

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
High-grade transformation after surgical resection of low-grade gliomas is a well-recognized phenomenon that leads to poor prognosis, but its pathophysiology is not yet completely understood. Research has reported that approximately 45% of oligodendrogliomas, 70% of oligoastrocytomas, and 74% of astrocytomas eventually undergo high-grade transformation [1]. Old age, male sex, and residual tumor after resection are common risk factors for high-grade transformation of low-grade gliomas [2]. Biologically, clonal evolution and therapy-driven genetic changes have been implicated as underlying mechanisms of high-grade transformation [34]. In the case of astrocytomas, gemistocytic tumor histology was shown to be an independent risk factor for both high-grade transformation and shorter overall survival [56]. However, the 2021 World Health Organization (WHO) Classification of Tumors of the Central Nervous System (CNS) no longer specifies histological subtypes of astrocytomas [7].
Here, we present a case of early recurrence of a CNS WHO grade 2 astrocytoma with high-grade transformation in a young adult after gross total resection, and review its pathological implications in relation to the WHO diagnostic criteria.
Go to : 
CASE REPORT
A 34-year-old male patient with no significant medical history presented to a tertiary medical institution with generalized seizures. After management with anti-seizure medication, a neurological examination revealed no additional focal deficits. Brain MRI performed at the initial hospital showed an approximately 8-cm diffuse, infiltrative, non-enhancing mass lesion in the left temporal lobe (Fig. 1A). Based on clinical presentation and imaging features, a tentative diagnosis of low-grade glioma was made, and curative surgical resection was planned.
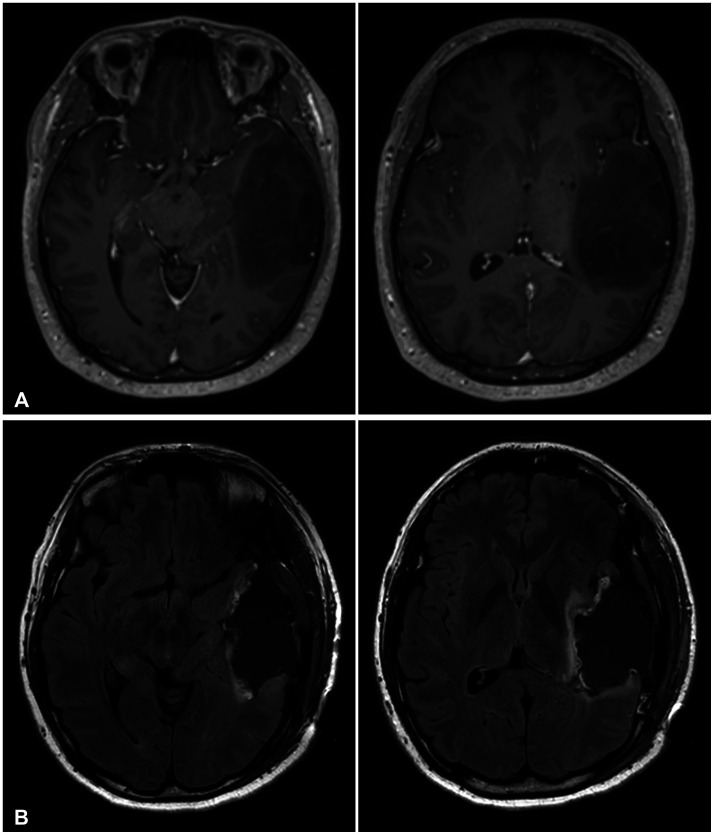
A standard left temporal craniotomy was performed at the initial hospital, achieving gross total resection with clear surgical margins (Fig. 1B). The final pathology results revealed an isocitrate dehydrogenase (IDH)-mutant, CNS WHO grade 2 astrocytoma according to the 2021 classification system. Histologically, fibrillary, gemistocytic, and protoplasmic features were all present (Fig. 2). IDH mutation and ATRX loss were noted on immunohistochemical staining. Genetic analysis was negative for CDKN2A/B homozygous deletion, as well as TERT promoter mutations and MGMT promoter methylation. Adjuvant therapy was not planned, considering the low tumor grade, gross total resection status, and young age. The patient was discharged from the hospital with no acute complications or neurologic abnormalities. Regular imaging follow-up was planned in 6-month intervals.
