after 17 months, shifting from Alpha to Bravo indexes, whereas the control group utilizing bulk-fill resin composite showed no changes. Previous clinical studies also observed anatomical shape alterations after 12 months with alkasite, albeit to a lesser extent than seen in this study [27]. Discrepancies in results might be attributed to variations in restoration size, cavity type, patient age, and the available sample size for analysis.
Changes in scores for the marginal adaptation criterion were noted over the months, but no differences were observed between the materials used, aligning with findings from the study by Oz et al. [28], where both groups (alkasite or composite resin) displayed significant changes in marginal adaptation after 12 months. However, in a 2-year evaluation, restorations with alkasite restorative material exhibited a more pronounced decrease in marginal integrity compared to the resin composite. The authors suggested that the technical intricacy and manual mixing of this material might have led to a greater reduction in marginal integrity compared to the composite resin restorations [25].
The criterion for color restoration was impacted by the choice of material. Initially, restorations made with Cention N composite received a Bravo rating due to its limited color range, confined to A2. While A2 is generally suitable for most cases, it may still present slight discrepancies when compared to adjacent teeth. Conversely, Tetric N Ceram Bulk Fill resin composite offers a significantly wider array of colors, allowing for better blending between the restorative material and natural teeth. This clinical study did not observe significant differences in the darkening of restorations. However, another clinical study reported slight darkening after 6 months during a 9-month follow-up on Class II restorations in deciduous molars [26]. Cention N showed potential for color alteration when exposed to solutions like Tea, Coffee, and Coke [29]. The dietary habits of the patients in our study might have influenced the variation in results concerning the darkening of the restorations.
Both materials demonstrated success in preventing secondary caries. This aligns with clinical reports showing a 100% success rate in preventing cavity recurrence after 24 months using conventional bulk-fill composite resin and alkasite restorative material [25]. Studies comparing alkasite with GIC also revealed the absence of secondary caries lesions after 9 months and 12 months [926]. The inclusion of alkasite in the experimental group was expected to improve success in this criterion by releasing ions that promote dental structure bioremineralization. Its high fluoride release capacity, ion rechargeability, and satisfactory marginal adaptation in extensive cavities make it an excellent choice for high-risk cavity patients [103031].
The utilization of an adhesive system in conjunction with both restorative treatments likely contributed to the sustained retention, yielding high success rates even after the 17-month evaluation. The adhesive system utilized encompasses the 10-methacryloyloxydecyl dihydrogen phosphate monomer, known for its capacity to generate stable calcium salts that shield collagen fibers from degradation. It helps maintain a balance between hydrophilic and hydrophobic domains, ensuring adequate substrate wetting and copolymerization ability [17]. Meshram et al. [18] observed reduced microleakage in restorations using Cention N when coupled with the adhesive system, emphasizing how bonding agents aided in achieving a tight seal between the restorative material and the tooth interface.
The utilization of bioactive composite in endodontically treated teeth offers an enticing option due to its ability to release ions, thereby strengthening the tooth, alongside its high monomeric conversion and dimensional stability [1531]. While the clinical performance of bioactive composite has yet to demonstrate superiority over bulk-fill resin composite restorations, the insights gleaned from this study provide valuable information across various criteria evaluated over a 17-month period. Further exploration of this restorative approach is warranted to attain a comprehensive understanding and potential refinements. Despite being a pilot study with a sample size considered small compared to other clinical studies, the assessment of the feasibility and suitability of the research protocol beforehand enables researchers to tackle methodological challenges, refine data collection procedures, and accurately estimate sample size parameters for future studies. This proactive approach bolsters the robustness of subsequent investigations and contributes to the advancement of knowledge in the field of restorative dentistry.
CONCLUSIONS
Despite the limitations of this clinical study, the 17-month evaluation indicates that the use of alkasite restorative material (Cention N) is a viable option for the restoration of endodontically treated teeth; however, long-term assessment of the clinical application of these bioactive composites is important.
 XML Download
XML Download