

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The femoropopliteal artery is the most commonly affected vessel in patients with peripheral artery disease undergoing endovascular treatment (EVT).1) However, EVT using conventional uncoated balloons and bare metal stents (BMS) is associated with relatively high rates of restenosis, especially in complex femoropopliteal lesions. Various forces generated by leg movement, such as axial and radial compression, bending, and torsion, can affect post-EVT outcomes.2)3) To reduce restenosis after EVT for femoropopliteal disease, paclitaxel-based drug-eluting stents (DES) and drug-coated balloons were developed and introduced for clinical use.4)5) Zilver PTX™ (Cook Medical, Bloomington, IN, USA), a polymer-free paclitaxel-coated nitinol DES, was the first DES demonstrating superior primary patency, compared to conventional balloon angioplasty or BMS, in a randomized controlled trial.5)6) Despite favorable outcomes reported in several registry studies, the effectiveness of Zilver PTX™ in real-world settings remains inconsistent.7)8)9)10)
The Eluvia™ (Boston Scientific, Marlborough, MA, USA) DES is a recently introduced and was designed to release paclitaxel over 6 months, facilitated by a biocompatible fluoropolymer coating. In the IMPERIAL study (a randomized controlled trial), Eluvia for femoropopliteal artery lesions demonstrated non-inferiority to Zilver PTX for both efficacy and safety at 12 months, as well as superiority over Zilver PTX for primary patency in a post-hoc analysis.11) However, the lesions included in the IMPERIAL study were relatively short, with a mean length of approximately 8 cm. According to a Korean registry study, more than 50% of femoropopliteal lesions were classified as Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) type C or D.1) Whether Eluvia is still able to achieve favorable clinical outcomes in complex femoropopliteal lesions during real-world practice remains uncertain. Thus, the objective of the present study (called K-ELUVIA) was to investigate the clinical efficacy and safety of the Eluvia stent for femoropopliteal artery disease using data from a prospective multicenter registry.
METHODS
Ethical statement
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki (2013) and was approved by the Institutional Review Board (IRB) at each participating center (Severance Hospital IRB number: 1-2015-0075). It was registered at www.clinicaltrials.gov (NCT03505931). All patients provided written informed consent before enrollment.
Study population and enrollment
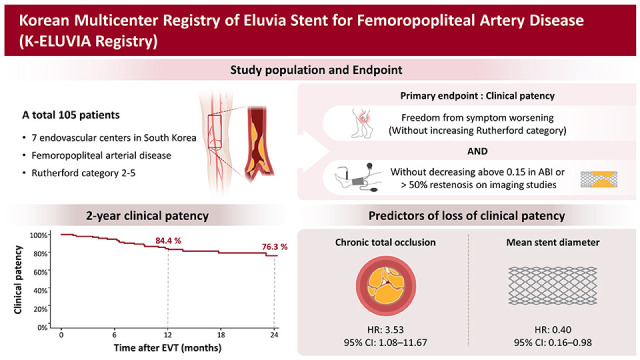
The K-ELUVIA was designed as a single-arm, prospective, multicenter trial to assess the efficacy and safety of Eluvia stents for the treatment of femoropopliteal artery disease. The study was conducted at 7 endovascular centers in South Korea. Patients were eligible for participation if all of the following criteria were met: age ≥19 years, Rutherford category 2 to 5, stenotic (≥50% diameter stenosis) or occlusive femoropopliteal artery lesions, and an ankle-brachial index (ABI) <0.9. The exclusion criteria were age >85 years; acute severe limb ischemia or severe chronic limb-threatening ischemia (CLTI; Rutherford category 6); in-stent restenosis of a previously implanted stent; lesion previously treated with a bypass graft; untreated proximal inflow disease of the ipsilateral iliac artery (>50% stenosis or occlusion); uncontrolled congestive heart failure or left ventricular ejection fraction ≤40%; severe hepatic dysfunction (aspartate aminotransferase or alanine aminotransferase ≥3-fold higher than the upper limit of normal); significant leukopenia, neutropenia, thrombocytopenia, anemia, or risk of bleeding; pregnant or fertile female; life expectancy <1 year; or known allergic reaction to heparin, aspirin, clopidogrel, or contrast agent. The following was obtained for each patient prior to study enrollment: medical history, baseline medications, Rutherford classification, ABI, the results of ≥1 lower extremity imaging study (e.g., computed tomography [CT], magnetic resonance imaging, duplex ultrasonography, catheter angiography), TASC II type, and standard laboratory test results.
