

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical neck metastases in papillary thyroid carcinoma (PTC) are quite common [12] and are associated with increased locoregional recurrence (LRR) [34567]. However, PTC has a relatively good prognosis compared to other types of thyroid cancers [8]. For this reason, local recurrence and postoperative quality of life remain important issues. The 2015 American Thyroid Association (ATA) guidelines for thyroid cancer management recommend that prophylactic central neck dissection (CND) should be considered in clinically involved lateral neck nodes [9], but there is no detailed description for the extent of CND (ipsilateral or contralateral compartment), and the extent of prophylactic CND depends on surgeon’s discretion. To date, only a few studies are about the contralateral central compartment in PTC patients with unilateral lateral neck metastasis (LNM). Some studies have been conducted to examine contralateral central neck metastasis (CNM) status and its risk factors but without actual long-term prognosis with regard to the extent of CND [610]. It is clinically significant to clarify long-term outcome according to the extent of CND in PTC patients with unilateral LNM because it is obvious that the incidence of surgery-related morbidities, such as hypoparathyroidism or hypocalcemia or vocal cord palsy, were observed more prominently in bilateral CND rather than unilateral CND [1112131415]. The purpose of this study was to compare the recurrence rate between unilateral CND group and bilateral CND group in patients who underwent unilateral modified radical neck dissection (MRND). This, in turn, could potentially decrease postoperative morbidities from unnecessary neck dissection.
Go to : 
METHODS
This research design received approval from Institutional Review Board of Samsung Medical Center (No. 2024-05-129). This study was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature.
Patient selection
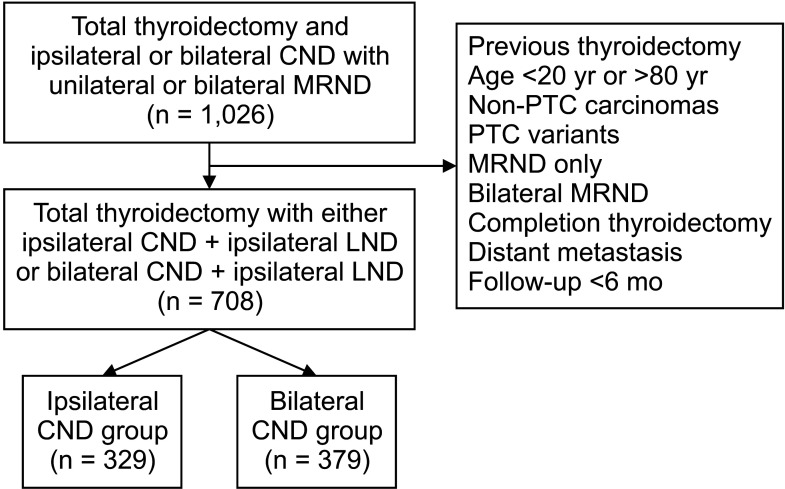
We conducted a retrospective study at a single institution between January 1997 and December 2022. A total of 1,026 patients underwent unilateral MRND with concomitant total thyroidectomy at Samsung Medical Center. Patients with the following were excluded: preoperative contralateral clinically apparent nodal disease (cN1a) patients, a history of previous thyroidectomy, an age younger than 20 years or older than 80 years, non-PTC carcinomas (follicular/medullary/anaplastic), PTC variants, mixed type PTC, MRND without thyroidectomy due to lateral neck recurrence, completion thyroidectomy, bilateral MRND, distant metastasis, and follow-up duration less than 6 months [16]. Finally, a total of 708 PTC patients who underwent total thyroidectomy with either ipsilateral CND + unilateral MRND or bilateral CND + unilateral MRND were enrolled (Fig. 1).
All patients were examined by ultrasonography (US) and/or CT preoperatively to evaluate primary tumor and the presence of suspected nodal metastases [16]. Korean Thyroid Imaging Reporting and Data System was used for US-based diagnosis [16]. Suspicious lesions were diagnosed by fine needle aspiration (FNA). Suspicious lymph nodes in the lateral compartment were confirmed by FNA or washing thyroglobulin (Tg) measurement or both. We characterized clinically involved central lymph node disease (cN1a) as suspicious central lymph node (CLN) metastases observed on preoperative imaging [16].
