

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Meningiomas are the most common primary intracranial tumor in adults, often remaining symptomless and slow-growing [1]. Even when they are symptomatic, approximately 90% are classified as World Health Organization (WHO) grade 1, exhibiting slow growth [2]. High-grade meningiomas, including WHO grades 2 (atypical) and 3 (anaplastic), constitute less than 10% of all meningiomas.
Meningiomas can recur even after a total resection [3], and approximately 29% of high-grade meningiomas arise from malignant transformation (i.e., dedifferentiation) of lower-grade meningiomas. Because of its rarity, the incidence and clinical features of the malignant transformation of benign meningiomas are poorly understood. Recent research on genetic alterations in meningiomas has identified potential therapeutic targets, such as inhibitors of mammalian target of rapamycin, focal adhesion kinase, cyclin-dependent kinase, phosphoinositide-3 kinase, sonic hedgehog signaling, and histone deacetylases. Nevertheless, the mechanisms behind this malignant transformation remain unclear.
Here, we report a 54-year-old male patient who underwent a stepwise malignant transformation of meningioma from grade 1 to grade 3 during 10 years of treatment, including five surgeries and multiple radiation therapies (RTs). There have been numerous case reports on stepwise malignant transformation of meningiomas so far [45]; however, this case report is unique in that we retrospectively examined the telomerase reverse transcriptase promoter (TERTp) mutation—one of the genetic mutations representing grade 3 meningioma—which revealed a c.-124C>T TERTp mutation from the initial grade 1 meningioma.
CASE REPORT
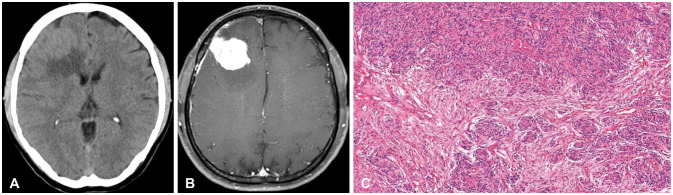
A 54-year-old male patient presented to the neuro-oncology clinic for further evaluation of a right frontal convexity mass with moderate peritumoral edema on outside brain CT (Fig. 1A). He suffered from gradual-onset headaches, intermittent dizziness, and vomiting that started 2 weeks before, though the neurological exam revealed no abnormalities. His brain MRI showed a lobulated, contoured, extra-axial, homogenously enhancing mass at the right frontal lobe and a dural tail suggestive of meningioma (Fig. 1B). Given the size of the mass and the symptoms presented, a surgical resection of the tumor was planned and conducted on January 16, 2013. A Simpson grade I resection was performed, and histopathology revealed a WHO grade 1 meningothelial-type meningioma (Fig. 1C). No unusual events occurred postoperatively. The patient was discharged and regularly followed with MRI at the outpatient clinic.
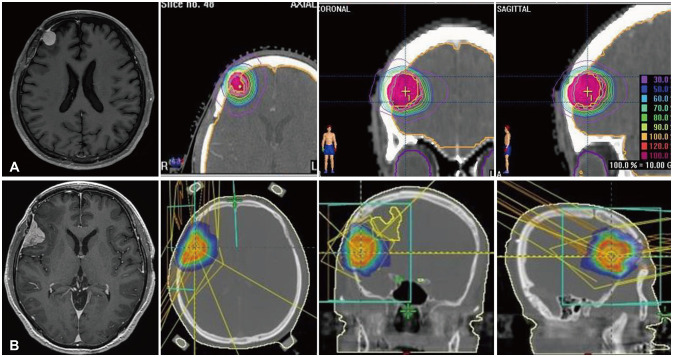
At the 2-year follow-up, MRI revealed a lobulated, contoured, enhancing, dural-based mass at the right middle frontal cerebral convexity, distant from the initial lesion, without any focal neurologic symptoms. Fractionated stereotactic radiotherapy (FSRT) of 3,000 cGy/3 fractions was performed in May 2015 for the recurrent lesion (Fig. 2A). MRI 1.5 years later showed a newly appeared right peri-Sylvian dural-based mass suggestive of recurrent meningioma, and stereotactic radiosurgery (SRS) with a 1,800-cGy marginal dose was delivered in March 2017 (Fig. 2B). Numerous intermittent seizure-like events were reported following SRS, and anti-epileptic drugs with dexamethasone were administered for the mildly aggravated post-RT perilesional edema. The right temporal lesion shrunk in size with progressive central necrosis, whereas the right frontal lesion seemed stationary.