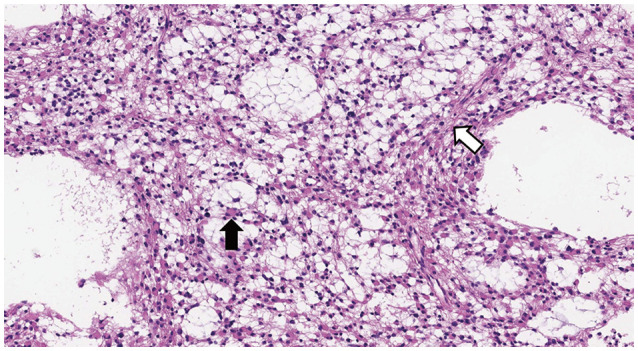 | Fig. 2Histopathological examination of the first operation (×200 magnification). Hematoxylin and eosin–stained tissue section showing gemistocytic features, with large eosinophilic cytoplasm with nuclei displaced to the periphery (black arrow). Other neoplastic fibrillary astrocytes show mild nuclear atypia on the background of a loosely structured tumor matrix with microcyst formation (white arrow).
|
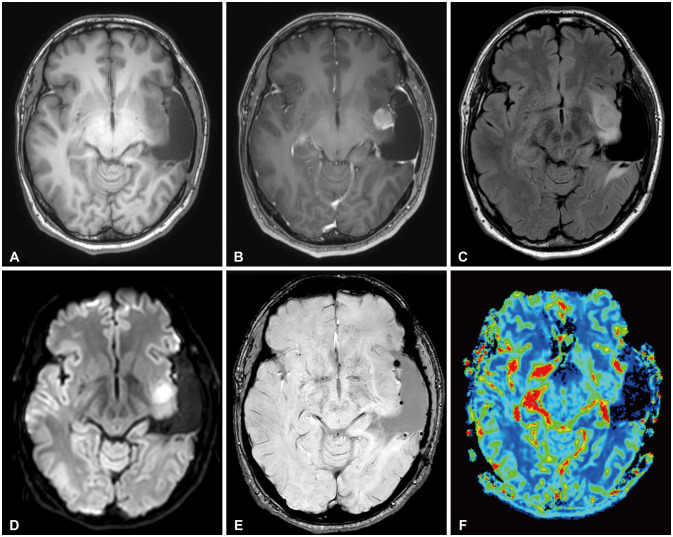
Six months after surgery, a follow-up brain MRI showed no signs of tumor recurrence. However, 1 year after surgery, a brain MRI revealed an approximately 2-cm round, solid, enhancing mass in the left insular region, with perilesional T2 high signal intensity (Fig. 3). Homogenous diffusion restriction with a mild increase in cerebral blood volume suggested tumor recurrence with high-grade transformation. Although the patient did not show any symptoms or neurological deficits, surgical resection was recommended for diagnostic and curative purposes.
