

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Percutaneous coronary intervention (PCI) using drug-eluting stents (DESs) has seen technological advancements and demonstrates outstanding safety and effectiveness characteristics. However, the persistence of repeated events such as late stent thrombosis and restenosis, with a nearly 2% annual risk following stent implantation, and the need for prolonged dual antiplatelet therapy (DAPT) have highlighted the necessity for alternative treatment approaches.1)2)3) The incidence of complex lesions such as multiple or diffuse calcified lesions, despite improvements in technology, often leads to suboptimal clinical outcomes, possibly due to the deployment of longer stents and an increased risk of stent-related factors.4)
Drug-coated balloons (DCBs) have emerged as a novel treatment option for coronary artery disease (CAD), offering an alternative to stents.5) DCB treatment leaves nothing within the vessel wall and maintains the anti-restenotic benefits, and it is free of the risk of stent-associated maladaptive biologic responses leading to restenosis and thrombosis, while promoting favorable natural vascular healing.6)
DCB treatment is currently recommended for managing in-stent restenosis (ISR) lesions arising from both bare-metal stents (BMS) and DES, as well as for treating de novo small vessel disease.7)8)9) Although more data are needed for other CAD scenarios, recent studies have emphasized DCB treatment as a promising alternative to conventional stent-based approaches in various CAD settings.10) Consequently, we will review the current therapeutic options for treating de novo CAD with DCB and evaluate the supporting evidence for their application. Furthermore, we intend to discuss future significant perspectives of DCB treatment for de novo CAD.
Go to : 
OPTIMAL LESION PREPARATION
The key to successful PCI for CAD lies not only in resolving epicardial coronary artery stenosis but also in optimizing coronary blood flow. Optimal lesion preparation is essential for ensuring proper blood flow to the myocardium supplied by the affected arteries, a procedure typically carried out through balloon angioplasty (BA). In a previous study, it was found that following BA, percent stenosis, intimal tear or dissection, and a pressure gradient of 20 mmHg or higher are associated with an increased risk of acute closure.11) In contrast, other studies have suggested that coronary dissection accompanied by a thrombolysis in myocardial infarction (TIMI) flow grade of 3 or uncomplicated, non-flow-limiting dissections are correlated with favorable results and predict a lower restenosis rate.12)13)
DCB consists of a matrix coating employed on the exterior of standard balloon catheter and it facilitates transfer from balloon surface to vessel wall. Though constructed similarly to conventional angioplasty, DCB serves a distinct purpose by delivering an anti-proliferative drug rather than resolving stenosis as BA does. Therefore, for successful local drug delivery, optimal lesion preparation prior to its application is a prerequisite factor. Optimal results from DCB treatment require the mandatory initial step of optimal lesion preparation, and the main goals of optimal lesion preparation are to improve blood flow by inducing dissection and to facilitate homogeneous drug delivery.