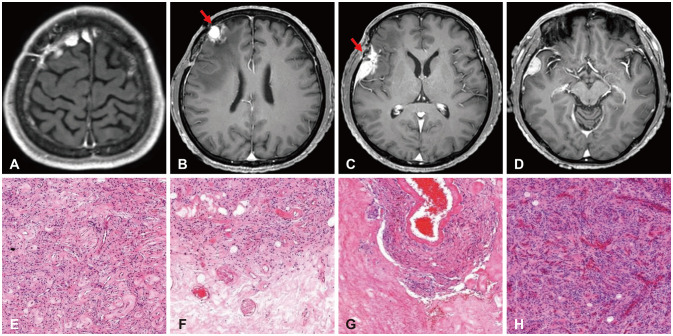
Two years after the last SRS, follow-up MRI revealed a newly formed high frontal midline lesion 8 mm in diameter (Fig. 3A) and a right temporal convexity meningioma 16 mm thick with peritumoral edema (Fig. 3D), along with the previously irradiated middle frontal and peri-Sylvian lesions (Fig. 3B and C, respectively). A second operation was conducted on June 27, 2019, and five lesions—including the above four and a falx lesion—were resected. Pathology revealed WHO grade 2 recurrent atypical meningioma with treatment-related changes in the irradiated middle frontal and peri-Sylvian lesions (Fig. 3E-H). The patient remained absent of neurologic deficits. At that time, a neurofibromatosis-2 (NF2) gene study was performed considering multiple distant recurrences but demonstrated no pathogenic or likely pathogenic variants. One year later, multiple recurrences were found at the frontal parasagittal area and right temporal pole, with a maximal diameter of 23 mm. A third operation was performed on December 3, 2020, for frontal parasagittal lesion Simpson grade II and temporal pole lesion Simpson grade I resection. The pathology results revealed WHO grade 2 atypical meningioma.
The 3-month follow-up MRI showed a newly appeared small (9 mm in diameter) residual, lobulated, dural-based, enhancing lesion at the surgical margin of the right frontotemporal area suggestive of a small residual meningioma. As SRS was not applicable for the right temporal lesion due to previous RT, the operation and radiotherapy were independently planned. On March 18, 2021, a fourth operation was performed on the right temporal lesion for gross total resection, and pathology revealed a WHO grade 2 atypical meningioma. Then, between March 2021 and May 2022, SRS (2,000 cGy) was performed on the right medial frontal base (olfactory groove) lesion, FSRT (4,500 cGy/10 fractions) was performed on the right high frontal dural thickening mass, and SRT (3,000 cGy/3 fractions) was performed on the right temporal lesion. Post-RT follow-up brain MRI showed that both the right high frontal mass and the temporal mass underwent central necrosis and reductions in size.
