

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Preterm birth is the most important determinant of poor neonatal outcomes, and prevention is a major issue in obstetric care. Tocolytics have been recommended to delay preterm births and save time to use antenatal corticosteroids for fetal lung maturation.1234 Although tocolytic use is generally limited to several days, maintenance tocolysis is used in many clinical situations reality.56789 Whether it is used in the short- or long-term, adverse effect profiles should be considered when they are used in women with pregnancy complications, such as gestational diabetes mellitus (GDM).
There are several types of tocolytics, including beta-agonists, calcium channel blockers, and oxytocin antagonists. Although beta-agonists have been used for a long time, they are associated with several maternal complications. In particular, its use increases the risk of diabetic ketoacidosis or maternal hyperglycemia in women with diabetes, which limits its use in women with diabetes.1011 Other tocolytics can be used in pregnancies with diabetes. Nifedipine, a calcium channel blocker, is considered effective and safe in inhibiting preterm labor in several studies.1213 However, there has been some evidence suggesting that calcium channel blockers may alter glucose homeostasis and have diabetogenic effects.1415 Atosiban, an oxytocin antagonist, has also been shown to be effective in inhibiting preterm labor.16 Studies have shown that atosiban does not increase the risk of complications, such as diabetic ketoacidosis or maternal hyperglycemia, compared to beta-agonists.1718 Thus, atosiban tocolytics have been recommended for diabetic women in preterm labor. However, there was a report that increased maternal and decreased neonatal glucose levels are associated with atosiban use.19 With this background, we felt the need to evaluate blood glucose levels in pregnant women with GDM who use these tocolytics for preterm labor.
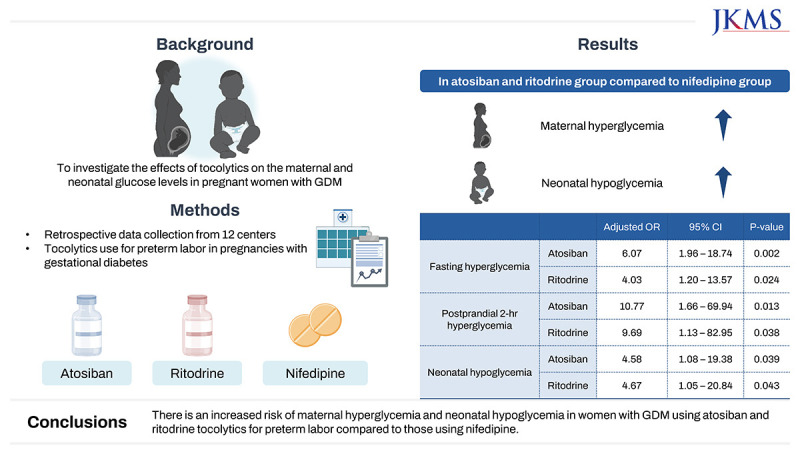
This study investigated the effects of tocolytics on maternal and neonatal glucose levels in pregnant women with GDM who used tocolytics for preterm labor.
METHODS
In this retrospective cohort study, we enrolled women with GDM who were admitted for preterm labor and were administered tocolytics, including atosiban, ritodrine, and nifedipine, between January 2011 and December 2020 at 12 hospitals in South Korea. Women with multiple pregnancies, fetal anomalies, overt DM diagnosed before pregnancy or at 23 weeks of gestation, and women who received multiple types of tocolytics simultaneously or in series were excluded.
Preterm labor was diagnosed based on the definition of regular uterine contractions accompanied by a change in cervical dilation, effacement, or both, or initial presentation with regular contractions and cervical dilation of at least 2 cm.20 Tocolytics were initiated at the responsible physician’s discretion. Ritodrine, atosiban, and nifedipine are currently used as first-line tocolytics in Korea. Ritodrine was administered intravenously in a dilute mixture with normal saline. The infusion rate was adjusted according to symptoms and adverse effects. Atosiban was administered intravenously at a loading dose of 6.75 mg, followed by infusion at a rate of 18 mg/hour for three hours and then 6 mg/hour for a total of 48 hours of one-cycle infusion. Nifedipine was administered orally and the doses were determined by the responsible physicians.
