

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute liver failure (ALF) is a rare but life-threatening condition characterized by an altered mental status and coagulopathy in patients without pre-existing liver disease [12]. Liver transplantation (LT) is the only life-saving intervention for patients with irreversible ALF, and the availability of a life-saving graft and timing of LT are crucial because ALF is frequently associated with significant mortality and morbidity attributable to cerebral edema and multisystem organ failure [34]. In Western countries, deceased donor liver transplantation (DDLT) is the main treatment for patients with irreversible ALF. In Asian countries, despite having the highest priority, DDLT is restricted because of the limited number of deceased organ donations; therefore, living donor liver transplantation (LDLT) is the only life-saving alternative to DDLT for patients with ALF [45].
LT has been established as a crucial treatment for ALF, and studies have reported evidence that supports the use of LDLT for ALF in adult patients [678]. These studies have described favorable survival rates of recipients and low morbidity rates of living donors, as well as advantages such as reduced waiting times and improved transplantation timing compared with those of DDLT. However, the adoption of LDLT for ALF has been approached with caution, mainly because of concerns regarding recipient outcomes and donor safety. The main concerns are whether a partial graft would lead to worse survival outcomes for critically ill recipients of highly urgent LT and whether urgent evaluations of live donors could result in the selection of inappropriate donors [910]. These issues highlight the need for careful evaluation and selection to ensure optimal outcomes for both donors and recipients. During this retrospective study, we aimed to evaluate the safety and efficacy of LDLT for ALF by comparing its surgical and survival outcomes with those of DDLT and to identify factors associated with survival after LT for ALF. The findings of this study provide valuable insights into the role of LDLT for irreversible ALF, potentially influencing clinical decision-making processes.
METHODS
Ethical considerations
Each transplantation was evaluated and approved by the local authorities and the Korean Network for Organ Sharing affiliated with the Ministry of Health and Welfare of the Republic of Korea. The study design was reviewed and approved by the Institutional Review Board of Asan Medical Center, University of Ulsan College of Medicine (No. 2022-1070). The requirement for informed consent was waived because of the retrospective nature of the study.
Study design and patient population
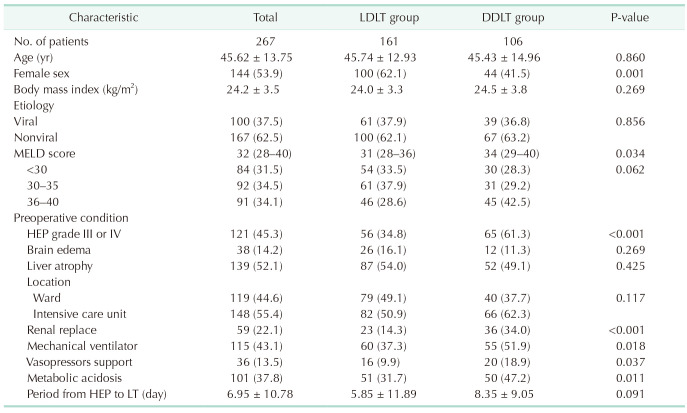
We retrospectively reviewed the medical records of 7,195 patients who underwent LT (5,970 living donors and 1,225 deceased donors) at Asan Medical Center in Seoul, Korea, between January 2006 and December 2020. Among 267 adult patients (18 years or older) who underwent LT for ALF, 161 underwent LDLT and 106 underwent DDLT. The mean age of all recipients was 45.6 years (±13.8 years), and 144 recipients (53.9%) were male. The leading cause of liver failure was toxic hepatitis (n = 167, 62.5%) resulting from drug-induced or chemical-induced liver injury, and 100 recipients (37.5%) had viral hepatitis, including hepatitis B and hepatitis A. At the time of LT, the mean Model for End-stage Liver Disease (MELD) score was 32.1 (±6.3). Preoperatively, 148 patients (55.4%) required treatment in the intensive care unit (ICU), and 115 patients (43.1%) required mechanical ventilation. Fifty-nine patients (22.1%) required renal replacement therapy. A total of 121 patients (45.3%) presented with grade III or IV hepatic encephalopathy (HEP), whereas brain edema and liver atrophy were observed in 38 (14.2%) and 139 patients (52.1%), respectively. The mean duration between the onset of HEP and LT was 6.9 days (±10.8 days). The preoperative characteristics of the patients who underwent LT because of ALF are summarized in Table 1.