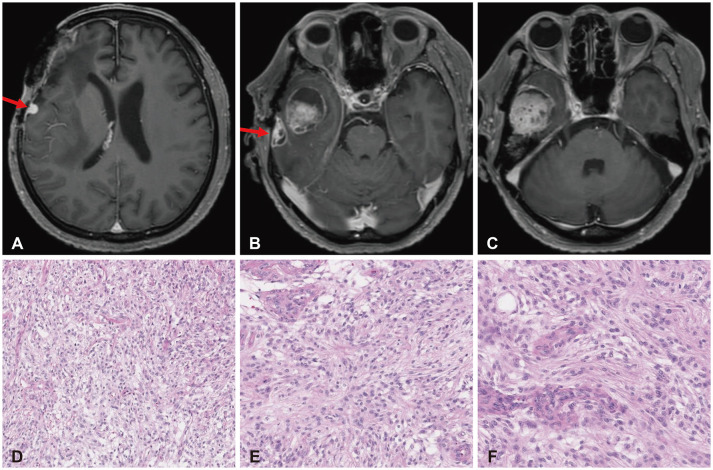
Over 8 months of serial follow-up, the right frontal parasagittal lesion reduced in size, a right frontal convexity mass 5 mm in diameter newly appeared (Fig. 4A), and the right temporal lesion grew from 8 to 14 mm and developed central necrosis (Fig. 4B). Moreover, a new right temporal base lesion appeared with partial cystic changes and a maximal diameter of 3.2 cm (Fig. 4C), necessitating a differential diagnosis of recurrent tumor and post-RT changes. A fifth operation for resection was performed on August 1, 2023, and histopathology revealed a WHO grade 3 anaplastic meningioma for the first time (Fig. 4D-F).
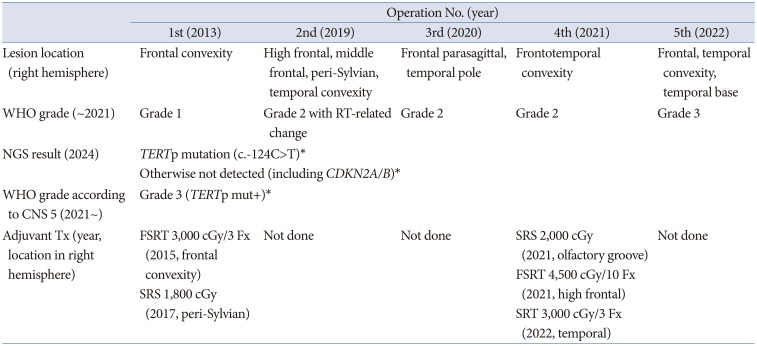
Next-generation sequencing (NGS) analysis was retrospectively conducted in January 2024 from formalin-fixed, paraffin-embedded (FFPE) specimens of the first, second, and fifth operations. The panel included 525 of the most common cancer-related genes, such as EGFR, BRCA, and PTEN, from comprehensive genomic database. The extracted DNA was fragmented using sonication before constructing the NGS library. Library preparation was performed using SureSelectXT Low Input Reagent Kits coupled with target enrichment (Agilent Technologies, Santa Clara, CA, USA). Customized probes were designed to capture the exonic regions of the 480 genes selected for the panel (including fusion genes) to detect the clinically actionable genetic variations in cancer. The total size of the targeted regions was 3.79 Mb. The constructed library was quantified using the KAPA Library Quantification Kit on the LightCycler 480 Instrument II (Roche, Basel, Switzerland). Paired-end sequencing was run on the Illumina NextSeq 550Dx sequencer using the NextSeq 500/550 High-Output v2 Kit (Illumina, San Diego, CA, USA). A TERTp somatic mutation (c.-124C>T) was identified in all specimens, while all other tumor-related genes were not detected including CDKN2A/B (Table 1). Thus, according to the 5th edition of the WHO central nervous system (CNS) tumor classification (WHO CNS 5), the patient’s meningiomas could be classified as grade 3 from the initial operation. The timeline table for the clinical course of the patient is illustrated in Table 2. After consultation with an oncologist, hydroxyurea was administered from 1 month after surgery. However, the 3-month follow-up brain MRI revealed a new lesion 9 mm in diameter at the lateral temporal base. The neuro-oncology board recommended SRS for that asymptomatic lesion, and 2,700 cGy/3 fractions was delivered. The patient was followed with caution for recurrence or new lesions.