Endovascular treatment
Loading doses of aspirin 300 mg and clopidogrel 300 mg were administered ≥12 hours before EVT to all patients who were not receiving aspirin and clopidogrel for ≥5 days prior to the procedure. During EVT, all patients received local anesthesia, which was supplemented with intravenous sedation and analgesia, as needed. After insertion of the introducer sheath, unfractionated heparin 5,000 U was administered intravenously, and the activated coagulation time was maintained above 250 seconds with additional doses of heparin, if required. Vascular access was achieved percutaneously using either the ipsilateral antegrade approach or the contralateral cross-over approach from the common femoral artery. A 6 or 7-Fr. TERUMO Inc. sheath (TERUMO Inc., Tokyo, Japan) was employed for the ipsilateral approach, and a 6 or 7-Fr. Balkin or Ansel sheath (Cook Inc., Bloomington, IN, USA) was used for the contralateral approach. A 0.018 or 0.035-inch guidewire was used to cross the target lesion. When occlusion was complete, either an intraluminal or subintimal approach was used for revascularization, at the operator’s discretion. After successful passage of the guidewire, target lesions were routinely predilated using a balloon with a diameter equal to or smaller than the reference diameter. Thereafter, Eluvia stent(s) were implanted to cover the target lesion. The stent diameter was selected based on the target lesion reference diameter. Post-stent dilation was performed when the residual stenosis was >30%. After EVT, dual antiplatelet therapy (aspirin 100 mg/day and clopidogrel 75 mg/day) was recommended for ≥6 months, after which single antiplatelet therapy with aspirin or clopidogrel was used.
Follow-up
Following EVT, patients underwent regular assessment of symptoms based on Rutherford classification at 1 month after the procedure and then every 6 months for 2 years. ABI measurements were obtained at 6, 12, and 24 months post-procedure or whenever deterioration in symptom status was observed. Imaging evaluation (e.g., duplex ultrasonography, CT angiography, invasive arteriography) was recommended at 12 months post-EVT or whenever symptoms worsened by ≥1 Rutherford category or ABI decreased by >0.15.
Endpoints and definitions
The primary study endpoint was initially defined as 12-month primary patency, determined by imaging studies such Duplex ultrasound, CT angiography, or catheter angiography. However, due to the challenges posed by the coronavirus disease 2019 (COVID-19) pandemic and patient apprehension regarding attendance for required imaging studies, the primary endpoint was modified to best reflect the clinical status of the trial subjects. Consequently, the primary endpoint was revised to 2-year clinical patency. This was defined as freedom from symptom worsening, indicated by an increase in Rutherford category accompanied by a ≥0.15 decrease in ABI or >50% restenosis on imaging studies. A lesion or adjacent-segment peak systolic velocity ratio >2.4, as measured by duplex ultrasonography, was considered indicative of >50% restenosis. The secondary study endpoint was the 2-year freedom from clinically driven target lesion revascularization (TLR), defined as any repeat intervention or surgical treatment for restenotic lesions characterized by both worsening symptoms and a ≥0.15 decrease in ABI. Procedural success was defined as <30% residual stenosis plus no evidence of arterial dissection causing flow limitation. Angiography findings were used to categorize arterial calcification severity according to the Peripheral Arterial Calcium Scoring System (PACSS)12): grade 1, mild calcification; grade 2 or 3, moderate calcification; and grade 4, severe calcification.