In this study, ALF was defined as acute deterioration of liver function with a PT/international normalized ratio (INR) ≥1.5 and HEP in patients without cirrhosis or pre-existing liver disease within 26 weeks of the onset of symptoms [11112]. We excluded patients with chronic liver disease observed during histopathologic examination.
Institutional approach to potential candidates for emergency liver transplantation
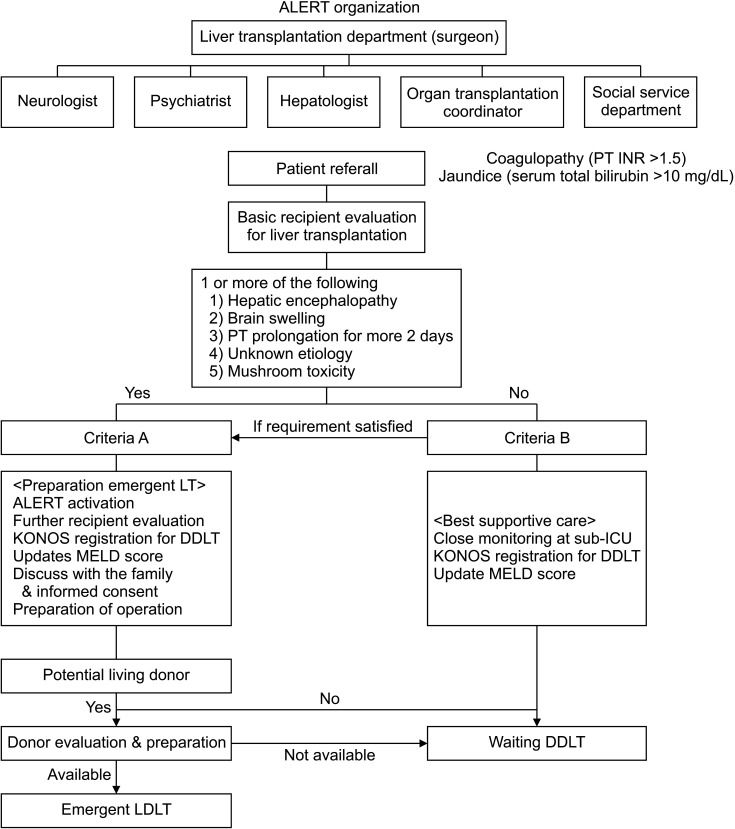
The Acute Liver Failure Emergency Response Team was organized to manage patients with ALF using a multidisciplinary approach. This team includes liver surgeons, hepatologists, neurologists, psychiatrists, organ transplantation coordinators, and members of social service departments. When patients are diagnosed with ALF, or when it is expected that patients will experience progression to ALF, the Acute Liver Failure Emergency Response Team initiates their evaluation and management to determine the need for LT. Patients are classified into the criteria A or criteria B groups. The criteria A group includes patients who meet the criteria of the criteria B group plus one or more of the following 5 conditions: HEP; brain swelling observed during CT; PT deterioration for more than 2 days; unknown etiology; and mushroom toxicity. The criteria B group includes patients without chronic liver disease who are expected to experience ALF and have at least one of the following conditions: PT/INR ≥1.5 and serum total bilirubin level >10 mg/dL.