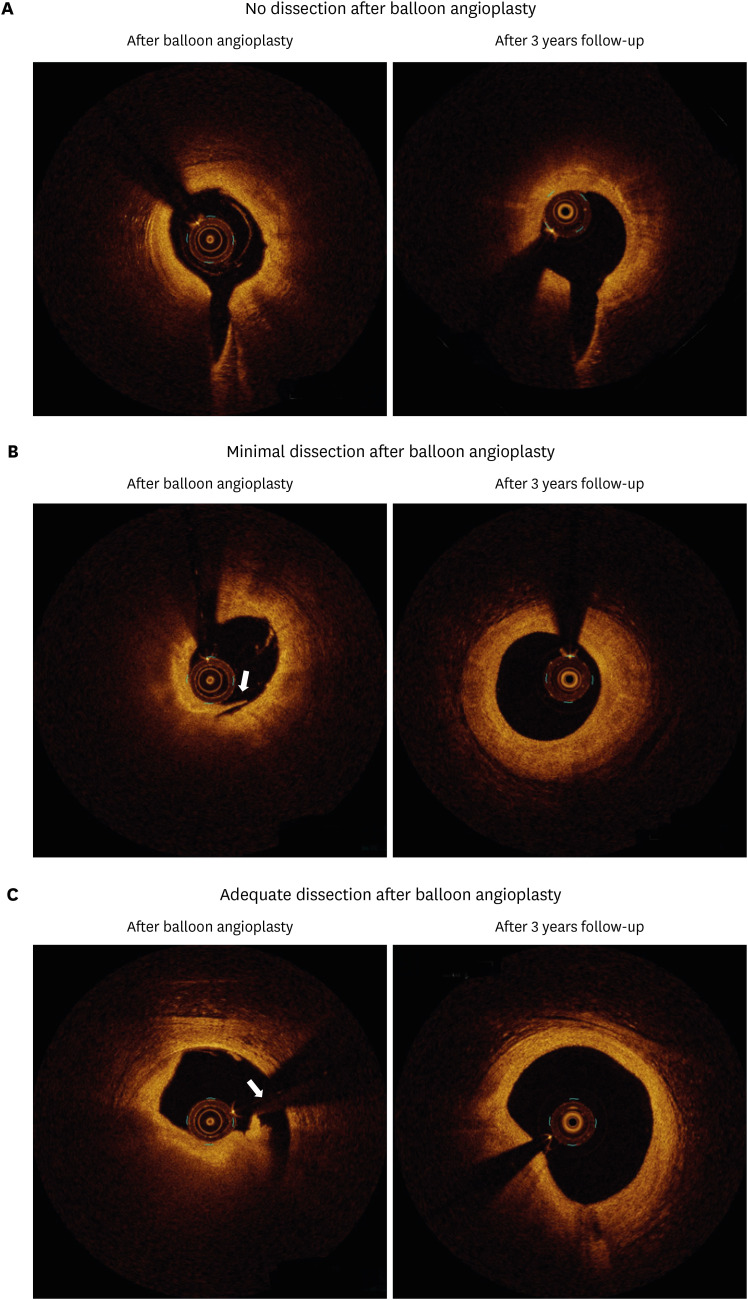
The most basic method of lesion preparation involves performing conventional angioplasty using a semi-compliant balloon with a balloon-to-vessel ratio of 1.0 and an inflation pressure exceeding nominal.6)14) In cases involving expected challenges with balloon delivery, vessel underfilling, or potential undersizing, it is reasonable to initiate treatment with a smaller balloon and reassess vessel dimensions after vasodilator usage.14) For more complex lesions, alternative techniques may be warranted, such as employing non-compliant high-pressure balloons, scoring or cutting balloons, and even considering rotablation, atherectomy, or lithotripsy. Additionally, potential adjunctive intravascular imaging techniques (such as intravascular ultrasound [IVUS] or optical coherence tomography [OCT]) or functional assessments (such as fractional flow reserve [FFR] or Instantaneous wave-free ratio) may be.15)16)17)18)19)20) Before considering DCB application, it is necessary for all 2 criteria to be met following BA: achieving TIMI grade 3 flow with the absence of a flow-limiting dissection, and maintenance of residual stenosis ≤30% (Figure 1).6)14)21) During angiography, it is essential to confirm the absence of delayed contrast clearance from both the vessel lumen and its walls, as well as from any potential dissection planes. The recent Korean data showed that fate of most non-flow limiting dissections less than type C after DCB was experienced benign heling process and can lead to positive remodeling at follow-up.22)23) Although evidence regarding the long-term effects of antiproliferative drug based on the degree of dissection is still lacking, current data suggests that long-term vascular remodeling varies according to the degree of dissection. The presence of adequate dissections tends to result in greater lumen enlargement, when flow is maintained. (Figure 2).24)
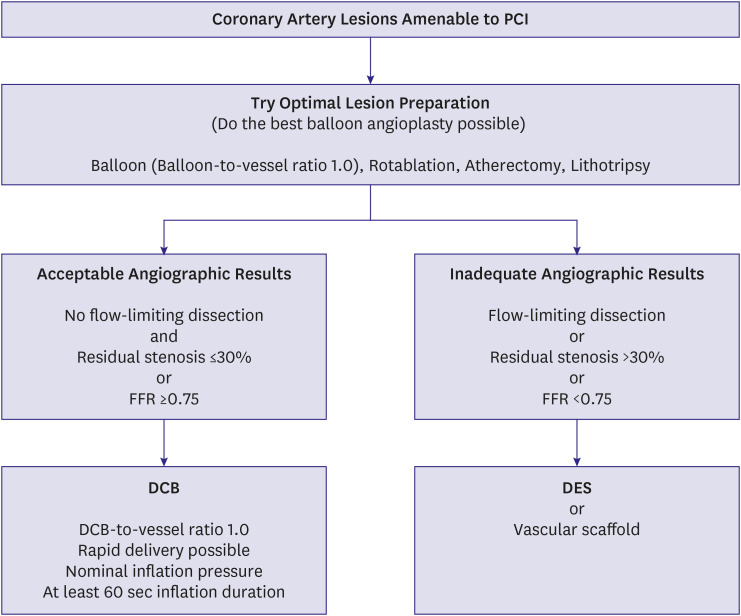
For larger vessels, the utilization of FFR after BA can assist in determining the appropriateness of treating the lesion with either DCB or DES. In the FFR-guided DCB treatment, when the FFR value following BA suggests that DCB treatment is appropriate (cutoff value of FFR ≥0.85), it ensures a safe and effective outcome with satisfactory anatomical and physiological patency observed during follow-up.15) Additionally, FFR-guided DCB treatment showed consistent anatomical and physiological patency with plaque redistribution and vessel remodeling without chronic elastic recoil or plaque compositional change during follow-up.25)26) Although validated data regarding the ideal FFR threshold following BA are limited, based on clinical efficacy, a value of 0.75 is suggested as a reasonable compromise for guiding angioplasty according to the current consensus (Figure 1).6)16)