Statistical analysis
Continuous variables are presented as mean ± standard deviation, and categorical variables are shown as frequency and percentage. Baseline clinical and lesion characteristics were analyzed using the Student’s t-test for continuous data and the χ2 and Fisher’s exact test for categorical data. Primary and secondary endpoints were assessed using Kaplan-Meier survival analysis, with the log-rank test used to compare groups, as appropriate. Predictors of loss of clinical patency were evaluated using Cox proportional hazard regression analyses. Sex, body mass index, age, and variables with a p value <0.2 in univariable Cox regression analysis were included in the multivariable Cox regression model. The p values <0.05 were considered statistically significant. All statistical analyses were performed using SPSS 25.0 software (IBM Corp., Armonk, NY, USA) and R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Study population and baseline characteristics
A total of 105 patients were enrolled in the K-ELUIVA study from May 2018 to March 2021. One patient was excluded because inclusion criteria were not met, with the remaining 104 patients included in the final analysis (Figure 1). Baseline patient characteristics are summarized in Table 1. The mean patient age was 68.2±10.4 years, and the majority of patients (82.7%) were male. Hypertension and diabetes were present in 64.4% and 67.3% of patients, respectively. Chronic kidney disease was present in 19.2% of patients, and 11.5% of all patients required hemodialysis for end-stage renal disease (ESRD). The most frequent clinical presentation of femoropopliteal artery disease was severe claudication (Rutherford category 3, 48.5%; Figure 2). The pre-procedural mean ABI in the treated extremity was 0.6±0.2.