Patients classified as the criteria A group require immediate LT. They are placed on the waitlist for DDLT and undergo an evaluation to determine whether they are candidates for LDLT. Additionally, a potential living donor evaluation is performed. Emergency LDLT is performed if a suitable living donor is available. Otherwise, these patients remain on the waitlist for DDLT and receive supportive medical care. If the patient is allocated to receive DDLT while preparing for LDLT, then DDLT is prioritized. Patients in the criteria B group are placed on the waitlist for DDLT as a preemptive action. These patients receive supportive medical care, and their liver function and clinical symptoms are closely monitored. The requirement for LT among these patients is continually reevaluated based on their clinical progression. The classification of patients with ALF and the management of LT candidates with ALF at our institution are illustrated in Fig. 1.
Preoperative evaluation of living donors
The donor evaluation for urgent LDLT shortens the timeframe and ensures that absolutely nothing is omitted compared to the elective donor evaluation. The volunteers undergo independent interviews with both a psychiatrist and transplantation surgeon to ensure that they fully understand the nature of the surgery and that their decision to donate is voluntary. Details of the donor selection criteria and evaluation process for adult LDLT at our institution have been previously described [1112].
Perioperative management of recipients
Patients with ALF are managed using a multidisciplinary approach before transplantation. Patients who present with grade III or IV HEP are managed and monitored in the ICU or subacute ICU and undergo elective endotracheal intubation to protect the airway. The management of HEP primarily involves the correction of precipitating factors and supportive care to minimize the risk of intracranial hypertension. Norepinephrine is the vasopressor of choice, and continuous venovenous hemofiltration is actively used as renal replacement therapy to control persistent hyperammonemia, hyponatremia, acidosis, and metabolic disturbances. Broad-spectrum antibacterial agents are administered as prophylactic treatment. Coagulopathy associated with ALF is proactively corrected by administering plasma products.
The surgical techniques for patients with ALF are similar to those used for patients who require transplantation because of other diseases. However, if long-term ICU care is anticipated after surgery, then feeding jejunostomy is performed during LT to facilitate early postoperative tube feeding unless contraindicated by conditions such as severe bowel edema. Surgical procedures for DDLT and LDLT, including dual LDLT, have been described in detail elsewhere [111314]. The standard immunosuppressive regimen consists of a triad comprising a calcineurin inhibitor, mycophenolate mofetil, and corticosteroid and anti-IL-2 induction.
Statistical analyses
All statistical analyses were conducted using SAS ver. 9.4 (SAS Institute) with the GMATCH SAS macro. Categorical variables are presented as numbers and percentages, and continuous variables are presented as medians and interquartile ranges. The 2-sample t-test or Wilcoxon rank-sum test for continuous data and the chi-square test or Fisher exact test were used to compare patient background characteristics and surgical outcomes of the LDLT and DDLT groups. During the analyses of time-to-event data, the Kaplan-Meier method was used to estimate survival. During the multivariable analysis performed to assess the association between in-hospital mortality and various predictors, a logistic regression model was used. Two-tailed P-value of <0.05 was considered statistically significant.
RESULTS
Our experience with liver transplantation for acute liver failure
Among the 267 patients evaluated in this study, the morbidity rate of those with ALF who underwent LT was 36.3%. Fifty-six patients died during follow-up; of these, 34 (12.7%) died in the hospital. The median recipient follow-up period was 95.9 months (±61.7 months; range, 0.1–198.9 months). Patient survival rates at 1, 5, 10, and 15 years after LT were 90.7.8%, 89.7%, 88.1%, and 85.3%, respectively. The liver graft survival rates at 1, 5, 10, and 15 years were 85.4%, 81.3%, 78.7%, and 75.9%, respectively.
