

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intracranial germ cell tumors (iGCTs) are rare, heterogeneous brain tumors that primarily arise in the pineal and suprasellar regions [12]. They account for about 10% of pediatric primary brain tumors in far East Asian countries [3]. iGCTs are germinomas and non-germinomatous germ cell tumors (NGGCTs), with the latter comprising teratomas categorized into mature and immature types. Frappaz et al. [4] established diagnostic criteria for iGCT based on clinical signs, radiology, markers in serum and cerebrospinal fluid, and histology.
Patients with NGGCTs show paradoxical growth of mature teratoma components after chemotherapy despite normalized tumor marker levels. Logothetis et al. [5] defined this phenomenon as growing teratoma syndrome (GTS). According to preceding studies, three criteria are required to diagnose: 1) normalization of tumor markers, such as alpha-fetoprotein (AFP) and/or beta-human chorionic gonadotropin (β-hCG), 2) rapid increase in tumor size during or after chemotherapy, and 3) absence of any NGGCT component in histopathology except mature teratoma [3]. Some researchers proposed that both chemotherapy and radiotherapy have to be included in definition of GTS [267]. GTS typically occurs in the gonad, retroperitoneum, or mediastinum [8]; however, it can manifest as intracranial GTS (iGTS). Michaiel et al. [6] reported that the incidence of iGTS is about 5% of all GCT patients due to a literature review from 2000 to 2017.
Here we report a rare case of iGTS one month after chemotherapy for pineal NGGCT.
Go to : 
CASE REPORT
A 22-year-old male patient complained of aggravating headaches and vomiting over the past few months. However, there was no specific illness in his past medical history. The initial contrast-enhanced brain MRI revealed a heterogeneously enhanced mass extending from the pineal gland to the fourth ventricle, causing obstructive hydrocephalus (Fig. 1A and B). A floating fatty droplet was also observed in the right lateral ventricle. The serum AFP level was elevated to 55.50 ng/mL, whereas the serum β-hCG level was within the normal range.
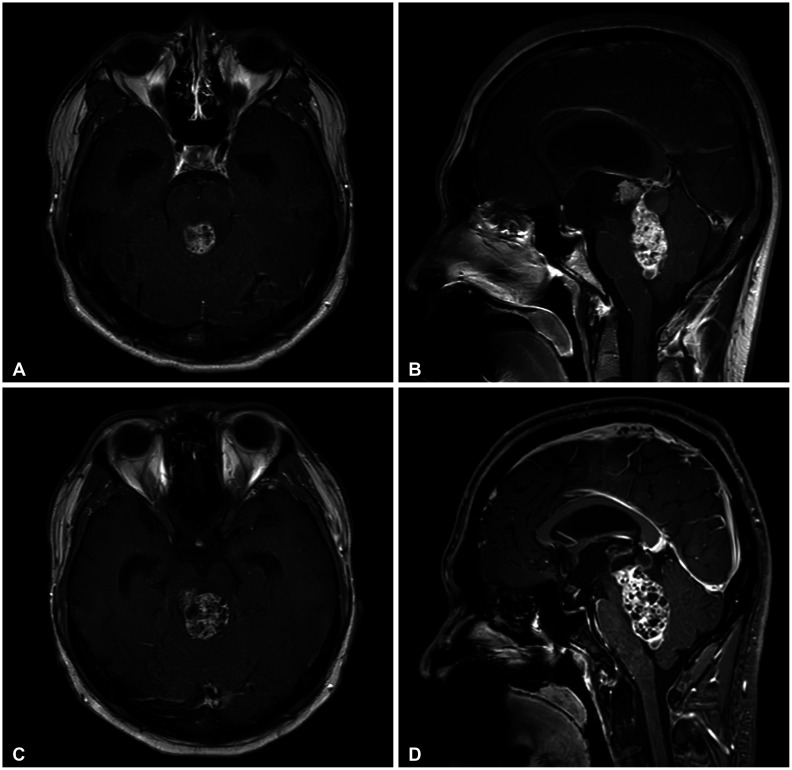 | Fig. 1Gadolinium-enhanced magnetic resonance (MR) brain images of intracranial growing teratoma syndrome (iGTS) patients. A and B: Initial MR images of germ cell tumor show heterogeneously enhanced mass obstructing the fourth ventricle. C and D: MR images after two cycles of chemotherapy show increased size of mass with honeycomb-like cystic patterns corresponding to iGTS.
