

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
High-grade gliomas (HGG) are the most common primary malignant central nervous system (CNS) tumors comprising mainly the glioblastoma multiforme (GBM) subtype (World Health Organisation [WHO] grade 4) [12]. Anaplastic astrocytomas (AA) were previously classified as WHO grade 3 based on greater degree of cellularity, nuclear pleomorphism, and mitotic activity as compared to low-grade gliomas (WHO grade 2). However, unlike GBM that are 20 times more frequent, AA lack vascular proliferation and necrosis on histopathological examination. However, both types exhibit parenchymal infiltration and thus remain almost incurable [23]. Others much less frequent subtypes such as anaplastic oligodendroglioma (AO), anaplastic oligoastrocytoma, or malignant glioneuronal tumor also fall into the category of HGG. Previous classifications of brain tumors based solely on histopathological criteria were limited by diagnostic discrepancies and variability in outcome and response to therapies. In France, the standard of care for newly diagnosed GBM includes maximal safe resection, concurrent temozolomide (TMZ) during radiotherapy (RT), and adjuvant TMZ for six or more 28-day cycles [4]. Grade 3 gliomas can be either treated like GBM or with combined chemotherapy using procarbazine, lomustine, and vincristine (PCV) or with TMZ after surgical resection, followed then by RT. AOs are also responsive to PCV chemotherapy, especially when harboring 1p19q codeletion. The 2021 fifth edition of the WHO Classification of Tumors of the Central Nervous System incorporated advances in understanding the molecular pathogenesis of brain tumors with histopathological criteria in order to group tumors into better defined entities. For the first time, adult- and pediatric-type gliomas were classified separately based on differences in molecular pathogenesis and prognosis. Furthermore, the previous broad category of adult-type diffuse gliomas was consolidated into three types: astrocytoma, isocitrate dehydrogenase (IDH) mutant; oligodendroglioma, IDH mutant and 1p/19q codeleted; and GBM, IDH wild type. These major changes were driven by IDH mutation status and included the restriction of the diagnosis of GBM to tumors that are IDH wild type; the reclassification of tumors previously diagnosed as IDH-mutated GBM as astrocytomas IDH mutated, grade 4; and the requirement for the presence of IDH mutations to classify tumors as astrocytomas or oligodendrogliomas. These changes will likely improve dedicated treatment efficacy and, hence the homogeneity of outcome.
Administrative medical databases are massive repositories of collected healthcare data for various purposes with a constant and often ongoing collection process. They frequently encompass the whole nation, a region, or a scheme ensuring high statistical power. In that respect, the French nationwide healthcare database, the Système National des Donnèes de Santé (SNDS), is a great opportunity to carry out comprehensive health studies at the country level [5]. In France, to date, no one has ever attempted to assess the outcome of HGG patients using the SNDS.
The aim of this study was to assess the overall survival of patients after HGG resection and to search for associated prognostic factors using information collected and available in the SNDS.