Comparison of living and deceased donor liver transplantation for acute liver failure
The preoperative characteristics of recipients in the LDLT and DDLT groups were compared (Table 1). The age (LDLT, 45.7 years vs. DDLT, 45.4 years; P = 0.56), body mass index (24.0 kg/m2
vs. 24.5 kg/m2, P = 0.269), and ALF etiology (P = 0.856) of both groups were comparable. However, notable differences in disease severity, as reflected by the MELD scores (31.0 vs. 34.0, P = 0.34) and clinical conditions, of the LDLT and DDLT groups were observed. Before LT, there was no significant difference in the ICU admission rate (50.9% vs. 62.3%, P = 0.117). However, the rates of renal replacement therapy (14.3% vs. 34.0%, P < 0.001), mechanical ventilation support (37.3% vs. 51.9%, P = 0.018), and vasopressor use (9.9% vs. 18.9%, P = 0.037) of the DDLT group were significantly higher. The proportion of patients with HEP grades III or IV was significantly higher in the DDLT group than in the LDLT group (34.8% vs. 61.3%, P < 0.001). Although not statistically significant, the proportion of patients with brain edema, as observed on brain CT images, was higher in the LDLT group than in the DDLT group (16.1% vs. 11.3%, P = 0.269). The mean durations from encephalopathy to transplantation of both groups were similar (5.9 ± 12.0 days vs. 8.4 ± 9.1 days, P = 0.091).
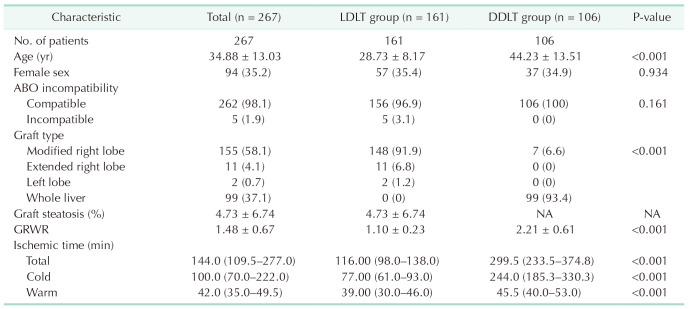
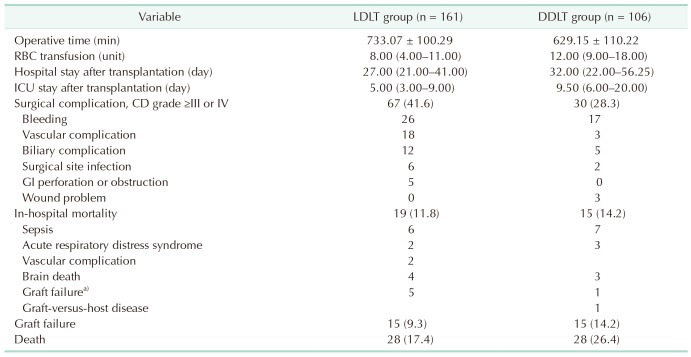
The donor characteristics are summarized in Table 2. As expected, the graft weight and graft-to-recipient weight ratio were lower in the LDLT group (1.1 ± 0.2 vs. 2.2 ± 0.61, P < 0.001). Furthermore, for patients in the LDLT group, the donor age was younger (28.7 ± 8.2 years vs. 44.2 ± 13.5 years, P < 0.001), the cold ischemic time was shorter (77 minutes vs. 224 minutes, P = 0.091), and the operative time was longer (733.1 minutes vs. 629.2 minutes, P < 0.001). The majority of LDLT recipients underwent transplantation with modified right lobe grafts (148 of 161, 91.9%). LDLT was associated with a higher incidence of surgical complications (41.6% vs. 28.3%, P = 0.009). The most common surgical complication in both groups was surgical site bleeding, followed by vascular complications. However, postoperatively, the mean ICU stay was shorter in the LDLT group (5.0 days vs. 9.5 days, P < 0.001). In addition, the in-hospital mortality rate of the DDLT group was higher than that of the LDLT group; however, the difference was not statistically significant (11.8% vs. 14.2%, P = 0.435). The causes of in-hospital mortality included sepsis, brain death, graft failure, acute respiratory distress syndrome, surgical complications, and graft-versus-host disease. All donors were followed up for a minimum of 2 years after donation. During this period, donor death and liver failure requiring transplantation did not occur (Table 3).