If angiographic results meet the criteria, the application of DCB may be considered. The DCB should extend beyond the pre-dilated area by 2–3 mm on each side to prevent geographic mismatch. Maintaining appropriate sizing is essential, with the DCB diameter matching that of the target vessel, and the recommended balloon-to-vessel ratio of 1.0. Inflation of the DCB should last for at least 60 seconds at nominal pressure to minimize the risk of further dissection or bailout stenting, though a shorter inflation time (e.g., 30 seconds) may be acceptable if the patient cannot tolerate a longer duration. It is important to note that the primary purpose of the DCB is drug delivery, rather than solely the resolution of vessel stenosis, as in conventional BA. The product company advises that the DCB should ideally reach the lesion within 2 minutes from vascular access, so it is advisable to aim for faster delivery whenever possible. If the drug persists in the aqueous environment for an extended duration (delayed inflation time >25 seconds) and shorter contact duration with the target lesion (total inflation time <60 seconds) might elevate target lesion failure (TLF) by nearly 2.0 fold, respectively.27)
Go to :
SMALL VESSEL DISEASE
Coronary small vessel disease, usually defined as CAD affecting vessels with diameter less than 3 mm, has been recognized as a challenging aspect of coronary revascularization due to its association with increased risks of restenosis and stent thrombosis after DES implantation.28)29) However, the potential role of DCB treatment in small vessel disease is noteworthy, as the proportion of lumen loss following stent implantation constitutes a larger percentage of the total lumen diameter in small vessel compared to larger vessel. The larger randomized BASKET-SMALL (Basel Kosten Effektivitäts Studie - Drug-Coated Balloons in Small Coronary Artery Lesions) 2 trial demonstrated that DCB treatment showed comparable effectiveness to second-generation DES for de novo small vessel disease. The combined outcome of major adverse cardiovascular event (MACE) up to the 3-year follow-up showed comparable rates across both groups (15% vs. 15%; hazard ratio [HR], 0.99; 95% confidence interval [CI], 0.68, 1.45, p=0.95).8) Furthermore, the other randomized PICCOLETO (Drug Eluting Balloon Efficacy for Small Coronary Vessel Disease Treatment) II trial in patients with small vessel disease suggested the superiority of DCB over DES (everolimus-eluting stent) in relation to late lumen loss (LLL, 0.04 mm vs. 0.17 mm, p=0.001 for noninferiority; p=0.03 for superiority).30) In the latest meta-analysis of 29 randomized controlled trials (RCTs) including 8,074 patients with small vessel CAD, there were no significant differences in any clinical outcomes between DCB and new-generation DES.31) Therefore, DCB treatment has emerged as a viable option for managing de novo small vessel disease in CAD.