DISCUSSION
Introduction of molecular markers in the diagnosis of CNS tumors and meningiomas
The WHO grading system for CNS tumors was initially introduced in 1979 and has undergone several major revisions in the decades since. Although the concept of atypical meningiomas was not introduced until 1993, many studies identified this aggressive subtype following the research published by Jellinger and Slowik [6] and Jääskeläinen et al. [7]. The WHO CNS 5—by far the most recent—was published in 2021 and further advanced the role of molecular diagnostics in CNS tumor classification while remaining wedded to other established approaches, such as histology and immunohistochemistry. This version also introduced new tumor types and subtypes, some of which are based on novel diagnostic technologies, such as DNA methylome profiling.
For meningiomas, the WHO CNS 5 retains the previous version’s grading system of 1–3 with 15 stratified subtypes. It emphasizes that the criteria defining atypical (grade 2) or anaplastic (grade 3) meningioma should be applied regardless of the underlying subtype. Previously, the factors differentiating meningiomas of grades 1–3 were solely histomorphologic. Aggressive, high-grade features included increased cellularity or mitotic index, a high nuclear-to-cytoplasmic ratio, prominent nucleoli, patternless or sheet-like growth, and the presence of necrosis or brain invasion [8]. However, despite its widespread use, the old grading system failed to accurately predict the clinical behavior, aggressiveness, and long-term recurrence of particular meningiomas [9]. In the new classification, several molecular biomarkers are associated with the classification and grading of meningiomas, including SMARCE1 (clear cell subtype), BAP1 (rhabdoid and papillary subtypes), and KLF4/TRAF7 (secretory subtype) mutations; TERTp mutation [10] and/or homozygous deletion of CDKN2A/B [11] (WHO grade 3); loss of nuclear H3K27me3 expression [12] (potentially worse prognosis); and methylome profiling [13] (methylation classes associated with increased risk of recurrence). Other key genes/molecular profiles characteristically alerted include NF2, AKT1, SMO, and PIK3CA in subtypes [14]. Importantly, according to the WHO CNS 5, no single, definitive criterion for grading meningiomas exists—appropriately combining the histopathologic, subtype (morphological), and mutational analysis results is essential for accurate diagnosis. Other genomic analyses, such as DNA copy number variations and DNA methylation profiles, have also proven more accurate in estimating the risk of recurrence compared with conventional histopathologic grading systems [115].
Multiple/recurrent meningiomas, malignant transformation of meningiomas, and TERT promoter mutation
Multiple meningiomas (MMs), referring to a subset of meningioma patients bearing two or more spatially separated, synchronous or metachronous tumors, account for 1%–10% of all meningiomas [16]. MMs are allegedly associated with genetic mutations, such as NF2, and are more frequently grade 2 or 3 meningiomas. However, Araújo Pereira et al. [17], in their analysis of MMs, revealed WHO grade 1 predominance similar to single meningiomas, and fewer than half of MM patients (43.89%) needed treatment.
Approximately 20%–40% of all high-grade meningiomas are secondary tumors that originally developed from WHO grade 1 tumors [18]. The literature suggests a step-by-step genetic progression in which the deletion of chromosome 22 is the fundamental genetic alteration and deletions in other chromosomes, such as 1p, 14q, and 10q, occur during malignant transformation [1920]. Consequently, high-grade meningiomas are classified as either de novo or secondary tumors. Some genetic differences between these two types have been reported: specifically, TERTp mutation is sometimes found in the latter but rarely in the former [212223]. Current research efforts aim to elucidate the histopathological changes associated with the malignant transformation of meningiomas, which is widely recognized as a combination of various oncogenic events. Some of the reported risk factors of malignant transformation of benign meningiomas include the histopathologic features of increased mitotic index [24] and non-skull base tumor location, without any apparent association with the patient’s sex or the primary treatment modalities (surgery or SRS) [25]. Moreover, several genetic mutations have also been linked to the malignant transformation of meningiomas, including FOXM1, TOP2A, BIRC5, MYBL2, and even TERTp [2226]. Few of these known risk factors were found in our case, as the tumor occupied a non-skull base location and harbored a TERTp mutation throughout the progression. Furthermore, although the histopathology from the first operation did not show an increased mitotic index, there was a prominent increase following the second operation. The underlying pathophysiological mechanisms behind the malignant transformation of meningiomas remain incompletely understood.