Long-term survival after liver transplantation for acute liver failure
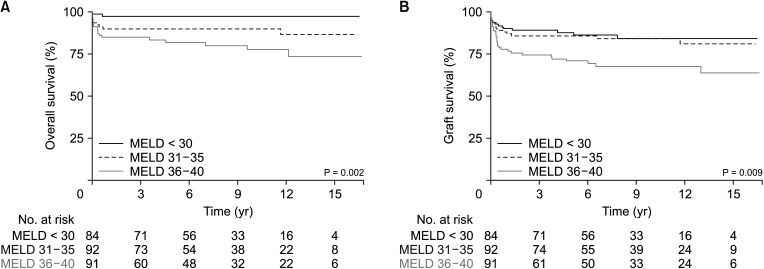
Among the 267 recipients who underwent LT for ALF, both graft survival and patient survival were significantly lower for those with higher MELD scores. The 1-year patient survival rates were 97.5% for recipients with MELD scores <30, 90.0% for recipients with MELD scores ≥30 but <35, and 85.0% for recipients with MELD scores ≥35 (P = 0.022) (Fig. 2). However, the 1-year graft survival rates were 90.4% for recipients with MELD scores <30, 88.0% for recipients with MELD scores ≥30 but <35, and 78.0% for recipients with MELD scores ≥35 (P = 0.05) (Fig. 2).
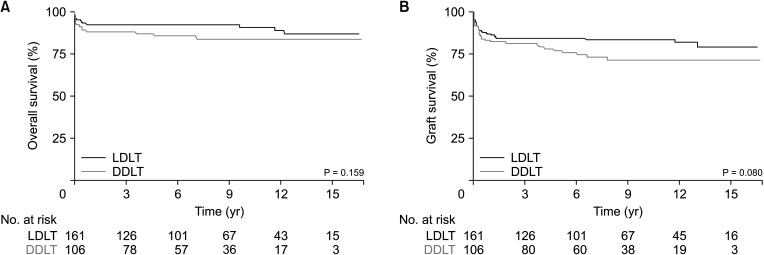
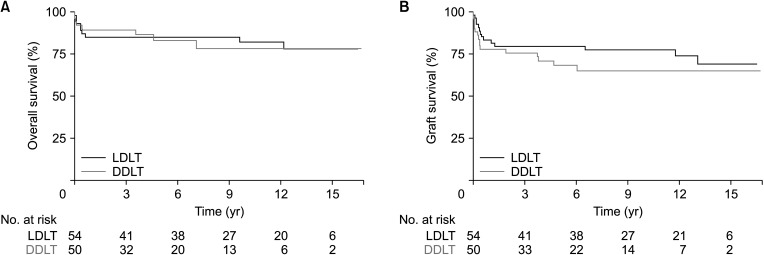
Among the 161 adults who underwent LDLT for ALF, the patient survival and graft survival rates were not inferior to those of patients who underwent DDLT (P = 0.159 and P = 0.080, respectively). The patient survival rates of the LDLT and DDLT groups at 1, 5, 10, and 15 years were 92.2%, 92.2%, 90.8%, and 86.8%, respectively, and 88.2%, 85.8%, 84.0%, and 84.0% respectively; however, the graft survival rates of the LDLT and DDLT groups at 1, 5, 10, and 15 years were 86.9%, 84.4%, 83.5%, and 79.3%, respectively, and 83.0%, 76.7%, 71.3%, and 71.3%, respectively (Fig. 3). A subgroup analysis of patient survival and graft survival rates of recipients with MELD scores ≥35 and <35 showed similar results for those in the LDLT and DDLT groups (P = 0.877 and P = 0.285, respectively) (Fig. 4).