Between 24 and 28 weeks of gestation, GDM was usually diagnosed using a two-step process with diagnostic criteria proposed by Carpenter and Coustan.21 Some physicians used a one-step diagnostic process using a 75-g oral glucose challenge test with the thresholds proposed by International Association of Diabetes and Pregnancy Study Groups.22 Blood glucose level was monitored at least four times a day; one fasting blood glucose (FBG) and three postprandial blood glucose levels. Postprandial blood glucose levels were monitored at 1 hour (PPG1) or 2 hours (PPG2) after meals according to the physician’s preference. A mean FBG level > 95 mg/dL, mean PPG1 level > 140 mg/dL, and mean PPG2 level > 120 mg/dL during tocolytic use were considered suboptimal, and maternal hyperglycemia was defined as any suboptimal glucose control. Neonatal hypoglycemia was defined as the presence of neonatal hypoglycemia in the medical records, the presence of symptoms, or treatment with glucose infusion. Glucose level ≤ 47 mg/dL in the first 24 hours after birth was also considered hypoglycemia.23
Patients were divided according to the type of tocolytic used: atosiban, ritodrine, or nifedipine. Baseline maternal characteristics, pregnancy outcomes, maternal glucose levels during hospitalization, and neonatal glucose levels after birth were collected.
Maternal and neonatal glucose levels were the outcomes of interest. We compared the mean FBG, PPG1, and PPG2 levels between groups. The frequencies of maternal and neonatal hypoglycemia were also compared. Continuous variables were compared using ANOVA. Categorical variables were compared using the χ2 test or Fisher’s exact test, as appropriate. Multivariate logistic regression analysis was performed to evaluate the factors contributing to the occurrence of maternal hyperglycemia and neonatal hypoglycemia. A P value < 0.05 was considered significant. Statistical analysis was performed using SPSS (IBM Corp., Armonk, NY, USA) version 24.0.
RESULTS
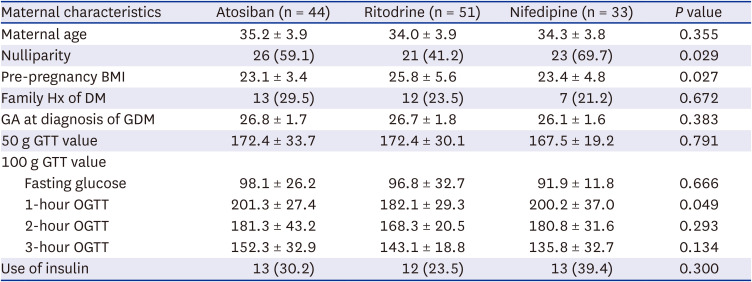
A total of 128 women were included; 44 (34.4%) received atosiban, 51 (39.8%) received ritodrine, and 33 (25.8%) received nifedipine. Among the baseline characteristics, the frequency of nulliparity was the lowest and the pre-pregnancy body mass index was the highest in the ritodrine group. The mean 1-hour oral glucose tolerance test (OGTT) result was lowest in the ritodrine group. Gestational age at GDM diagnosis, 50 g OGTT, 100 g OGTT values (except 1-hour OGTT results), and the frequency of insulin use were not different among the groups (Table 1).