Go to : 
MATERIALS AND METHODS
Clinical material and population selection
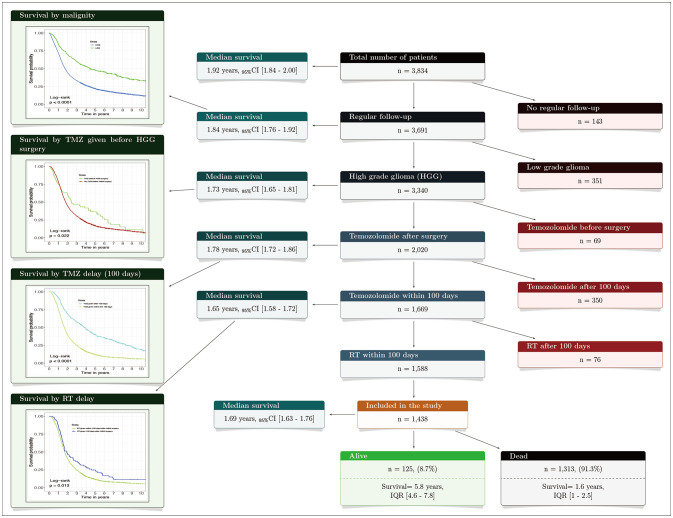
We performed a cross-sectional and longitudinal nationwide observational retrospective study using the SNDS. The SNDS database links claims with hospital discharge summaries and the national death registry, using pseudonymization of the unique national identifier. It now covers 99% of the French population, over 66 million persons, from birth to death, making it one of the world’s largest continuous homogeneous claims database. The database includes demographic data, date and cause of death, long-term disease registration for full reimbursement, outpatient reimbursed healthcare encounters such as physician or paramedical visits (e.g., nursing, physiotherapy), medicines prescribed, medical devices, lab tests with costs; all private and public hospitalizations with primary, linked and associated ICD-10 (International Classification of Diseases 10th Revision) diagnoses, procedures, duration, and cost coding system as well as most very expensive drugs. The power of the database is correlatively great, and its representativeness is guaranteed. As such over 3,000 variables are spread into around 500 tables. For this study, we used many variables such as date of birth, sex, previous neurosurgical procedure, past medical history of neoplasm, age at surgery, anatomical location of the tumor, delay between HGG resection and chemotherapy start, chemotherapy (molecule(s), dose, duration, number of course), delay between HGG resection and RT start, number of RT fraction, duration of the RT, anti-epileptic treatment (molecule, dose, duration), redo neurosurgical procedure, and date of death. A random sample of patients treated for a malignant brain tumor was extracted from the SNDS and provided to us for research purpose. The period of selection of patients operated on for an HGG extended from January 1, 2008, up to December 31, 2017. Patients were then followed up until December 31, 2020. An algorithm combining two variables to get appropriate cases was used: the type of the surgical procedure identified by the French Common Classification of Medical Acts (CCAM) which describes precisely all medical and surgical interventions (AAFA002: Exérèse de tumeur intraparenchymateuse du cerveau, par craniotomie; resection of an intracerebral tumor by craniotomy) [678]. The second variable taken into account was the main diagnosis of malignant cerebral tumor according to the ICD-10 code C71.x: malignant neoplasm of brain. As such metastasis (C79.3 secondary malignant neoplasm of brain and cerebral meninges) or other types of brain tumors were not taken into account. In this study, we solely considered newly diagnosed HGG resection. The patients who solely had a brain biopsy were not considered. However, the patients who had a brain biopsy followed by HGG surgery were included. To ensure that no low-grade glioma were represented in our study, a complex selection process was applied to our initial population in order to keep only HGG patients (Fig. 1). The Mortality-Related Morbidity Index (MRMI) predictive of all-cause mortality was used to assess the severity of the patient’s global health state including numerous comorbidity [9]. This weighted index summarizes the association between a set of conditions identified through algorithms using SNDS data and each outcome [10]. The MRMI index has been validated against the most commonly used morbidity indices [9]. Chemotherapy and other medications such as anti-epileptic drugs were retrieve across the databases using ad hoc “Unité Commune de Dispensation” (UCD) or “Code Identifiant de Présentation” (CIP) codes. Aware that coding rules are somewhat inconsistent, we applied a stepwise selection algorithm to the initial population as our goal was to target mainly GBM patients (Fig. 1). As standard treatment after HGG resection is chemoradiotherapy with temozolomide (TMZ/RT), we solely considered the patients who received this therapy after surgery. All HGG patients who at least completed the RT and initiated the TMZ adjuvant phase were included.
Statistical analysis
Continuous variables were reported as means and standard deviations or medians and interquartile ranges (IQR) for non-Gaussian distributions. Categorical variables were reported as frequencies and proportions. Survival statistics were based on time to death, which was measured from the first date of HGG surgery to the date of the last follow-up or death. We used the Kaplan–Meier method to estimate the OS and the Mantel–Cox log-rank test to compare survival curves. Cox proportional hazards regressions were used to identify predictors of death and to estimate hazard ratio (HR) with their 95% confidence intervals (95% CI). All tests were two-sided, and statistical significance was defined with an alpha level of 0.05 (p<0.05). Data extraction and processing were achieved with SAS Enterprise Guide version 8.3 (SAS Institute Inc., Cary, NC, USA), and analyses were performed with the R programming language and software environment for statistical computing and graphics (R version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria). The statistical programme and workflow was written in R Markdown v2 with RStudio® for dynamic and reproducible research.