Go to :
LARGE VESSEL DISEASE
Based on the promising outcomes observed with DCB treatment in small vessel disease, there is increasing evidence supporting the effectiveness and safety of DCB treatment for de novo large (≥3.0 mm) coronary vessels.32)33)34) When encountering persistent dissections and angiographically restricted acute luminal gain following pre-dilatation, employing FFR can provide a more precise assessment of the functional outcome. This approach is based on the concept that a FFR value at the ischemic threshold indicates a suitable condition to refrain from treatment.6)14)15)16) Recent data from Korea has shown that FFR-guided DCB treatment is both proven to be safe and efficacious in managing de novo lesions within large coronary arteries, even among patients with acute coronary syndrome.15) At the 9-month follow-up, favorable anatomical and physiological patency was noted. Notably, the LLL was significantly lower with DCB compared to DES (0.05±0.27 mm vs. 0.40±0.54 mm, p=0.022), while there was no significant difference in the FFR values between the 2 groups at 9-month follow-up (0.85±0.08 vs. 0.85±0.05, p=0.973). The authors suggest that DCB treatment enhances the restoration of coronary blood flow through plaque modification, leading to a progressive enlargement of the minimal lumen area as demonstrated by intravascular imaging modalities like IVUS or OCT.25)26)35)36) Additional European data has shown that using FFR guidance, a DCB-only approach was shown to be both safe and feasible for treating stable CAD, demonstrating positive remodeling with no compromise to lumen patency as confirmed by OCT after the 6-month follow-up.37)
Recent observational studies have indicated that the effectiveness and safety of DCB treatment were similar for both de novo non-small coronary lesions and small vessel disease.22)38) Her et al.22) demonstrated that there was no significant difference in target vessel failure between the 2 groups during the 3.4-year follow-up (7.0% vs. 7.9%, p=0.596). In a latest study focusing on left anterior descending (LAD) lesions, Gitto et al.39) found that the DCB-based treatment for LAD was safe and resulted in acceptable rates of adverse events at 2 years follow-up compared to contemporary DES (TLF; DCB: 4.1% vs. DES: 9.8%; HR, 0.51 [95% CI, 0.20, 1.27], p=0.148). After a 1:1 propensity score matching, DCB-based treatment was associated with a lower risk of TLF compared to DES-only PCI, primarily due to reduced instances of target lesion revascularization (TLR) (HR, 0.2 [95% CI, 0.07, 0.58], p=0.003). Another recent meta-analysis suggested that DCB treatment was non-inferior to DES implantation for managing de novo large coronary lesions, with similar rates of TLR observed at 6–9 months follow-up (risk ratio [RR], 1.17; 95% CI, 0.46, 2.95; p=0.746).40) This suggests that the use of DCB treatment for large CAD leads to enduring beneficial anatomical patency, vascular restoration, and positive long-term clinical results. Therefore, DCB treatment might provide a safe and efficient strategy for the management of de novo large CAD, despite the limited number of randomized trials comparing DCB with DES for this indication. The ongoing REVERSE (Randomised Trial of Drug-Coated Balloon Versus Drug-Eluting Stent for Clinical Outcomes in Patients With Large Coronary Artery Disease) trial (ClinicalTrials.gov: NCT05846893) is currently comparing the safety and effectiveness of DCB with DES for large vessel disease (≥3.0 mm), with expected results to reveal clinical outcomes in de novo large vessel CAD.
Go to :
BIFURCATION DISEASE
Patients with coronary bifurcation lesions typically suffer from worse long-term clinical outcomes, characterized by a higher incidence of cardiac death, myocardial infarction (MI), and the need for revascularization of both main vessel and side-branch.6)14)41)42) The recent PEPCAD-BIF trial, a randomized study comparing the Paclitaxel-Eluting Percutaneous Coronary Angioplasty-Balloon Catheter with conventional BA in treating coronary bifurcations, along with a meta-analysis, demonstrated a significantly lower restenosis rate in the DCB group compared to the BA group when the side-branch was treated solely with DCB.43)44) In the Korean OCT study, where only the main vessel received treatment with a DCB-only approach, provided evidence for the safety of DCB treatment in bifurcation lesions.45) Despite the absence of direct intervention on the side-branch, the study observed an increase in the lumen area at the side-branch ostium, with measurements showing 0.92±0.68 mm2 pre-procedure, 1.03±0.77 mm2 post-procedure, and 1.42±1.18 mm2 at 9 months follow-up. In the specific context of left main bifurcation lesions, Pan et al.46) identified that employing a hybrid strategy, combined with DCB and DES, yielded superior results compared to a DES-only strategy (provisional stenting or 2-stent strategies) in terms of LLL and TLF. Patients treated with DES alone showed significantly higher LLL at 1 year compared to those in the DCB group (0.42±0.62 mm vs. 0.13±0.42 mm, p<0.001). Additionally, the incidence of TLF within 2 years was lower in the DCB group (7.6%) compared to the DES group (14.4%), with an odds ratio (OR) of 0.49 (95% CI, 0.26, 0.92; p=0.025; log-rank p=0.024). Recent studies have showed that DCB treatment subsequent to coronary atherectomy for bifurcation lesions, even when involving the left main coronary artery, could lead to a reduction in the number of stents required, avoidance of complex stent placement techniques, and yield favorable clinical outcomes.47)48) While the optimal strategy and precise role of DCB treatment in bifurcation diseases remain uncertain, it emerges as a potential alternative option for managing bifurcation lesions.