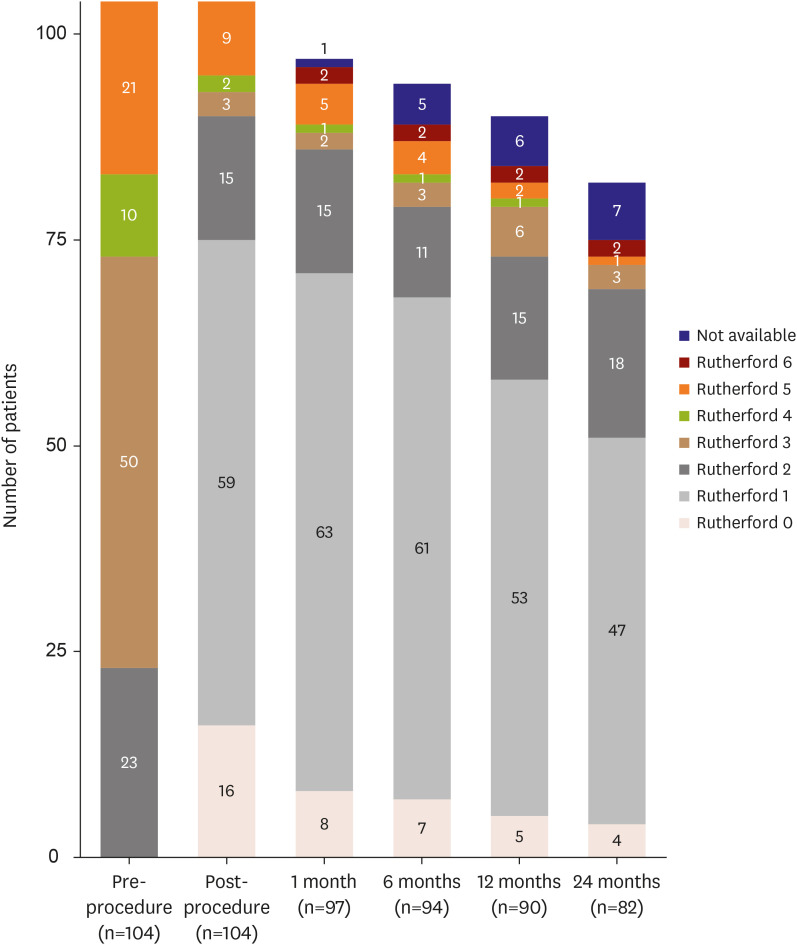
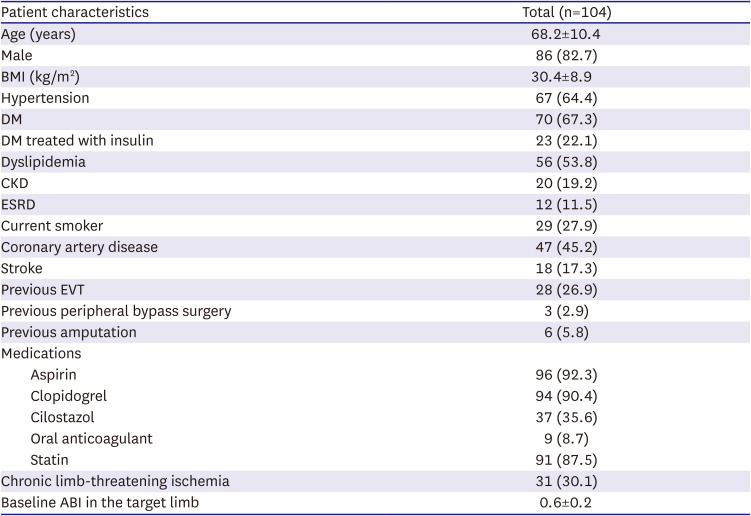
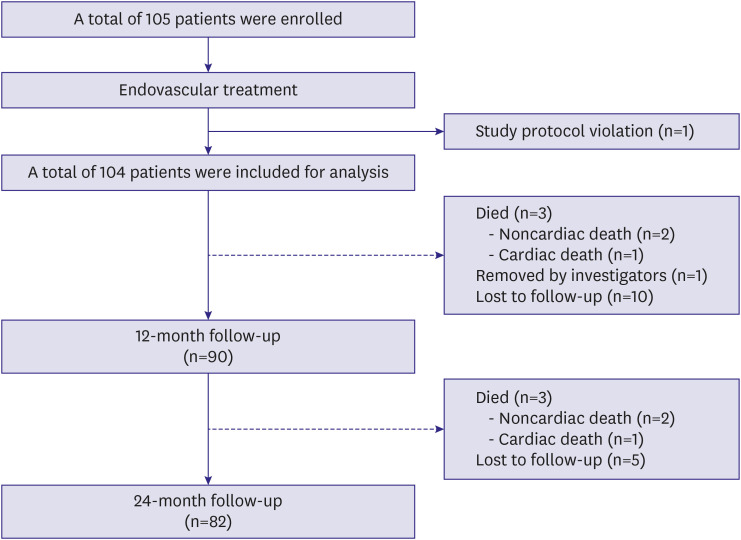
Figure 2
Distribution of Rutherford categories before endovascular treatment, after the procedure, and during follow-up.
![]()
Table 1
Baseline patient characteristics
Data are mean ± standard deviation or number (percentage).
ABI = ankle-brachial index; BMI = body mass index; CKD = chronic kidney disease; DM = diabetes mellitus; ESRD = end-stage renal disease; EVT = endovascular treatment.
![]()
Lesion characteristics and procedural data
Lesion and procedural characteristics are summarized in Table 2. The mean lesion length was 168.3±117.6 mm. A totally occluded lesion was treated in 57.7% of patients. Complex lesions (TASC II type C or D lesions) were present in 46.1% of patients, and 26.9% of patients had concurrent popliteal artery involvement. The procedural success rate was 99.0%. Only 1 patient had a suboptimal result, characterized by slow antegrade flow after stent implantation because of distal thrombus embolization.
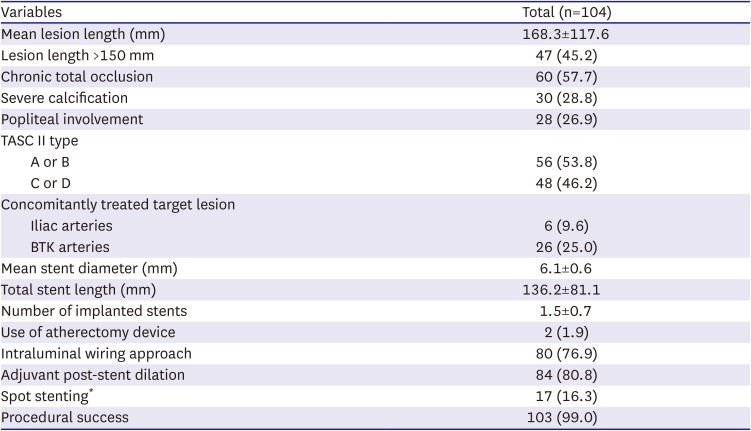
Table 2
Baseline lesion characteristics and procedural data
Data are mean ± standard deviation or number (percentage).
BTK = below the knee; TASC II = Trans-Atlantic Inter Society Consensus for the Management of Peripheral Arterial Disease.
*Total length of stents/length of lesion <0.5.