Compliance with ethical standards
This study was conducted according to the ethical guidelines for epidemiological research in accordance with the ethical standards of the Helsinki Declaration (2008). It was also approved by the French Data Protection Authority (Commission nationale de l'informatique et des libertés) an independent national ethical committee, authorization number: DR-2021-352.
Go to :
RESULTS
Population description
A total of 1,438 patients who had HGG resection between 2008 and 2017 were selected. Among them, 34.8% were female, and median age at HGG resection was 63.2 years (IQR 55.6–69.4) (Table 1). Females were significantly older at surgery (64.3 years) compared to males (62.4 years) (p=0.003). According to the MRMI index, male had a significantly higher mortality risk at baseline compared to female (p=0.008) (Table 1). Additionally, 51.8% of the patients had at least one seizure, and 73.6% used to take an anti-epileptic medication over 3 months of which levetiracetam was the most often prescribed with 65.3%. The median follow-up time was 7.4 years (95% CI 5.4–8.8).
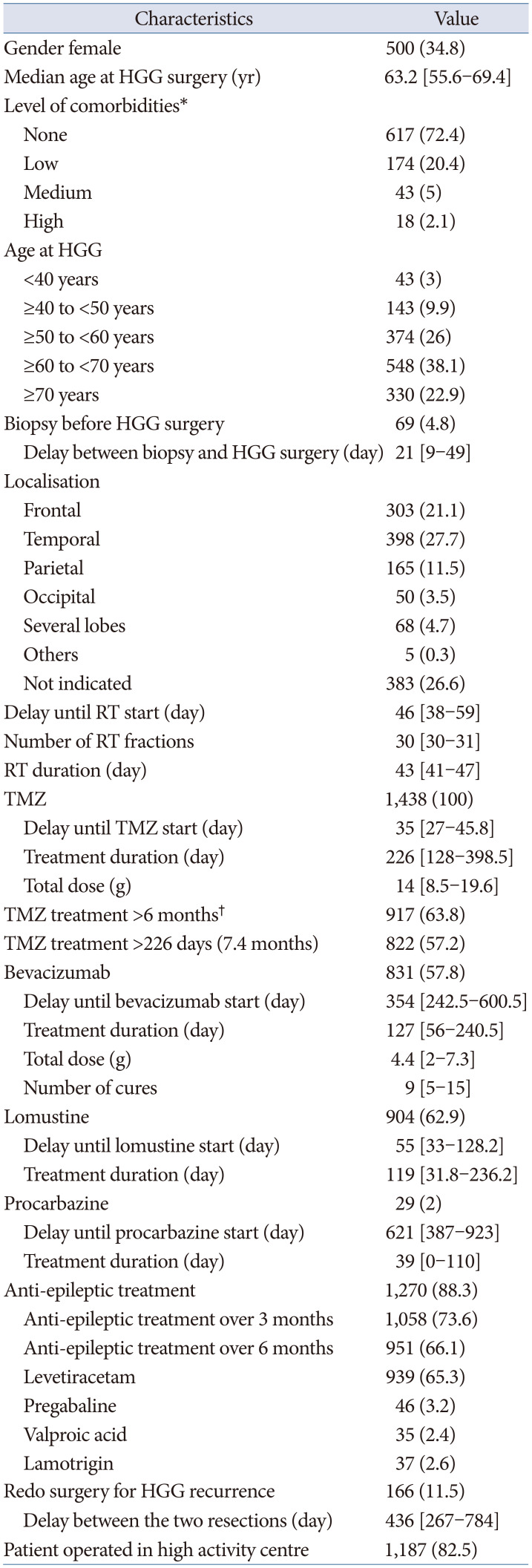
Table 1
Characteristics of the 1,438 patients with HGG resection
![]()
Outcome
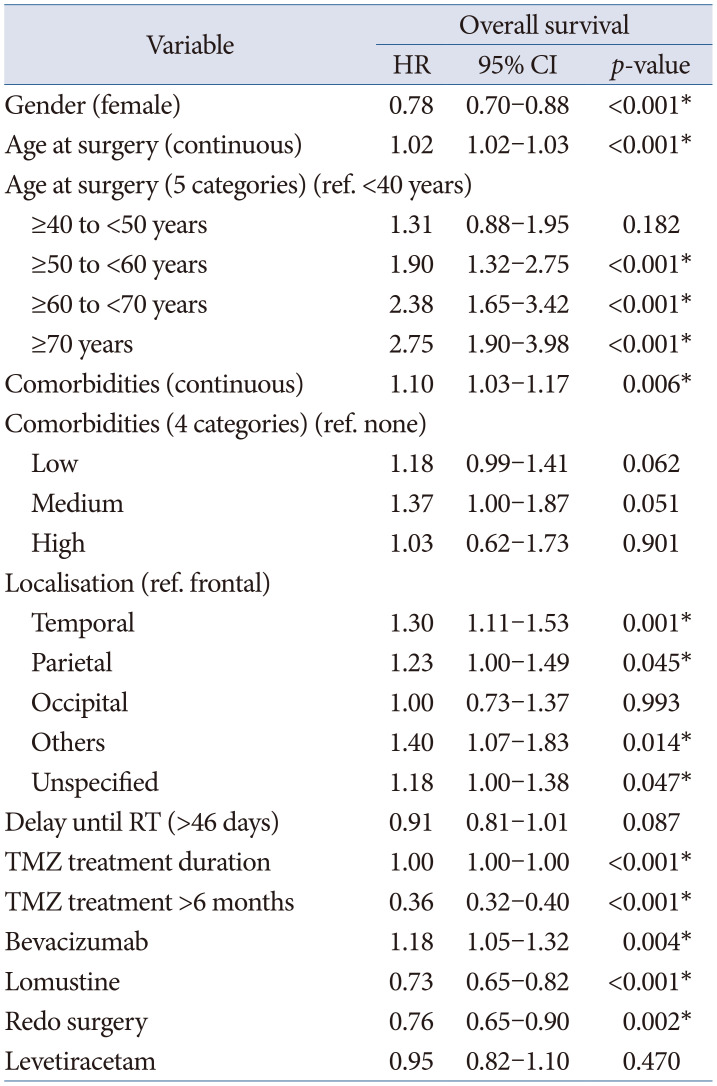
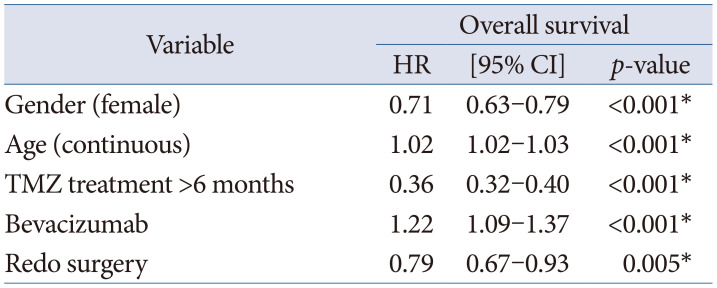
Fourteen (1%) patients died within the 3 postoperative months of HGG resection. Ultimately, 1,313 patients (91.3%) had died at data collection, and median age at death was 65.5 years (IQR 58.5–71.8) (Fig. 1). Median OS was 1.69 years (95% CI 1.63–1.76). OS at 1, 2, and 5 years was 78.5% (95% CI 76.4–80.7), 40.3% (95% CI 37.9–43), and 11.8% (95% CI 10.2–13.6), respectively. In the adjusted regression, gender (HR=0.71, 95% CI [0.63–0.79], p<0.001), age at HGG surgery (HR=1.02, 95% CI [1.02–1.03], p<0.001), TMZ treatment over 6 months (HR=0.36, 95% CI [0.32–0.4], p<0.001), bevacizumab (HR=1.22, 95% CI [1.09–1.37], p<0.001), and redo surgery (HR=0.79, 95% CI [0.67–0.93], p=0.005) remained significantly associated with the outcome (Tables 2, 3; Figs. 2, 3).