Go to :
DIFFUSE LONG DISEASE AND MULTIVESSEL DISEASE
In cases of CAD with diffuse involvement and multivessel conditions, as well as lesions with high stent burden, the placement of multiple lengthy metallic devices within coronary arteries might compromise the restoration of vasomotion in the stented segment.6) This compromise is associated with stent-related complications such as ISR, stent thrombosis, neoatherosclerosis, and may also restrict the feasibility of coronary artery bypass graft surgery. In a retrospective study on the treatment of diffuse CAD (>25 mm), patients who underwent a DCB approach, whether alone or combined with DES, were evaluated against those of DES alone.49) The clinical results related to the DCB approach were found to be comparable to those of DES alone at the 2-year follow-up. Specifically, MACE occurred in 20.8% of patients in the DCB group vs. 22.7% in the DES-alone group (p=0.74), target vessel revascularization (TVR) rates were 14.8% vs. 11.5% (p=0.44), and TLR rates were 9.6% vs. 9.3% (p=0.84). Another observational study (lesion length >25 mm) found that the long-term effectiveness and safety outcomes associated with the DCB strategy (either DCB alone or in combination with DES) were comparable to those of DES alone in diffuse coronary lesions. This was supported by similar rates of TLR (7.3% vs. 8.3%, log-rank p=0.636) and MACE (11.3% vs. 13.7%, log-rank p=0.324) observed at the 3-year follow-up.50) Shin et al.51) recently conducted a study on multivessel CAD, revealing that the use of a DCB-based treatment approach (using DCB alone or in combination with DES) led to a significant reduction in stent burden and resulted in a lower incidence of MACE compared to treatment with DES alone (3.9% vs. 11.0%, p=0.002) at the 2-year follow-up. These findings indicate that a DCB-based treatment strategy for diffuse long diseases and multivessel diseases effectively reduces stent burden and may lead to improved long-term outcomes by reducing stent-related events.
Go to :
DIABETES MELLITUS
Diabetic patients are commonly regarded as being at heightened risk for cardiovascular events and tend to experience poorer outcomes following PCI, with increased rates of ISR, stent thrombosis, MI, and mortality.52) Additionally, it states that they are considered typical examples of both diffuse long disease and multivessel disease. This is primarily attributed to the presence of more complex, diffuse, and lengthy lesions in smaller coronary vessels, along with a diminished coronary vasodilator reserve. Results from the previous trial indicated that diabetic patients receiving DCB prior to BMS showed markedly superior outcomes when compared to those who received BMS alone, with outcomes similar to those observed with DES.53) Additionally, a latest subgroup analysis of the BASKET-SMALL 2 trial revealed that DCB treatment was as effective as DES, with a significantly lower need for TVR observed with DCB compared to DES in diabetic patients (9.1% vs. 15.0%; HR, 0.40; 95% CI, 0.17, 0.94, p=0.036).54) In recent Korean study, Her et al.55) showed that in patients with multivessel CAD, the clinical advantage of a DCB-based revascularization strategy seems to be more pronounced in diabetic patients compared to non-diabetic patients after 2-year follow-up. Specifically, the DCB-based group exhibited a significantly reduced risk of MACE in diabetic patients (HR, 0.19; 95% CI, 0.05, 0.68; p=0.003), while this reduction in risk was not observed in non-diabetic patients (HR, 0.52; 95% CI, 0.20, 1.38; p=0.167). Despite the requirement for additional data and thorough analyses, DCB treatment may represent a promising alternative to DES implantation in diabetic patients.