![]()
The intraluminal wiring approach was utilized in 76.9% of patients. Mean total stent length and diameter were 136.2±81.1 mm and 6.1±0.6 mm, respectively. Adjuvant post-stent dilation was performed in 80.8% of patients. One patient developed arterial rupture with nonfatal bleeding, which was successfully managed by implanting a covered stent. During hospitalization, 1 patient died because of sepsis secondary to an infected foot wound.
Clinical outcomes
The median duration of clinical follow-up was 530 days (interquartile range, 369–718 days). Of the 104 patients included in this study, 82 completed the 2-year follow-up. There were 6 mortalities (2 cardiovascular and 4 noncardiovascular deaths), and 15 patients were lost to follow-up. Two of participants required minor amputation due to the deterioration of foot wounds despite undergoing repeated EVT, but there were no cases of major amputation. Imaging studies were conducted in 42.3% of patients at 12 months. Patient symptom status improved from a median Rutherford category of 3 pre-procedure to 1 after EVT. This improvement was sustained for 24 months (Figure 2).
The primary outcome of clinical patency was 84.4% at 1 year after EVT and 76.3% at 2 years post-EVT (Figure 3A). The secondary outcome of freedom from clinically driven TLR was 89.1% at 1 year after EVT and 79.1% at 2 years post-EVT (Figure 3B). The clinical patency rate was higher in nonocclusive lesions than in chronic total occlusions (89.7% vs. 64.5%, p=0.023; Figure 4A). However, complex lesions (TASC II type C/D vs. type A/B; Figure 4B), long lesions (≥150 mm vs. <150 mm; Figure 4C), and severely calcified lesions (PACSS grade 4 vs. grade 0–3; Figure 4D) were not significantly associated with clinical patency during follow-up. In multivariable Cox regression analysis, chronic totally occluded lesions (hazard ratio [HR], 3.53; 95% confidence interval [CI], 1.08–11.67; p=0.039) and mean stent diameter (HR, 0.40; 95% CI, 0.16–0.98; p=0.044) were identified as independent predictors of loss of clinical patency at 2 years (Table 3).