|
We performed an endoscopic third ventriculostomy (ETV) with tumor biopsy and extraventricular drainage (EVD). There was no definitive sign of drop metastasis on the whole spine MRI. At first, the tumor was presumed to be an NGGCT; however, the biopsy specimen includes only an ependymal cyst-like component (Fig. 2A). According to the follow-up tumor marker results, the AFP level further increased to 76.52 ng/mL, and the β-hCG level rose to 9.35 ng/mL. Based on these findings, the tumor was diagnosed as a mixed germ cell tumor. Consequently, he was transferred to the oncology department to initiate adjuvant chemotherapy. The regimen included etoposide, cisplatin, and bleomycin. Serum AFP and β-hCG levels normalized after two cycles of chemotherapy. Meanwhile, he complained of aggravating symptoms, such as tinnitus, hearing loss, and diplopia. Subsequent brain MRI for response evaluation showed an increase in mass size with honeycomb-like cystic patterns (Fig. 1C and D). Therefore, we performed suboccipital craniotomy with subtotal tumor removal by infratentorial supracerebellar and telovelar approaches. The final pathologic findings showed different types of mature tissues such as chondroid tissue with columnar epithelium and cartilaginous tissue with respiratory epithelium, confirming the diagnosis of mature cystic teratoma (Fig. 2B and C).
 | Fig. 2Hematoxylin and eosin staining of the resected tumor. A: Tissue from ETV with biopsy shows only squamous epithelium containing keratin debris. B and C: Tissue from subtotal tumor resection shows typical mature cystic teratoma histopathology. It consists of different types of mature tissue components such as chondroid tissue (*) with columnar epithelium (**), cartilaginous tissue (black arrow), and respiratory epithelium (white arrow).
|
A postoperative hematoma was observed on the brain CT at the site where the mass had been located. While in an intensive care unit, the patient experienced drowsiness and quadriparesis, leading to a tracheostomy. Subsequent brain MRI revealed a left thalamic infarction. After several weeks of intensive care, the patient was successfully weaned off the ventilator and transferred to the general ward and then to the rehabilitation department. Currently, the patient can follow simple commands but is hospitalized for rehabilitation therapy and remains bedridden.
Go to :
DISCUSSION
The patient exhibited normalization of tumor marker after two cycles of chemotherapy, whether the tumor rapidly increased in size with a pathognomonic honeycomb-like cystic lesion and final pathologic diagnosis corresponding to mature teratoma. According to Tasaka et al. [9], the onset of iGTS usually occurs at a median time of 12.8 months, with a range from 3 to 56 months. Additionally, Michaiel et al. [6] report a median onset of 2 months, with a range of 0.5 to 32 months. In our case, it took only a month to confirm the diagnosis of iGTS. Therefore, while the onset of the current case is not exceptionally short, it is still relatively rapid compared to the ranges reported in the literature.
There was no definite consensus about the pathogenesis of iGTS, but a few hypotheses have been proposed. First, chemotherapy and/or radiotherapy may induce the immature proportion of tumor differentiation to a mature phenotype. Second, the selective destruction by chemo-radiation therapy, excluding mature teratoma, may lead to uninhibited growth of teratomatous element [1011]. Satake et al. [12] claimed that DMRT1 loss and 12p gain contribute to teratomagenesis in GTS by copy number variation analysis. In addition to genetic factors, certain microenvironments, such as unlimited benign cell growth, and an immune-compromised state due to chemotherapy may lead to the rapid growth of mature teratoma [3].
Referring to the pathological findings of our case, the rapid increase in the mass size is attributed to the formation of multiple cysts with exudate, not the growth of tumor cells themselves, which is consistent with previous studies. According to recent research, multiple cyst-like lesions usually comprise fatty components rather than pure cystic content, and the fatty component is more important [913].
Thus, the treatment of iGCT depends on tumor classification and clinical symptoms. The primary treatment option for NGGCT is neoadjuvant or adjuvant chemotherapy. Recently, radiotherapy has become significant; however, it is not recommended for teratomas. For germinoma, chemo-radiotherapy approaches are essential. If obstructive hydrocephalus is present at the initial diagnosis, ETV with optional biopsy or at least EVD is preferred. If residual mass persists after chemotherapy, a second-look operation is highly recommended for maximal safe resection [414]. Considering iGTS as an extension of the iGCT treatment, the ideal treatment for iGTS requires surgical approaches with gross total resection, if possible [361516]. For unresectable tumors due to their location, a clinical trial of palbociclib as adjuvant chemotherapy was undertaken [17].
Although iGCT patients showed favorable overall survival, early detection and early surgical intervention can mitigate deterioration. This is important since immature teratoma show faster growth even during chemotherapy and have a significantly higher incidence of iGTS, for example, 40%, as indicated in related literature [3]. In our case, the tumor was considered a mixed germ cell tumor containing an epidermal cyst-like component. The growing teratoma exhibited very rapid growth, causing symptoms that necessitated earlier imaging with a second-look operation.
iGTS rarely occurs during or after chemotherapy for iGCTs. iGTS presents with paradoxical growth of tumor mass containing mature teratomatous components, despite normalized tumor markers. The pathogenesis of iGTS is associated with the differentiation or destruction of immature components. Hence, several aspects require clarification. Surgery is a common and preferred treatment for iGTS, while ongoing clinical trials are exploring additional options. To improve prognosis, practitioners should remain vigilant for the possibility of iGTS and frequent imaging follow-ups.
Go to :
 XML Download
XML Download