Surgical methods
Surgical strategies were chosen based on the ATA guidelines [9]. All patients underwent total thyroidectomy with either unilateral CND or bilateral CND + unilateral MRND. Therapeutic unilateral CND was typically performed after suspicious unilateral CNM was detected preoperatively in US or during surgery. Since all patients were without contralateral CNM by preoperative exams in this study, prophylactic contralateral CND was performed at the discretion of the surgeon. The term “unilateral” was employed to denote the side where the main tumor was located, while “contralateral” was defined as the side opposite to the main tumor. In cases of bilateral tumors, the largest tumor was considered to be the main tumor. Unilateral CLNs included unilateral paratracheal, pretracheal lymph nodes, and precricoid (Delphian) nodes. MRND was defined as a neck dissection of levels II–V, preserving the internal jugular vein, spinal accessory nerve, and sternocleidomastoid muscle [16].
Histopathological examination of surgical specimens
Surgical specimens were examined by 2 or more experienced pathologists. Histopathologic factors including main tumor size (longest diameter of the largest lesion), cell type of main tumor, multifocality, bilaterality, microscopic or gross extrathyroidal extension (ETE), central or lateral lymph node (LLN) metastasis, and underlying conditions of the thyroid were assessed [16]. Multiplicity was defined as multiple PTCs in one lobe. Thyroid cancer staging was determined following guidelines outlined in the article of Edge and Compton [17].
Surgery-related outcomes
The terms “transient” and “permanent” were defined on a 6-month basis. “Transient” was defined as a duration of less than 6 months and “permanent” was defined as a duration of more than 6 months. Hypocalcemia was defined as a serum calcium <8.0 mg/dL. Calcium level was the lowest value within or more than 6 months of surgery accordingly. Recurrent laryngeal nerve injury described as vocal cord palsy was diagnosed by laryngoscopy. Postoperative serum Tg level in Table 1 was defined as the stimulated Tg after the first ablation.
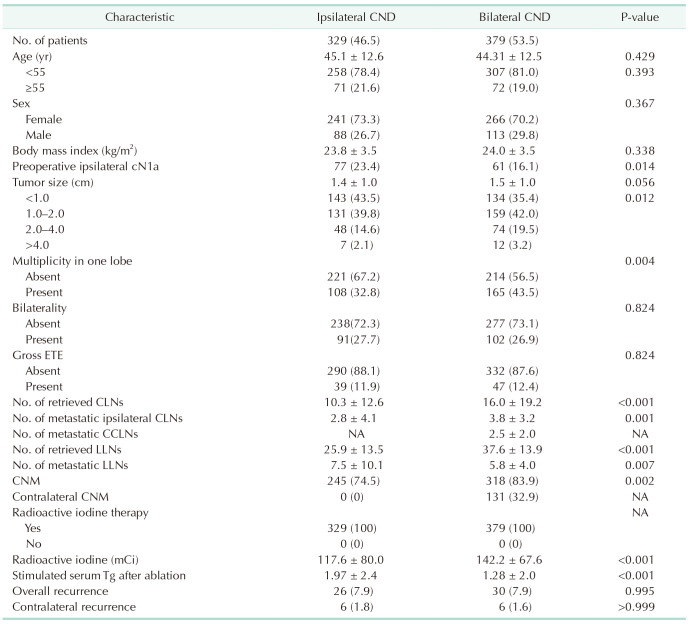
Table 1
Clinicopathological characteristics of 708 PTC patients who underwent total thyroidectomy with either ipsilateral CND + ipsilateral LND or bilateral CND + ipsilateral LND
Values are presented as number (%) or mean ± standard deviation.
PTC, papillary thyroid carcinoma; CND, central neck dissection; LND, lateral neck dissection; ETE, extrathyroidal extension; CLN, central lymph node; CCLN, contralateral central lymph node; NA, not available; LLN, lateral lymph node; CNM, central neck metastasis; Tg, thyroglobulin.
![]()
Postoperative follow-up and management
After the initial surgery, all patients underwent regular follow-up at 6- to 12-month intervals with clinical evaluations including physical examinations, US, CT, iodine-131 (131I) scans, and serum unstimulated Tg level. Lesions suspicious for recurrence were verified through US-guided FNA with or without washing Tg measurement and/or CT or PET. We defined LRR as the presence of tumors or metastatic lymph nodes on cytology from FNA. Radioactive iodine (RAI) therapy was performed with 131I at 4–12 weeks after surgery according to the ATA guidelines [9]. In this study, all patients received postoperative RAI therapy, and thyroid-stimulating hormone suppression was performed according to the ATA guidelines [9].