Table 1
Comparison of maternal baseline characteristics according to the type of tocolytics
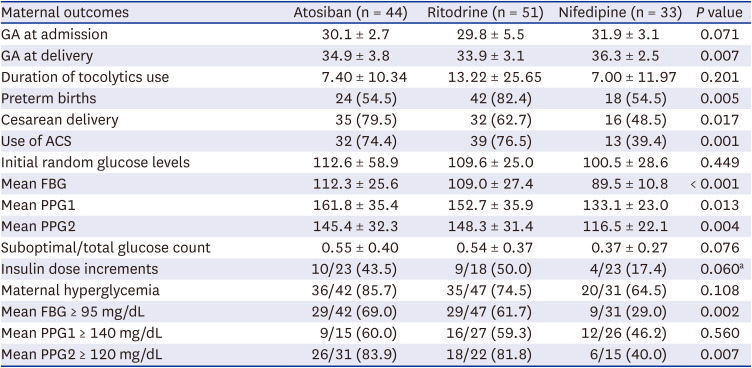
Gestational age at delivery was significantly lower in the ritodrine group. The duration of tocolytic use was not significantly different between groups. Preterm birth was more frequent in the ritodrine group as well. However, mean FBG, PPG1, and PPG2 levels were significantly higher in the atosiban and ritodrine groups than in the nifedipine group (Table 2). Insulin dose increment and the ratio of suboptimal glucose counts to total glucose counts were higher in the atosiban and ritodrine groups, but the difference was not statistically significant. The frequencies of fasting and PPG2 hyperglycemia were significantly higher in the atosiban and ritodrine groups. Maternal hyperglycemia showed a significant decreasing trend from atosiban to nifedipine (P = 0.036, linear-by-linear test). According to pairwise comparison, there were significant differences in mean FBG, PPG2, frequency of mean FBG ≥ 95 mg/dL, and mean PPG2 ≥ 120 mg/dL between ritodrine and nifedipine group and between atosiban and nifedipine group. Mean PPG1 levels differed between the atosiban and nifedipine groups. There was no difference in maternal glucose levels or neonatal hypoglycemia between the atosiban and ritodrine groups (P values not shown).
Table 2
Comparison of maternal outcomes and glucose levels during hospitalization for tocolysis according to the types of tocolytics
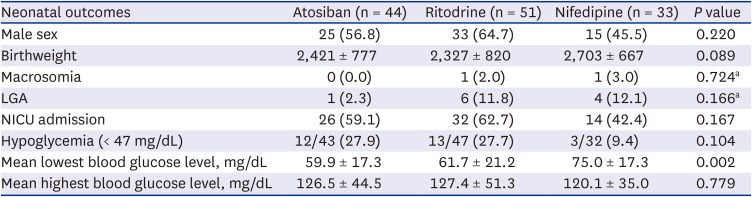
Regarding neonatal outcomes, birth weight, frequency of macrosomia, and gestational age were not different among the groups (Table 3). Neonatal hypoglycemia less than 47 mg/dL in the first 24 hours was not significantly different, but the mean lowest blood glucose levels were significantly lower in atosiban and ritodrine than nifedipine group (59.9, 61.7, and 75.0 mg/dL, respectively).
Table 3
Comparison of neonatal outcomes according to the tocolytics groups
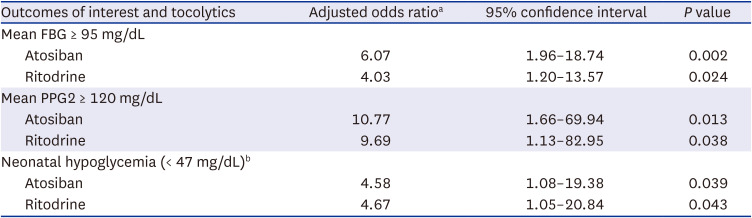
We calculated the risk of maternal hyperglycemia and neonatal hypoglycemia according to the tocolytic group using logistic regression (Table 4). After adjusting maternal antenatal steroid use, gestational age at admission, and pre-pregnancy body mass index, the risk for mean FBG ≥ 95 mg/dL and PPG2 ≥ 120 mg/dL were significantly increased in the atosiban and ritodrine group compared to nifedipine group. Neonatal hypoglycemia (< 47 mg/dL) was also significantly increased in the atosiban and ritodrine groups compared to the nifedipine group (odds ratio [95% confidence interval], 4.58 [1.08–19.38] for atosiban; 4.67 [1.05–20.84] for ritodrine group) after adjusting for covariates.