The systematic review and meta-analysis conducted by Nakasu et al. [25] specified an incidence rate of malignant transformation in benign meningiomas of 2.98 per 1,000 person-years. Individual case data revealed that the median time for malignant transformation was 5.0 years, with some cases of malignant change occurring up to 30 years after the initial surgery. Our case showed malignant transformation from grade 1 to grade 2 in 6 years, and from grade 2 to grade 3 in another 4 years.
TERTp mutation has been discovered as a driving factor in the aggressiveness of meningiomas, leading to reduced survival rates for patients [27]. Sahm et al. [10] reported that the inclusion of TERTp mutations in the hotspot regions C228T and C250T in meningioma samples from 252 patients enabled higher prognostic power because TERTp mutations were statistically significantly associated with shorter time to progression. Mirian et al. [28] found that TERTp gene alterations (TERT-alt) affected prognosis independent of the previous WHO grades: the recurrence rate was 4.8 times higher in WHO grade 1 or 2 TERT-alt patients compared with WHO grade 3 TERT wild-type patients, and the mortality rate was 2.7 times higher in WHO grade 1 or 2 TERT-alt patients compared with WHO grade 3 TERT wild-type patients. Therefore, TERTp mutation serves as a crucial biomarker, indicating a significantly higher risk of recurrence and death in meningioma patients. In our case, histologic findings from the first operation did not show any aggressive features except for slightly increased cellularity. From the second operation, although the histology from the right temporal and middle frontal lesions with RT-related changes remained relatively non-aggressive, the newly grown temporal lesion despite SRS (Fig. 3D and H) started to show an increased mitotic index (10/10 high-power fields [HPF]). Subsequently, newer aggressive histologic features, such as increased cellularity, patternless or sheet-like growth, and prominent nucleoli, emerged throughout the third and fourth operations, and the mitotic index peaked (21/10 HPF) in the fifth operation to satisfy classification as grade 3 meningioma. However, because the TERTp mutation was found to be present from the first operation despite CDKN2A/B was not, all the lesions from then on can be classified as grade 3 meningiomas according to the WHO CNS 5.
The treatment strategies for high-grade meningiomas resulting from malignant transformation do not specifically differ from ordinary management of meningiomas, though some potential therapies targeting specific molecular markers are on the rise. As TERTp mutation is a widely known pathologic mutation for tumorigenesis, recurrence, and progression, our patient’s meningiomas since the initial diagnosis in 2013 can be understood to be more susceptible to further recurrence and progression than if the mutation was not present. However, TERTp mutations vary from benign to pathogenic. The culprit mutations reported as “pathogenic/likely pathogenic” according to ClinVar (a public genomic database) include -146G>A (referred to as C250T) and -124G>A (referred to as C228T), which form the basis for 2021 WHO CNS 5 modifications [102223]. Our meningioma case presented with a c.-124C>T (C228T) mutation.
The limitations of our case are as follows. First, the NGS results were of poor quality with limited depth, especially for the 2013 specimen due to DNA degradation of the FFPE slides. Second, if the NGS results of pathogenic variants related to malignant transformation of meningioma were available earlier, more aggressive presumptive measures, such as radical resection with wider surgical margins or higher-dosed RT/SRS, could have been considered to prevent the tumor from recurring.
Based on our experience with this case, we suggest routinely performing early-stage genomic analysis, such as NGS, to look for the above-mentioned mutations related to malignant transformation/prognostication, including TERTp mutations, for all newly diagnosed meningioma patients. If any such mutations are detected, appropriate preemptive measures for treating and monitoring TERT-alt patients must be taken for preventative or surveillance purposes.

 XML Download
XML Download