Statistical analysis
Statistical analyses were conducted utilizing IBM SPSS Statistics ver. 28.0 (IBM Corp.). The chi-square test and Student t-test were used for categorical variables and continuous variables, accordingly. Statistical differences were considered as P-values less than 0.05. Propensity score matching was performed to adjust clinicopathological variables which can effect on recurrence. Under the matched condition, the Kaplan-Meier and the log-rank test were adopted to analyze time-dependent LRR.
Go to :
RESULTS
Clinicopathological characteristics of 708 N1b patients who underwent total thyroidectomy with either ipsilateral or bilateral central neck dissection
The mean patient age was 44.7 years (range, 20–77 years) and the mean tumor size was 1.5 cm (range, 0.1–8.0 cm). Of the 708 patients, 329 (46.5%) underwent ipsilateral CND and 379 (53.5%) underwent bilateral CND. In the bilateral CND group of 379 patients, contralateral CNM occurred in 131 patients (34.6%). Of the 33 patients with tumor encroaching on isthmus, there were 23 patients (69.7%) who underwent bilateral CND; 13 (39.4%) had contralateral CNM and 10 (30.3%) had no contralateral CNM. The final 10 patients (30.3%) with tumor encroaching on isthmus were in the ipsilateral CND group. Most patients in the whole cohort received RAI treatment except for the 19 patients (5.8%) in the ipsilateral CND group.
A comparison of the 2 groups showed that preoperative ipsilateral cN1a (P = 0.014), tumor multiplicity in a single lobe (P = 0.004), a number of retrieved CLNs (P < 0.001), number of metastatic ipsilateral CLNs (P = 0.001), a number of retrieved LLN (P < 0.001), a number of metastatic LLNs (P = 0.007), ipsilateral CNM (P = 0.002), RAI treatment status (P < 0.001), RAI dose difference (P < 0.001), and postoperative stimulated Tg level (P < 0.001) were significantly different (Table 1). Recurrence (P = 0.995) and contralateral recurrence (P > 0.999) were not statistically different between the 2 groups. LRR was observed in 26 patients (7.9%) in the ipsilateral CND group and 30 patients (7.9%) in the bilateral CND group. Contralateral recurrence occurred in 12 patients in the whole cohort; there were 6 contralateral recurrence cases (1.8%) in the ipsilateral CND group and 6 cases (1.6%) in the bilateral CND group (Table 1).
Recurrence sites for 65 recurred patients
There were 65 recurred patients (9.2%) in the whole population. Among 23 patients with LRR (7.0%) in the ipsilateral CND group, recurrence was detected at the ipsilateral thyroidectomy site in 5 patients (1.5%), ipsilateral central neck in 1 patient (0.3%), ipsilateral lateral neck in 10 patients (3.0%), and ipsilateral central neck + lateral neck in 1 patient (0.3%). Contralateral recurrence occurred in 6 patients overall: 2 cases (0.6%) in the contralateral thyroidectomy site, 1 case (0.3%) in the contralateral central neck, 3 cases (0.9%) in the contralateral lateral neck (Table 2).
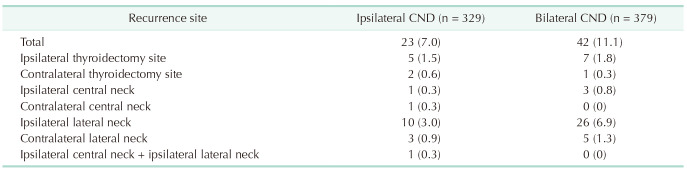
In the bilateral CND group, there were 42 patients (11.1%) with LRR. Recurrence occurred at the ipsilateral thyroidectomy site in 7 patients (1.9%), ipsilateral central neck in 3 patients (0.8%), and ipsilateral lateral neck in 26 patients (6.8%). Contralateral recurrence occurred in 6 patients overall; there were 1 case (0.3%) in the contralateral thyroidectomy site, 5 cases (1.3%) in the contralateral lateral neck. There was only one contralateral central neck recurrence in the ipsilateral CND group (Table 2).