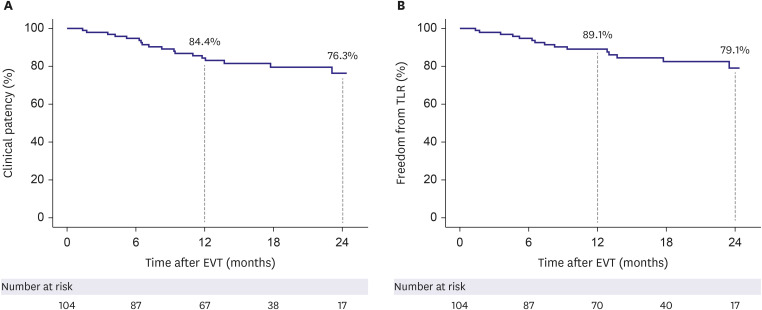
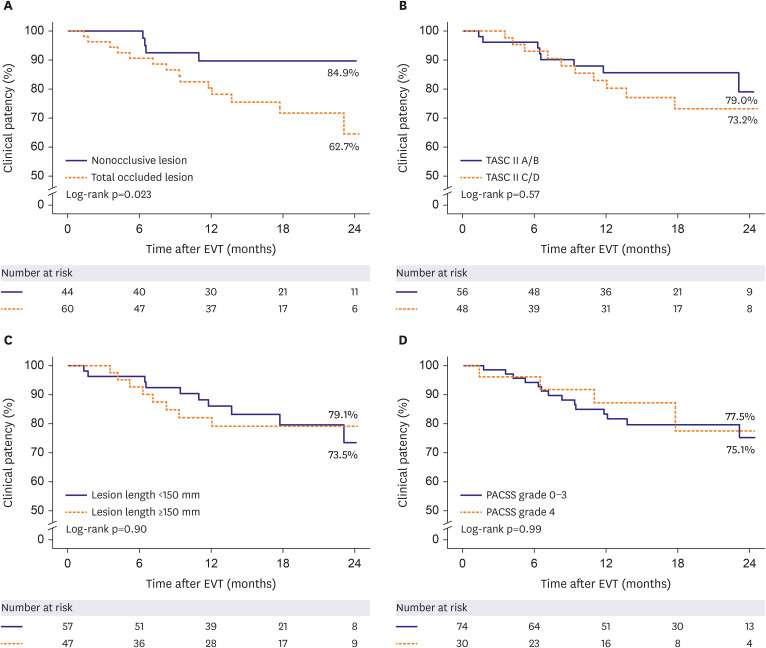
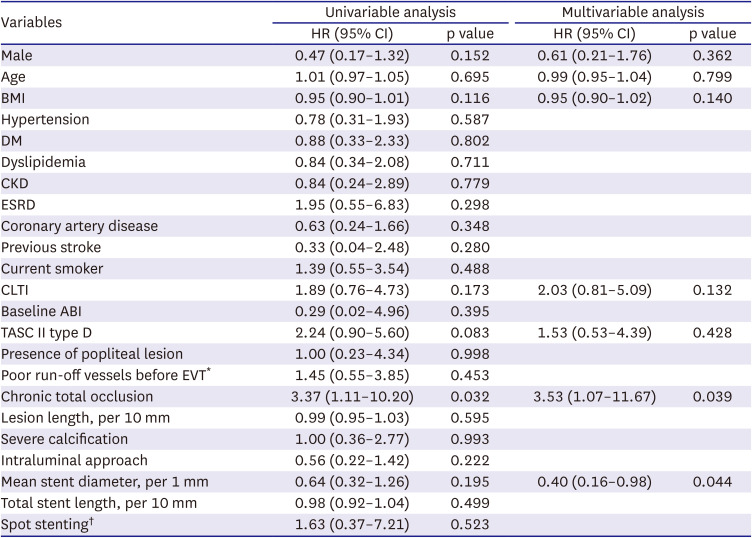
Figure 3
Kaplan-Meier curves and estimates of clinical patency over time (A) and TLR free–survival (B).
EVT = endovascular treatment; TLR = target lesion revascularization.
![]()
Figure 4
Kaplan-Meier curves and estimates of clinical patency over time according to lesion characteristics. Total occluded lesion (A), TASC II classification (B), lesion length (C), and calcification (D).
EVT = endovascular treatment; PACSS = Peripheral Arterial Calcium Scoring System; TASC II = Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease.
![]()
Table 3
Univariable and multivariable Cox proportional hazard analyses for predictors of loss of clinical patency
ABI = ankle-brachial index; BMI = body mass index; CI = confidence interval; CKD = chronic kidney disease; CLTI = chronic limb-threatening ischemia; DM = diabetes mellitus; ESRD = end-stage renal disease; EVT = endovascular treatment; HR = hazard ratio; TASC II = Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease.
*>2 tibial arterial lesions with >50% stenosis.
†Total length of stents/length of lesion <0.5.
![]()
One patient treated with subintimal angioplasty and Eluvia implantation developed an asymptomatic aneurysmal change in the target lesion, as detected on follow-up CT (Supplementary Figure 1). Three patients were found to have a hypoechoic halo surrounding the Eluvia stent on 1-year follow-up duplex ultrasonography (Supplementary Figure 2), which also was not associated with any symptoms.
DISCUSSION
In this single-arm prospective registry study, Eluvia, a self-expandable polymer-based paclitaxel-eluting stent, provided excellent clinical outcomes in terms of 2-year clinical patency (76.3%) and freedom from clinically driven TLR (79.1%).