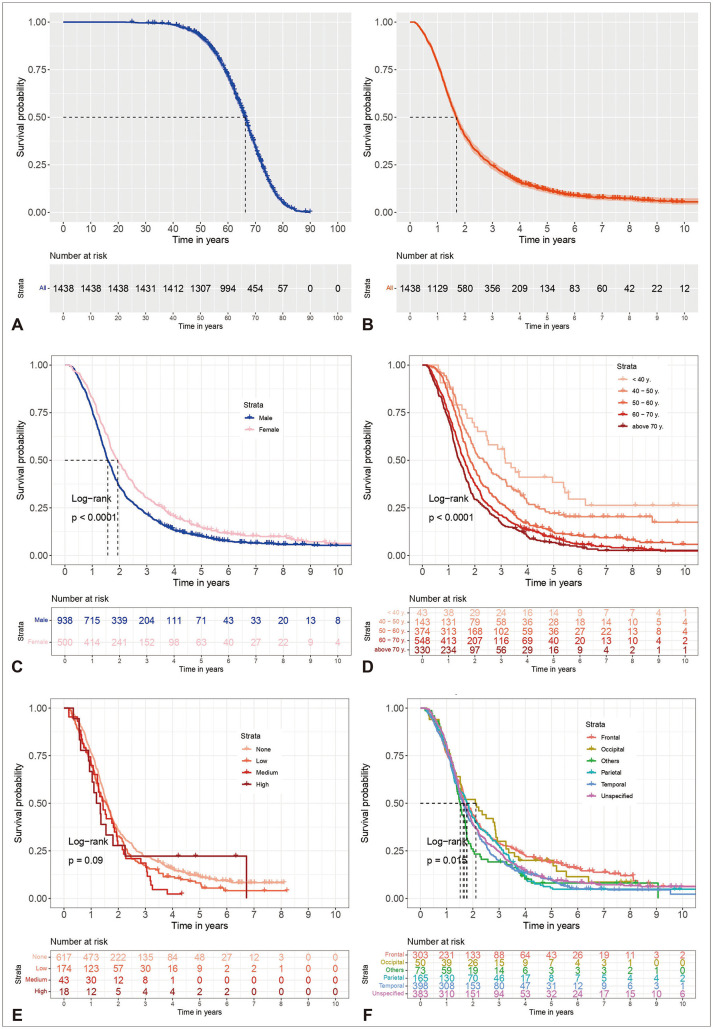 | Fig. 2Kaplan-Meier curves for overall survival (OS). A: OS from date of birth. B: OS from high-grade glioma surgery. C: OS by gender. D: OS by age categories. E: OS by categories of comorbidity index. F: OS by tumor location.
|
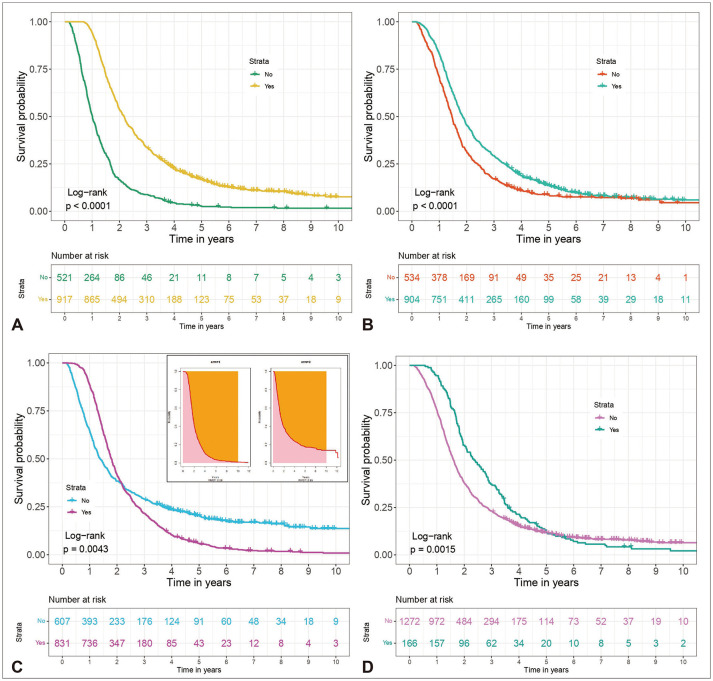 | Fig. 3Kaplan-Meier curves for overall survival (OS) by treatment. A: OS by temozolomide duration over 6 months. B: OS by lomustine. C: OS by bevacizumab, with restricted mean survival time plot. D: OS by redo surgery for HGG recurrence.