Table 4
The risks of maternal fasting and postprandial hyperglycemia and neonatal hypoglycemia associated with ritodrine and atosiban compared to nifedipine group using logistic regression
DISCUSSION
When the three types of tocolytics were used for preterm labor in women with gestational diabetes, the mean FPG, PPG1, and PPG2 levels were higher in the atosiban and ritodrine groups than in the nifedipine group. The frequency of maternal fasting (mean FBG ≥ 95 mg/dL) and 2-hour postprandial (mean PPG2 ≥ 120 mg/dL) hyperglycemia were also significantly higher in the atosiban and ritodrine group, which remained significant after adjusting for covariates. We also found that tocolytic use affected neonatal glucose levels, as evidenced by the difference in the mean lowest blood glucose values in neonates.
The severity and duration of tocolytic use may influence maternal glucose levels. For all three groups, the frequency of insulin use, fasting glucose, 2-hour OGTT, and 3-hour OGTT were not different between groups. The average value of the 1-hour OGTT was low in the ritodrine group. In addition, the duration of tocolytic use was not significantly different among the three groups. Although the mean duration of tocolytic use was longer in the ritodrine group, this difference was not statistically significant. Therefore, considering that patients in the atosiban and ritodrine groups did not have more severe disease than those in the nifedipine group in terms of insulin use, OGTT results, and duration of tocolytic use, it is unlikely that GDM severity influenced the results.
The findings of maternal hyperglycemia and decreased neonatal glucose levels in the atosiban group were unexpected. Most of the previous clinical trials indicated that the frequency of maternal hyperglycemia was lower in women using atosiban compared to those in women with beta-agonists.172425 There was a trial where maternal hyperglycemia was more frequent in the atosiban group26 and another trial reported similar occurrence.18 They did not make a comment about why those results happened. This is probably because maternal hyperglycemia was not the primary outcome, and they might have thought that it could have occurred by chance. There were no differences in the occurrence of neonatal hypoglycemia between these groups.172425 One study reported the side effects of maternal hyperglycemia while comparing the tocolytic effects of atosiban and nifedipine.27 In that study, there were insignificant changes in blood sugar 24 hours after the initiation of therapy. The reason why the results of our study are different from those of other studies is not clear, but the treatment duration might have caused the difference because our study included cases with both initial and maintenance tocolysis. Our results can be considered when choosing tocolytics for women with GDM, particularly for maintenance tocolysis.
Reportedly, the relationship between oxytocin and diabetes. In experimental research on mice, acute administration of oxytocin increased insulin secretion, and antagonism of oxytocin receptors by atosiban impaired insulin secretion and induced GDM in gestating but not non-gestating mice.28 They also showed that blood oxytocin levels were lower in patients with GDM than in healthy pregnant women and were associated with impaired beta-cell function. They suggested that oxytocin is needed for beta cell adaptation and the maintenance of beta cell function throughout pregnancy. The lack of oxytocin or the presence of oxytocin antagonists may be associated with the risk of GDM.
This study is unique in that it examined the blood glucose levels in pregnant women with GDM treated with various tocolytics, especially atosiban. Based on our data, researchers should pay attention to maternal and neonatal glucose levels when designing studies using oxytocin analogs. The limitations of this study include the retrospective nature of the study design and the lack of uniform utilization of the diagnostic criteria for GDM. As the data were gathered from multiple centers, the use of tocolytics may have been different. In addition, we did not have information about the timing of steroid and tocolytic administration, which might have affected maternal and neonatal glucose levels. Lastly, although the odds ratios in Table 4 are quite large, readers should be reminded that the 95% confidence intervals are wide, and the actual risks can differ.
In conclusion, the risk of maternal hyperglycemia or neonatal hypoglycemia in women with GDM who used tocolytics for preterm labor was higher with atosiban and ritodrine than with nifedipine. This should be recognized by physicians and counseled by patients when selecting the appropriate tocolytics.
 XML Download
XML Download