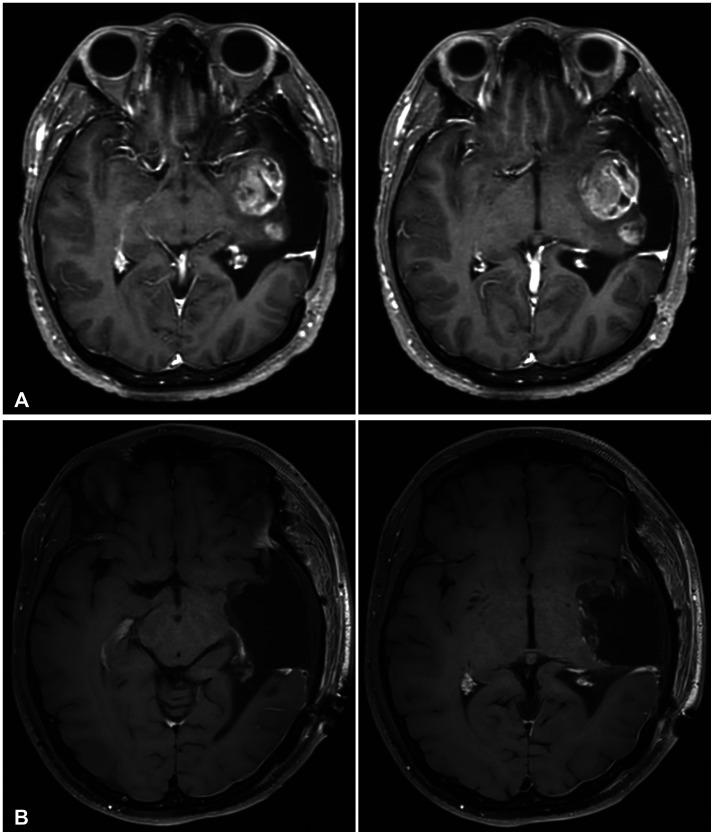
The patient was referred to another tertiary medical institution for a second opinion. Two months thereafter, a short-term follow-up brain MRI showed an increased size of the primary mass and another newly appeared enhancing mass in the posterior margin of the left insula (Fig. 4A). A left temporal craniotomy was performed identically to the first surgery. A gliotic membrane was observed along the resection cavity, and a grayish tumor was readily exposed directly underneath. Both masses showed jelly-like, hypovascular consistency, in contrast to normal tissue, and were easily removed with ultrasonic aspiration. Special care was taken to preserve the lenticulostriate arteries and the posterior limb of the internal capsule. Gross total resection was achieved with clear resection margins in the operative field and was confirmed by postoperative brain MRI (Fig. 4B).
The final pathology results revealed an IDH-mutant, CNS WHO grade 4 astrocytoma according to the 2021 classification system. Histology showed microvascular proliferation and very poor differentiation, including sarcomatous and giant cell appearances, and the astrocytoma bore almost no resemblance to the initial tumor (Fig. 5A and B). Immunohistochemical staining for IDH1 R132H mutation was also strongly positive (Fig. 5C). The MGMT promoter was not methylated, and ATRX loss was found.
 | Fig. 5Histopathological examination of the second operation (×200 magnification). A: Hematoxylin and eosin–stained tissue section showing microvascular proliferation. B: Same hematoxylin and eosin-stain showing bizarre, monstrous, multinucleated tumor cells with high cellularity (black arrows). The nuclei varied in size, and some cells showed atypical mitoses (white arrow). C: Immunohistochemical staining positive for IDH mutation (using IDH1 R132H monoclonal antibody).
|
Immediately after surgery, the patient did not show any neurological deficits and seemed to recover well. However, 4 days after surgery, he developed sudden right-side weakness and numbness, and right homonymous hemianopsia. Diffusion MRI showed acute infarctions at the posterior limb of the left internal capsule, posterior thalamus, and corona radiata, most like due to local vascular compromise during surgery (Fig. 6A). The symptoms gradually improved with hydration and rehabilitation, and the patient was discharged 10 days after surgery.
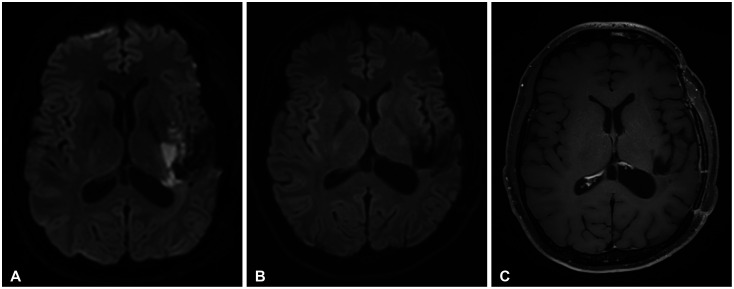 | Fig. 6Unexpected postoperative cerebral infarction and follow-up MRI. A: Diffusion-weighted MRI 4 days after surgery revealed multifocal diffusion restriction at the left internal capsule posterior limb, posterior thalamus, and corona radiata, indicative of acute infarction. Diffusion-weighted (B) and T1 contrast-enhanced (C) MRI before standard concurrent chemoradiation therapy showed minimal cerebromalacia at the infarction site without any enhancing lesions.