|
Table 2
Univariable Cox regression of overall survival
![]()
Go to :
DISCUSSION
HGG remains one of the least treatable cancers. The current standard therapy for HGG represented by maximal surgical resection combined with chemo- and radiotherapy, offers only a palliative treatment since the median OS is less than 2 years [411]. We report herein on the outcome of a sample of 1,438 patients who had HGG resection. The present study, one of the largest on outcomes after HGG resection in France, may serve as a reference for future research.
Our population characteristics are quite similar to those described in previous studies with a median age at HGG surgery of 63.2 years (IQR 55.6–69.4) [1213]. In Nunna et al. [13], 45.8% of the patients were above 65 years, compared to 42.9% in the present report, but only 24.4% in Kuo et al. [14]. Additionally, 22.9% of our patients were above 70 years, compared to 17.4% of Yoshimoto et al. [12], which used a methodology quite similar to ours. A male preponderance has been consistently reported (56.8%–61%), but our proportion of 65.2% is surprisingly high [12131415].
Outcome
In the present study, the median OS was 1.69 years (95% CI 1.63–1.76), i.e., 20.28 months. Our finding is above the “classical” ranges of previously reported results. Patients had a poor median OS of solely 9.4 to 15 months in the case of GBM, and around 36 months for AA [411]. Nunna et al. [13] queried the National Cancer Database (NCDB) over the 2004–2016 period to assess 104,456 GBM patients and found a mean OS of 9.1 months (standard deviation [SD], ±10.0) and, 5-year OS was 5.3% [13]. Using 3,895 histologically confirmed GBM, Shieh et al. [16] retrieved a median survival of 12.6 months (95% CI 12.1–13.2). For Kang et al. [17], 1-, 2-, and 5-year relative survival rates were for 5,754 GBM patients 59.3% (95% CI 58.0–60.6), 30.4% (95% CI 29.2–31.7), and 12.1% (95% CI 11.1–13.1), respectively. In Hansen et al. [15], the median overall survival for all GBM patients was 11.2 months. However, in Fabbro-Peray et al. [18], the patients who had HGG resection followed by a complete Stupp regimen (6 TMZ cycles) demonstrated a median survival of 25.5 months (95% CI 24.0–28.3). Based on 2,379 patients with HGGs who underwent TMZ treatment, Kuo et al. [14] report a mean OS time of 50.3 months (SD, ±41.0).
The restricted mean survival time (RMST) is determined by measuring the area under the Kaplan–Meier survival curve. It can be defined as the average event-free survival time, ranging from 0 up to a specific prespecified important time point that reflects a clinically relevant temporal horizon, such as 5 years. As the median survival time is insensitive to outliers, it is expected to be much shorter than the mean survival time in the presence of many long-term survivors. Although the median survival time is easy to understand, it describes only the outcome at a single time point, i.e., the length of time after which half of the HGG patients are dead. RMST can be seen as an improvement of the median because it can be computed with no exceptions (i.e., irrespectively of the number of events that have occurred) and, more importantly, it examines the entire shape of the survival curve (from time 0 to the last time-point of the follow-up) and therefore takes into account the presence of long-term survivors [19]. Comparatively, in our study, the 5-year RMST was 2.16±0.04 years.
Unsurprisingly, the outcome is better in the case of AA, with 1-, 2-, and 5-year relative survival rates being 71.4% (95% CI 68.4–74.2), 46.8% (95% CI 43.5–50.0), and 26.2% (95% CI 23.1–29.4), respectively [17].