Go to :
CHRONIC TOTAL OCCLUSION
Chronic total occlusion (CTO) poses substantial technical hurdles in PCI, and accurately sizing the stent following BA can be challenging, often leading to underestimated stent dimensions and the potential for late stent malapposition. Furthermore, performing a ‘full-metal jacket’ PCI using overlapping DES is associated with a high adverse event rate.56) In a previous trial, 2 independent predictors of TLF in “full-metal jacket” PCI were identified: number of target vessel DES (HR, 1.72; 95% CI, 1.16, 2.54; p=0.006) and persistent distal luminal narrowing (HR, 2.73; 95% CI, 1.66, 4.47; p<0.001).57) In the PEPCAD CTO (Percutaneous Transluminal Coronary Angioplasty-Balloon Catheter in Coronary Artery Disease to Treat Chronic Total Occlusions) trial, angiographic observations and clinical results in the cohort receiving BMS along with DCB showed no significant differences compared to those in the DES cohort (restenosis: 28% vs. 21%, p=0.44; MACE: 15% vs. 19%, p=0.58).58)
Another recent study indicated that employing a DCB-only approach without stenting proved to be a practicable and well-tolerated therapeutic strategy for CTO, particularly when the results of predilatation were satisfactory.59) Although the development of devices, procedural techniques, and medication regimens for preventing very late events is necessary to further improve lifelong outcomes in patients undergoing coronary revascularization,60) adopting a DCB-based treatment approach provides potential benefits for managing CTO lesions.
Go to :
ACUTE MYOCARDIAL INFARCTION
As the most representative disease characterized by atherothrombotic lesions, acute myocardial infarction (AMI) has seen significant advancements in reducing repeat revascularization through stent implantation. However, persistent risks of stent thrombosis and ISR remain in AMI patients.61) Hence, DCB treatment could be considered as an alternative therapeutic option for AMI, particularly when coronary flow returns to normal and residual stenosis is minimal after thrombus aspiration and balloon dilatation.6) According to findings from the REVELATION (Revascularization with Paclitaxel-Coated Balloon Angioplasty Versus Drug-Eluting Stent in Acute Myocardial Infarction) trial, DCB treatment was shown to be non-inferior to DES in terms of FFR assessment at the 9-month follow-up (0.92±0.05 vs. 0.91±0.06, p=0.27).62) These findings suggest that DCB treatment may represent a safe and viable strategy in the management of ST-segment elevation MI. In the context of non-ST-segment elevation MI, it was demonstrated that DCB treatment was comparable to stenting using either BMS or DES (TLF: 3.8% vs. 6.6%, p=0.53).63) Additionally, the recent meta-analysis, encompassing 9 studies and over 2,000 acute coronary syndrome cases, showed the feasibility of DCB treatment in comparison to recent DES implantation.64) Statistical analysis confirmed both the clinical safety and angiographic efficacy of DCB treatment across various MACE, including MACE, cardiac mortality, all-cause mortality, MI, bleeding events, TVR, TLR, and LLL. These findings suggest the need for extended investigation of DCB treatment in this context, preferably through large scaled randomized trials with DES as control groups.
Go to :
HIGH BLEEDING RISK
Post-PCI bleeding is associated with increased mortality and can lead to additional adverse events such as MI, prolonged hospitalization, emphasizing the importance of its prevention.14)65) Despite the shortened duration of DAPT after DES implantation, consideration for cessation of antiplatelet agents may be considered earlier after DCB treatment, particularly in instances of severe, life-threatening bleeding, compared to DES implantation. The DEBUT (Drug-coated balloon for treatment of de novo coronary artery lesions in patients with high bleeding risk) trial demonstrated that in patients identified as high risk for bleeding, DCB treatment showed superiority over BMS (MACE: 1% vs. 14%; RR, 0.07; 95% CI, 0.01, 0.52, p<0.00001 for noninferiority, p=0.00034 for superiority at 9 months).9) FFR-guided DCB treatment has demonstrated superior efficacy in terms of both angiographic and physiologic patency compared to BMS at the 9-month follow-up, with only 1 month of DAPT, in patients considered to be at high risk of bleeding (LLL: 0.2±0.3 mm vs. 1.2±0.8 mm, p<0.001; FFR: 0.87±0.06 vs. 0.89±0.06, p=0.254).66) Therefore, DCB treatment may confer benefits compared to stent placement in patients who are at a high risk of bleeding, and DCB treatment warrants future comparison to new-generation DES.