Risk factors for in-hospital mortality after liver transplantation for acute liver failure
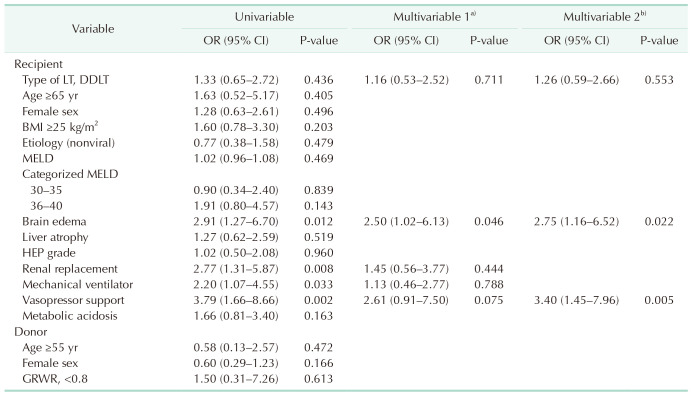
The results of the univariable and multivariable analyses of in-hospital mortality are presented in Table 4. The univariable analysis identified persistent brain edema (OR, 2.91; 95% CI, 1.27–6.70; P = 0.012), renal replacement therapy (OR, 2.77; 95% CI, 1.31–5.87; P = 0.008), mechanical ventilation (OR, 2.20; 95% CI, 1.07–4.55; P = 0.033), and vasopressor use (OR, 3.79; 95% CI, 1.16–8.66; P = 0.022) at the time of transplantation as significant predictors of in-hospital mortality after LT for ALF. According to the multivariable logistic regression analysis, factors that were significantly associated with in-hospital mortality included vasopressor use (OR, 3.40; 95% CI, 1.45–7.96; P = 0.005) and brain edema (OR, 2.75; 95% CI, 1.16–6.52; P = 0.022) at the time of transplantation. Living donor status was not independently associated with in-hospital mortality (P = 0.553).
DISCUSSION
We demonstrated that LDLT for patients with ALF can result in satisfactory short-term and long-term survival outcomes comparable to those achieved with DDLT. Notably, even for recipients with ALF with severe illness and high MELD scores, LDLT resulted in 10-year patient survival and graft survival rates of 90.8% and 83.5%, respectively. This finding surpasses those of previous studies [791015]. Additionally, this study showed that LDLT is technically more complex and associated with a higher incidence of major complications compared to that of DDLT; furthermore, the postoperative graft function and in-hospital mortality rates of the LDLT group were similar to those of the DDLT group. Therefore, if a living donor is available, it is advisable to perform LDLT in a timely manner.
LT is the only treatment that has been proven to significantly enhance the survival rates of patients with irreversible ALF [216]. Before the availability of emergency LT, the survival rates ranged from 15% to 20%; however, with advancements in perioperative care, these rates have increased to 60%–80% [2171819]. However, although LT can save lives, it is also associated with long-term morbidity and mortality. Thus, the accurate identification of patients who require transplantation and those who can recover spontaneously without LT is critical; furthermore, it is important to determine the most suitable timing for LT to prevent disqualification caused by deteriorating conditions.
Various selection criteria, such as the King–s College and Clichy criteria for LT with ALF, are used worldwide; however, there is ongoing debate regarding their accuracy and usability [2021]. Alternative or supplementary prognostic indicators have been proposed to address the limitations of these established criteria and more accurately and rapidly identify patients who require transplantation [17]. These indicators include single laboratory values, such as elevated serum ammonia, serum lactate, and arterial phosphate levels, PT/INR, reduced platelet counts, reduced levels of procoagulant factors V and VII, liver volume shrinkage to less than 1,000 cm3, and liver biopsy results indicating the presence of hepatic necrosis [2417]. Numerous prognostic scoring models have been suggested; unfortunately, these models demonstrate variable reliability and predictive precision, thus, restricting their usefulness in clinical settings [18]. Recently, a predictive model of 21-day transplant-free survival of patients with ALF that included data from the Acute Liver Failure Study Group was introduced [22]. This model incorporated data regarding the HEP grade, ALF etiology, vasopressor use, and logarithmic transformations of the bilirubin level and PT/INR during the initial stage of hospitalization. Although this study confirmed that this model is superior to the King’s College criteria and MELD score for predicting ALF transplant-free survival, additional validation studies are necessary.