Even if prolonged survival of HGG patients has been reported, it is nonetheless a rare eventuality. In our study, 125 patients (8.7%) were found to be alive at data analysis, and for these alive patients, the median survival was 5.8 years (IQR 4.6–7.8). Most of these long survivors may likely have an AA and not a GBM. OS of GBM, including all cases, is nowadays around 12 months [16]. However, many factors influence patients’ outcomes.
Predicting factors
Unsurprisingly, age at surgery was one of the favorable predictors but, gender also. Despite the fact that female patients were older at surgery, they demonstrated a significantly better OS. We confirm herein that women have the survival advantage in HGG patients who have received standard of care treatment [20]. Of the numerous factors associated with the OS, HGG subtypes are one of the strongest. Despite GBM patients constituting the vast majority of this sample, it was not possible to precisely identify AA and AO patients whose better outcome, increased the global OS in this study. However, AO is preferentially treated with the PCV regimen. Our stepwise selection algorithm, which includes solely the patients who received concomitant TMZ and RT within the 100 postoperative days, mostly targets newly diagnosed HGG.
The patients who received TMZ for 6 months or more demonstrated a better outcome. The DNA repair enzyme O(6)-methylguanine-DNA methyltransferase (MGMT) antagonizes the genotoxic effects of alkylating agents. MGMT promoter methylation is the key mechanism of MGMT gene silencing, and predicts a favorable outcome in HGG patients who are exposed to alkylating chemotherapy [21]. MGMT promoter methylation status is not only prognostic but also predictive of a better response to chemotherapeutic agents in GBM, such as TMZ or carmustine (Bis-ChloroethylNitrosoUrea, BCNU). On the contrary, GBM patients with unmethylated MGMT promoters have limited survival benefits from TMZ [22]. The better OS of patients who received TMZ over 6 months may reflect this molecular features of the GBM cells.
There is much debate regarding the use of bevacizumab in HGG patients. Bevacizumab slows tumor growth but does not affect OS of newly diagnosed GBM patients, nor of those presenting a recurrence [23]. In our study, those who received bevacizumab had a reduced OS (HR=1.22, 95% CI 1.09–1.37, p<0.001). Under the proportional hazards assumption, crossing of the survival curves is impossible. Thus, in a study where the patient groups do not differ between the treatments, a crossing of the survival curves implies a violation of the proportional hazards assumption. As discussed previously, the RMST has been recommended as an alternative measure to overcome some of the limitations of proportional hazard modeling. As such, Fig. 3C present the plot of 10-year mean restricted survival time for patients who received bevacizumab (arm=1, RMST=2.28 years) vs. those who did not (arm=0, RMST=2.96 years) (p<0.001). This finding is however hard to interpret as this anti-angiogenic therapy may have been given in combination with chemotherapy. However, it likely reflects the fact that patients receiving bevacizumab are those with rapidly progressing tumors causing symptomatic edema, and who consequently have worse survival.
HGG nearly always recurred, often in the vicinity of the original tumor site. Few treatment options are then available at recurrence. There is much evidence that the extent of resection for newly diagnosed HGG increases OS. Whilst the role of initial aggressive resection has become standard practice, its implication for recurrent GBM is still controversial. With the surgical progresses and adjuvant treatment modalities, many patients are now surviving to recurrence in good functional status. The indications for redo surgery include among others individuals with tumor mass effect or radiographic evidence of progression with or without new neurological deficit. In a review investigating reoperation for recurrent HGG, Hervey-Jumper and Berger [24] found that 29 studies among 31 showed a survival benefit or an improved functional status. In Sacko et al. [25], the median OS of patients who underwent repeat resection for HGG recurrence was significantly better than that of those who did not, with 23 months (95% CI 20.20–28.85) vs. 14.6 months (95% CI 12.63–16.81), respectively (p<0.05). In France, redo craniotomy for recurrent GBM is around 9%, a rate inferior to the North American series (13%–31%) [112426]. OS after a second resection for HGG recurrence varies greatly from one month up to over one year [2427]. No meta-analysis of OS rates has ever been published; however, Montemurro et al. [27] in their “concise overview of the current literature” found a median OS of 9.7 months after recurrent HGG surgery. Some comparative studies have suggested a possible survival advantage with re-operation within the context of being able to select suitable candidates for re-operation [28]. There is no agreement about the best way to manage recurrent HGG, given that no treatment has ever been shown to be more beneficial than another [29]. The management of recurrent HGG is thus based on expert guidelines. Treatment decisions usually require multi-disciplinary discussion on a case-by-case basis to determine the optimal option.