Go to :
SIROLIMUS-COATED BALLOON
There is a diverse range of DCB available for use in coronary interventions (Table 1). Although the paclitaxel is the most widely used drug for balloon coating because of its high lipophilic profile and potent anti-proliferative effect,67) recent studies have been focused on various coatings and drug delivery technologies.5)68)69)70)71) All contemporary DES uniformly release sirolimus or limus analogues. They exhibit superior outcomes compared to paclitaxel-eluting stent (PES) across various indications. Additionally, there is an observed increased risk of stent thrombosis with PES compared to BMS and sirolimus-eluting stent.72) Although sirolimus exhibits enhanced safety and efficacy compared to paclitaxel when delivered from a coronary stent, its application on a DCB, which requires rapid drug release and short transfer times, may be hindered by its low lipophilicity and limited penetration and retention in the target vessel wall, especially in the adventitia. In the first-in-human RCT comparing a novel sirolimus-coated balloon (SCB) compared with a well-established paclitaxel-coated balloon (PCB) with de novo coronary lesions, SCB with a crystalline coating showed similar angiographic results.73) After 6 months, in-segment LLL was 0.10±0.32 mm in the SCB group vs. 0.01±0.33 mm in the PCB group. However, a higher incidence of late lumen enlargement was noted in patients with PCB treatment (32% in the SCB group vs. 60% of lesions in the PCB group, p=0.019). In the TRANSFORM I (TReAtmeNt of Small Coronary Vessels: MagicTouch Sirolimus Coated Balloon) trial, patients diagnosed with de novo single-vessel disease (≤2.75 mm) have been randomly assigned to receive either the MagicTouch SCB or the SeQuent Please Neo PCB.74) The primary objective was to evaluate in-segment net lumen gain via angiography at the 6-month follow-up, and the SCB failed to demonstrate noninferiority compared to the PCB in terms of angiographic net gain at 6-month follow-up. The mean angiographic net gains were 0.25±0.40 mm with SCB compared to 0.48±0.37 mm with PCB, and SCB did not meet the 0.30 mm criterion for noninferiority (p for noninferiority=0.173), showing an absolute difference of −0.23 mm (95% CI, −0.37, −0.09) primarily due to a smaller late loss (0.00±0.32 mm vs. 0.32±0.47 mm; p<0.001) and a higher frequency of late lumen enlargement with PCB (53.7% vs. 30.0%; OR, 2.60; 95% CI, 1.22, 5.67; p=0.014). In contrast to stent-based drug delivery, paclitaxel is observed to yield better angiographic outcomes than sirolimus in DCB treatment. Nevertheless further investigation through larger and more extensive studies with adequate statistical power to evaluate clinical outcomes are necessary to establish the efficacy of SCB compared to PCB in de novo lesions.
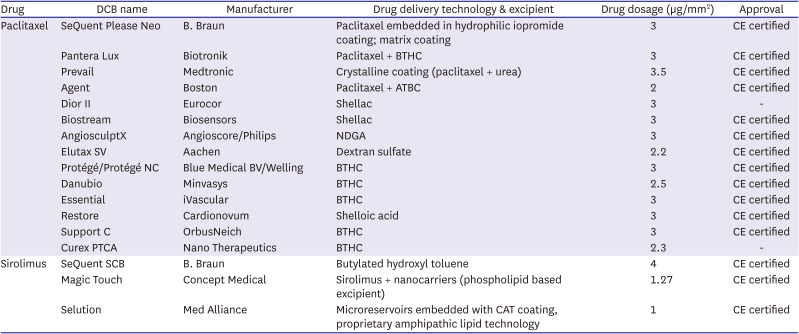
Table 1
A list of current commercially available coronary DCBs
ATBC = acetyl-tri-n-butyl citrate; BTHC = n-butyryl tri-n-hexyl citrate; CAT = cell adherent technology; CE = conformite Europeenne; DCB = drug-coated balloon; NDGA = nordihydroguaiaretic acid.
![]()
Go to :
FUTURE PERSEPCTIVES
Despite recent data showing more promising outcomes in terms of the safety and efficacy of DCB treatment in various clinical and angiographic settings, a significant number of ongoing trials and studies remain, aiming to provide further clarity on the feasibility of DCB as an alternative to stent implantation.