At our institution, the decision to perform LT is made based on a range of prognostic factors identified through a multidisciplinary approach. Identical criteria are used for both DDLT and LDLT for patients with ALF. All patients with ALF and HEP were initially considered candidates for DDLT. The Korean allocation system prioritizes the selection of patients with ALF. DDLT is prioritized for patients with ALF and significant HEP (grade III or higher) within 8 weeks of the onset of liver disease symptoms who do not have a history of chronic liver disease and are currently receiving intensive care. This priority was based on the fulfillment of one or more of the following criteria on the day of waitlisting: mechanical ventilation use, renal replacement therapy use, or PT/INR >2.0. However, the limited availability of deceased donors often results in delays in transplantation, thus, leading to death among patients awaiting DDLT. These deaths are primarily caused by clinical deterioration resulting from complications such as sepsis, hemodynamic instability, multiorgan failure, and irreversible neurological impairment, which are typical of the progression of ALF [2324]. Our primary clinical determinant of transplantation timing was HEP severity. For patients with progressive HEP and cerebral edema, prompt confirmation of the availability of living donors is essential. When a suitable living donor is identified, LDLT is preferred to avoid risks associated with waiting for a deceased donor, thereby preventing irreversible neurological damage. This approach of selecting LDLT candidates likely resulted in the high incidence of cerebral edema in the LDLT group observed during this study. Additionally, even in the absence of cerebral edema and rapid progression of HEP accompanied by the rapid decline of liver function indices, the evaluation of a living donor for LDLT is recommended when patients do not meet the Korean Network for Organ Sharing criteria for the prioritization of DDLT.
Better survival outcomes associated with LDLT can be expected when transplantation is performed at an optimal time. This optimal timing is facilitated by the availability of grafts from living donors when recipients are experiencing critical disease stages. Our results also confirmed that despite the prioritized allocation of deceased donor liver grafts to patients with ALF, liver grafts from living donors enabled transplantation within a shorter time from the date of symptom onset. This factor also influenced the severity of the patient’s condition at the time of LT, thus leading to the observation that the LDLT group, who underwent transplantation at a time of lower severity, had better survival outcomes. Contrary to the early perceptions of LDLT’s inferior efficacy for ALF, several recent studies have suggested that there is no significant difference in survival outcomes between DDLT and LDLT [79252627]. The survival benefit of LDLT, especially when DDLT cannot be performed in a timely manner, is gradually expanding the indications for LDLT. Satisfactory results of LDLT using ABO-incompatible grafts have been reported as well [282930].
To our knowledge, this is the largest single-center study of LDLT for ALF. Comprehensive follow-up of survivors was performed for more than 15 years, which is a significant strength of this study. However, this study had some limitations. First, because this was a retrospective study, our analysis relied heavily on the completeness of the medical records. Second, this study was conducted at a single center in Asia. However, the etiology of ALF in Asia differs from that in Western countries. Moreover, this study was conducted at a center with a major LDLT program where more than 400 LDLTs are performed annually; therefore, these outcomes may not be applicable to all centers worldwide. Third, the extensive study duration (15 years) may have led to historical bias caused by substantial advancements in perioperative assessments, surgical methods, and perioperative care during the study period. Finally, the selection criteria for LDLT or DDLT were distinctly different, thus, rendering the comparison of the 2 groups less significant and impracticable.
This study demonstrated excellent outcomes, with 1-year patient survival and graft survival rates of 92.2% and 86.9%, respectively, for LDLT for adult patients with ALF, and used a standardized protocol for patient selection and donor selection, surgical techniques, and perioperative multidisciplinary care. Therefore, although LDLT is both procedurally and technically more complex than DDLT, it is significantly clinically valuable when deceased donors are unavailable. This study showed that LDLT is a feasible treatment option for patients with ALF, even when high-grade HEP is accompanied by brain edema, that can be performed as an alternative to DDLT. However, this study identified brain edema as an independent predictor of in-hospital mortality after LT. Consequently, when a living donor is available, prompt LDLT that is performed before brain edema development can positively affect patient survival.
 XML Download
XML Download