Strengths and limitations
The strengths of the SNDS lie both in the large number of patients and in the comprehensive data available from every hospital in France. The database’s representativeness is nearly perfect, as it includes the whole country’s population of nearly 68 million inhabitants constituting one of the largest healthcare databases in the world [5]. Evaluation of patients before that time is therefore not possible. These data were not initially collected for research purposes, and they may therefore be subject to random or systematic measurement errors, which can have consequences when defining study populations, events, and covariates. Compiled from various institutions, its accuracy is limited by inconstancies in data collection and recording. Moreover, important variables such as the quality of resection or histopathological details are not recorded in the SNDS. The retrospective nature of this study, together with the lack of clarity regarding treatment rationales and non-homogeneous management strategies without random assignment, needs to be considered when evaluating the results. The most significant limitation of our study was the lack of histological diagnoses, which made it impossible to assess the OS by glioma subtypes. Without knowing the exact tumor types, caution should be taken whilst attributing the observed survival differences solely to the presented factors rather than to the inherent biology and prognosis of different glioma subtypes. Using the ICD-10 code C71, we assumed that we could extract mainly data on astrocytic, oligodendroglial, ependymal, and other neuroepithelial tumors. Primary CNS lymphomas were not included as they are specified by a different code (C83/C85). We also hypothesized that no malignant meningeal (C70) or metastasis (C79.3) were included in the analysis. Patients with malignant tumors of the sellar region were also excluded. Moreover, we apply a strict selection process to exclude as much as possible unwanted brain neoplasms. Nonetheless, our median survival of 1.69 years (95% CI 1.63–1.76) is greater compared to usual findings. This likely betrayed the presence of borderline or benign primary brain tumors such as low-grade glioma within our population. Despite these limitations, the SNDS is an invaluable tool to assess HGG patients’ outcomes. It offers an incomparable means to explore associations with other pathology, medication, or combined surgical treatments, which could not be assessed before. Moreover, use of these databases is less expensive than conducting specific surveys in dedicated populations. However, SNDS data extraction and analysis is a complex task that requires dedicated training, coding expertise, and special authorizations. We estimated that around 3,000 cases of HGG are operated each year in France. However, solely a random sample of patients treated for a malignant brain tumor was extracted from the SNDS and provided to us for research purposes. The SNDS is a huge medical database covering over 95% of the 68 million inhabitants with a 20-year follow-up. We cannot directly have access to this complex database. However, to assess its usefulness for studying the outcome of HGG patients, a random sample of 3,834 patients was provided to us to perform this pilot study whose results are described in the present paper.
Perspectives
The main weakness of the present work is the absence of verified HGG histopathology. Our study was made with healthcare data extracted from the French administrative medical database that does not record precise histopathological diagnoses. The French Brain Tumour Database (FBTDB) is an original, nationwide, surgical-based system for registration of histological cases of primary CNS tumor (PCNST) [2330]. The FBTDB is hosted by the Hérault Tumours Registry which is part of Francim, a network grouping the French cancer registries. This collection process is a one-time registration with no information regarding the treatment, the follow-up, or the outcomes. Tumor characteristics and patient’s demographic details are registered once. Patient’s information is not updated, and solely new cases of brain tumors enrich the database over time. Our project is thus to merge the FBTDB with the SNDS to assess HGG patients’ outcomes according to each subtype.
Conclusion
The SNDS is a reliable source to study the outcome of HGG patients. OS is better in younger patients, females, and those who complete concomitant chemoradiotherapy. Additionally, redo surgery for HGG recurrence was associated with prolonged survival.
Go to :
 XML Download
XML Download