The REVERSE (Randomised Trial of Drug-Coated Balloon Versus Drug-Eluting Stent for Clinical Outcomes in Patients With Large Coronary Artery Disease) trial (ClinicalTrials.gov: NCT05846893) aims to demonstrate the non-inferiority of DCB treatment against current-generation DES in patients with de novo lesions in large CAD (reference vessel diameter ≥3.0 mm by visual estimation). The STENTLESS (STrategies of Scheduled Drug-coated Balloons Versus Conventional DES for the interveNTional Therapy of de Novo Lesions in Large Coronary vESSels) trial (ClinicalTrials.gov: NCT06084000) is a randomized controlled study to compare the safety and efficacy of scheduled DCB and conventional DES strategy in the treatment of de novo large coronary vessels with diameter larger than 2.75 mm. The other trial (ClinicalTrials.gov: NCT04664283) intends to assess whether DCB is non-inferior to DES in treating large vessel disease (vessel diameter 3.0–4.5 mm), as evaluated by OCT.
The DCB-BIF (Drug-coating Balloon Angioplasties for True Coronary Bifurcation Lesions) trial (ClinicalTrials.gov: NCT04242134) is designed to investigate whether DCB compared to conventional BA for side-branch after provisional stenting in true coronary de novo bifurcation lesions will lead to lower rates of the composite endpoint of MACE at 12 months.75)
The D-Lesion Long (PCB for Long De Novo Lesions of Main Coronary Arteries) trial (ClinicalTrials.gov: NCT03155971) compares a DCB vs. a DES approach in patients with de novo long coronary lesions, and the primary endpoint is LLL assessed by angiography.
The ULTIMATE-III (Intravascular Ultrasound Versus Angiography Guided Drug-coated Balloon) trial (ClinicalTrials.gov: NCT04255043) is designed to compare IVUS-guided and Angiography-guided DCB treatment for coronary de novo lesions in patients with high bleeding risk. The DCB-HBR (Drug-Coated Balloon Versus Drug-Eluting Stent for Treatment of De-Novo Coronary Lesions in Patients With High Bleeding Risk) trial (ClinicalTrials.gov: NCT05221931) aims to compare clinical outcomes of DCB with DES for treatment of de novo coronary lesion under intravascular imaging-guided optimization in patients with high bleeding risk. The DEBATE (Drug-Coated Balloon in Anticoagulated and Bleeding Risk Patients Undergoing PCI) trial (ClinicalTrials.gov: NCT04814212) is proposed to compare DCB with DES in stable CAD or acute coronary syndrome patients who are at high risk of bleeding. The hypothesis of the DEBATE trial is that the strategy using DCB and a shorter DAPT regimen is non-inferior to the treatment using DES and longer DAPT duration in patients on anticoagulation or otherwise on high bleeding risk.
The TRANSFORM II trial (ClinicalTrials.gov: NCT04893291) aims to address the gap in understanding the use of DCB for treating small and medium-sized de novo coronary lesions (2–3 mm) by conducting a comparative analysis between MagicTouch DCB and everolimus-eluting stents, focusing on the TLF at 12-month follow-up.76) Additionally, the PICCOLETO III randomized trial will perform a 3-arm comparison among the MagicTouch SCB, a new-generation PCB, and the latest-generation DES in the setting of complex coronary lesions.
Go to :
CONCLUSIONS
Although additional evidence is required to clarify the efficacy of DCB treatment across various lesion subsets, it remains an appealing therapeutic option and could play a significant role in managing de novo coronary lesions. PCI now has an additional therapeutic option in DCB, allowing for the improvement of patient outcomes by addressing lesions that were previously challenging or less responsive to DES implantation. DCB treatment may be considered if there is no flow-limiting dissection and the residual diameter stenosis is acceptable after BA, particularly in the context of treating de novo CAD. For more complex lesions such as de novo large vessel disease including left main stenosis, bifurcation disease, complex high-risk and indicated PCI, further utilization of intravascular imaging or functional measurements can provide valuable insights. Additionally, advancements in DCB technology, along with improvements in imaging techniques, physiological guidance, along with supplementary pharmacotherapy, will be crucial for improving clinical outcomes in the management of de novo CAD. Finally, the development and implementation of new-generation bioresorbable scaffolds in the future may enable metal-free PCI in conjunction with DCB, which could bring about changes in the field of PCI and improvements in outcomes for patients of CAD.
Go to :
 XML Download
XML Download