The Eluvia is a fluoropolymer-based low-dose paclitaxel-eluting stent designed to release paclitaxel over 6 months. The clinical efficacy of Eluvia for femoropopliteal artery disease has been investigated in 2 randomized controlled trials. The EMINENT trial demonstrated superior 1-year primary patency with Eluvia stents than with BMS. At 1-year follow-up, Eluvia was associated with a primary patency rate of 83.2% and a TLR rate of 8.9%.13) In the IMPERIAL study, Eluvia was not only noninferior to but also superior to Zilver PTX (a nonpolymer-based paclitaxel-eluting DES) in terms of 12-month primary patency rate (86.8% vs. 81.5%).11)14) The results of IMPERIAL study suggested that even with a low paclitaxel dose, the polymer-based slow drug-releasing Eluvia stent more effectively prevents restenosis than the nonpolymer Zilver PTX stent.15)
Importantly, the mean lesion length in these 2 previous randomized controlled trials was <100 mm (75.6 mm in the EMINENT trial; 86.5 mm in the IMPERIAL trial), and the proportion of totally occluded lesions was relatively low (42.3% in the EMINENT trial; 31.2% in the IMPERIAL trial), compared with the proportion in real-world registries.1)15)16) Several prospective or retrospective registry studies have investigated the efficacy of the Eluvia stent for the treatment of more complex lesions. The largest study (in terms of sample size) was the CAPSICUM study, which was a prospective multicenter single-arm registry. It included a total of 1,204 limbs and documented 1-year clinical outcomes after femoropopliteal EVT with Eluvia of 87.1% primary patency rate and 93.8% TLR-free survival rate. These rates were comparable to those observed in the IMPERIAL trial, despite the mean lesion length being 186 mm, which was substantially longer than the length in the 2 randomized controlled trials.15) In a retrospective registry study, Stavroulakis et al.16) reported primary patency rates of 90% at 1 year and 71% at 2 years, as well as TLR-free survival rates of 94% at 1 year and 80% at 2 years, using Eluvia for femoropopliteal artery lesions with a mean length of 194 mm. The ULTIMATE study, a retrospective cohort study comparing the Viabahn stent graft (W L Gore & Associates Inc., Flagstaff, AZ, USA) and the Eluvia stent for long femoropopliteal artery lesions (mean lesion length, 230 mm) also found higher primary patency rates with Eluvia (75.9%) than with Viabahn (69.5%) at 24 months.17) Our current study, which included more complex femoropopliteal lesions than the randomized trials in terms of longer mean lesion length (168.3 mm) and a higher proportion of totally occluded lesions (57.7%), demonstrated clinical patency and clinically driven freedom from TLR rates similar to those reported in the previous real-world registry studies. Thus, Eluvia appears to also be an effective endovascular device for complex femoropopliteal lesions.
Previous studies reported CLTI, long lesion length, small reference vessel diameter, totally occluded lesions, and ESRD as risk factors for loss of patency or need for TLR after treatment with DES for femoropopliteal artery disease.15)18) Similarly, we also identified chronic total occlusion and smaller stent diameter as independent predictors of loss of patency at 2 years post-EVT in the present study.
Several studies reported cases of aneurysmal degeneration after Eluvia implantation,11)19)20) and 2 studies found incidences of 16.8% and 20% for dark halos around the stent (observed on duplex ultrasonography).15)16) Nevertheless, this halo sign has also been observed after implantation of BMS and stent grafts.21) In the EMINENT study, the incidence of halo signs was similar in the BMS and Eluvia stent groups.13) A study investigating EMINENT and IMPERIAL studies also concluded that there was no difference in the occurrence of halo signs across femoropopliteal arterial stent types.22) In the CAPSICUM study, subintimal angioplasty and use of intravascular ultrasonography were described as predictors of aneurysmal change.15) Thus, vessel injury from aggressive procedures may have led to the development of aneurysmal degeneration of the target lesions. However, the halos observed in the EMINENT study were not associated with aneurysm formation. Thus, the pathologic mechanism and long-term effects of the halo sign remain unclear. In the present study, one patient was observed to have aneurysmal changes on follow-up CT images, and 3 patients exhibited a hypoechoic halo sign around the stent on follow-up duplex ultrasonography. However, we cannot report the true incidence of aneurysmal change or halo sign because only a minority of patients underwent duplex ultrasonography during follow-up. Furthermore, transverse ultrasonography images, which provide the best view for diagnosing aneurysmal changes and hypoechoic halos surrounding stents, were not available for all of the patients evaluated with ultrasonography.
This study has limitations. First, it is a single-arm, nonrandomized study with a relatively small sample size. Second, the COVID-19 pandemic prevented some patients from returning to the hospital for follow-up visits, despite our best efforts. This resulted in a loss to follow-up rate of approximately 15%, with almost half of the participants being unable to undergo scheduled imaging assessments. Third, routine transverse ultrasonography was not incorporated into the follow-up assessments, which limited our ability to detect a halo sign or aneurysmal degeneration following Eluvia implantation.
The K-ELUVIA study demonstrated favorable 2-year clinical efficacy and safety outcomes of the Eluvia stent for femoropopliteal artery lesions in real-world practice.
 XML Download
XML Download