|
On consultation, the radiation oncologist advised avoiding immediate radiation therapy to the infarcted cerebrum until full recovery and suggested delaying radiation therapy up to 3 months after surgery. Two cycles of ifosfamide–carboplatin–etoposide (ICE) chemotherapy followed by standard concurrent chemoradiation therapy (CCRT) were then planned. The pre-CCRT brain MRI after two cycles of ICE chemotherapy showed only minimal cerebromalacia at the infarction site, with no evidence of tumor recurrence (Fig. 6B and C). The patient recovered from the hemiparesis completely, but the numbness and right homonymous hemianopsia remained.
Go to :
DISCUSSION
High-grade transformation of low-grade gliomas poses significant clinical challenges due to its unexpectedly aggressive clinical course. In the 2016 WHO classification of CNS tumors, such cases were referred to as “IDH-mutant glioblastoma” or, colloquially, “secondary glioblastoma” [8]. Despite their similar histological appearance, IDH-mutant and IDH-wildtype glioblastomas are considered distinct tumor entities that originate from different pathological pathways and require tailored clinical management [9]. This recognition originated from many studies showing that IDH-mutant gliomas showed better prognosis and response to treatment compared to their IDH-wildtype counterparts [101112].
In the 2021 WHO classification of CNS tumors, all IDH-mutant diffuse astrocytic tumors are now considered a single type, which is then graded as 2, 3, or 4 according to histological or molecular criteria. A glioblastoma diagnosis is applicable only when IDH mutation is absent; thus, “IDH-mutant glioblastoma” is currently an obsolete nomenclature. Furthermore, given the shift toward precise molecular diagnoses, histological subtypes of astrocytomas are no longer defined [7]. Therefore, IDH mutation status is now a disease-defining feature, and no longer considered a prognostic factor within a given disease subtype.
Recent clinical practice guidelines on adult diffuse gliomas have taken into account such major changes in pathological and molecular diagnosis. These include the European Association of Neuro-Oncology (EANO), National Comprehensive Cancer Network (NCCN), and Korean Society for Neuro-Oncology (KSNO) guidelines [1314]. All three guidelines recommended conservative management after resection of WHO grade 2 IDH-mutant astrocytoma for low-risk patients (i.e., age under 40 and gross total resection status).
In a recent single-center retrospective analysis of IDH-mutant low-grade gliomas, gross total resection was shown to delay high-grade transformation of grade 2 astrocytomas and improve overall survival. Interestingly, this effect was not significant for grade 3 astrocytomas or grade 2 oligodendrogliomas [15]. These results further emphasize the role of gross total resection in the treatment of grade 2 astrocytomas. Classically, gemistocytic astrocytomas have been associated with significantly higher rates of high-grade transformation and shorter overall survival compared with purely fibrillary or protoplasmic subtypes [1617]. Gemistocytes are glassy, plump, angular eosinophilic cell bodies showing glial fibrillary acidic protein (GFAP)-positive processes that may form a fibrillary network, as shown in the pathological examination of the first surgical specimen. Although the aggressive pathophysiology of gemistocytic astrocytomas has not yet been completely elucidated, some molecular studies suggest that the high frequency of p53 mutations and bcl-2 hyperexpression among gemistocytes lead to increased malignant behavior [18].
Herein, we presented a case of early recurrence of a CNS WHO grade 2 IDH-mutant astrocytoma with high-grade transformation in a young adult after gross total resection. Although this case was deemed to show a low risk of IDH-mutant astrocytoma based on the 2021 WHO classification of CNS tumors, gemistocytic histology should be noted with caution. This case highlights the limitations of relying solely on the most recent WHO classification system for risk stratification. Multiple histopathological characteristics should be incorporated into clinical decision-making.
Go to :
 XML Download
XML Download