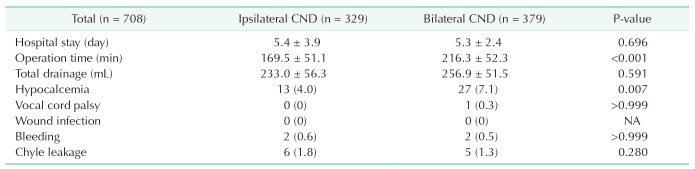
Surgery-related outcomes in 708 papillary thyroid cancer patients according to contralateral central neck dissection status
The incidence of hypocalcemia (4.0% vs. 7.1%, P = 0.007) was significantly higher in the bilateral CND group and operation time (169.5 minutes vs. 216.3 minutes, P < 0.001) were longer in the bilateral CND group compared to the ipsilateral CND group (Table 3).
Go to :
DISCUSSION
Previous studies have reported that the rate of regional lymph node metastasis in patients with PTC is approximately 30% up to 80% [1819] and the rate of contralateral CNM in patients with ipsilateral LNM was 34.7% and 5% to 30% in the final pathology [2021]. Since these rates were relatively high, there has been a controversy as to whether or not surgeons should perform contralateral CND without suspicious contralateral CLNs on preoperative imaging. To our knowledge, this study is one of the unique studies exploring the long-term outcome of prophylactic contralateral CND in PTC patients with ipsilateral LNM.
In our study, ipsilateral CND only did not increase the risk of recurrence (Tables 1, 2). In the ipsilateral CND group, the rate of recurrence in the ipsilateral compartment was higher than those in the contralateral compartment. There was no significant difference in recurrence regarding CND status with either the ipsilateral or bilateral sides (Table 2).
The point is, recurrence is more likely to occur in the ipsilateral neck, not in the contralateral compartment in this whole study population (Table 2). A previous study demonstrated that male sex, larger tumor size, ETE, and gross nodal metastasis were associated factors for contralateral lateral neck recurrence [22]. However, contralateral neck recurrence rarely occurred so it was difficult to analyze risk factors for contralateral recurrence in our study.
Furthermore, we found that ipsilateral CND only was not associated with a higher risk of either overall recurrence or contralateral recurrence. Interestingly, there was only one recurrence in the contralateral central neck among the whole study population. LRR occurred mostly in the ipsilateral compartment.
The greater number of metastatic ipsilateral lymph nodes were observed when bilateral CND was performed. In our study, ipsilateral CND can be either therapeutic or prophylactic purpose. Based on our data, we found that the number of patients with preoperatively ipsilateral clinical N1a was 136. cN1a patients are more likely to undergo bilateral CND at surgeon’s discretion so that it may lead to such result. Also, this result means that majority of CNM was microscopic metastasis. Previous studies concluded that microscopic node metastasis occurs frequently, but it does not give rise to the higher recurrence risk seen in clinically detectable macroscopic disease and recurrence rates ranged from 2% to 6% [2324]. Our study showed that microscopic CNM was present in 79.5% of patients, the prevalence of contralateral CNM was 32.9% (131 of 397), and the recurrence rate was 9.2%. Hughes et al. [24] concluded that there was no significant difference in postoperative Tg level between the thyroidectomy alone group and prophylactic CND group in pathologic N1a patients who presented clinically no lymph node metastasis (cN0) preoperatively. Our data showed that Tg was higher in the ipsilateral CND group than in the bilateral CND group with no difference in overall recurrence.
Postoperative complications such as hypocalcemia were higher in patients who underwent bilateral CND than those who underwent ipsilateral CND (Table 3). This is a critical issue in thyroid surgery because hypocalcemia is closely associated with the patients’ quality of life, and all endocrine surgeons should not ignore it.
Given the results above, we recommend that only PTC patients with evident lymphadenopathy intraoperatively or contralateral N1b on preoperative imaging should undergo therapeutic contralateral CND. Otherwise, ipsilateral CND may be sufficient treatment of the PTC patients with ipsilateral LNM.
This study had several limitations. Our study was a non-randomized, retrospective, cohort study. Confounding variables or unmeasured factors may not have been identified. Further prospective, randomized trials are needed to resolve this selection bias issue. Additionally, there exists inter-observer variability in the identification and interpretation of cervical lymph node metastasis.
Bilateral CND increased surgery-related complications, especially hypocalcemia, and did not reduce the risk of recurrence in PTC patients with unilateral N1b; therefore, surgeons may perform contralateral CND only in the presence of evident nodal disease on the contralateral neck. Prophylactic contralateral CND may be skipped in specific situations where you have to focus on preserving function of contralateral recurrent laryngeal nerve or worry about postoperative hypoparathyroidism.
Go to :
 XML Download
XML Download