

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Kidney stone disease is a common urological condition that affects about 15% of the world's population [1]. In the past few decades, the prevalence of kidney stones in both sexes has been steadily rising due to the drastic changes in lifestyle and dietary patterns, and the increasing number of individuals with obesity and metabolic syndrome, in addition to advances in radiological diagnosis [2]. Kidney stones are usually recurrent with a relapse rate of approximately 50% in 5 to 10 yrs and 75% in 20 yrs [34] The costs associated with diagnosis and treatment place a huge burden on the healthcare system [5]. Moreover, since the workforce population is at high risk, the condition also imposes a considerable burden on society as a whole [6]. Therefore, identifying the modifiable risk factors for kidney stones can help in the formulation of public health policies to prevent kidney stones and reduce the related socioeconomic burden.
Increased dietary fiber intake offers multiple health benefits [78], and improves cardiovascular and cerebrovascular health [9]. A relatively higher intake of dietary fiber was found to lower the risk of obesity, metabolic syndrome, and diabetes [1011], all of which are established risk factors for kidney stones. However, studies on the association between dietary fiber intake and kidney stone risk are few, and the results have been conflicting [12131415]. Furthermore, smaller population sizes have been a common limitation in recent studies examining this association. Therefore, we drew data from the National Health and Nutrition Examination Survey (NHANES) to explore the association between dietary fiber intake and kidney stones in a representative sample of the US population [16]. The results were adjusted for known risk factors to provide additional evidence on the independent effect of dietary fiber intake on kidney stones.
SUBJECTS AND METHODS
Study population
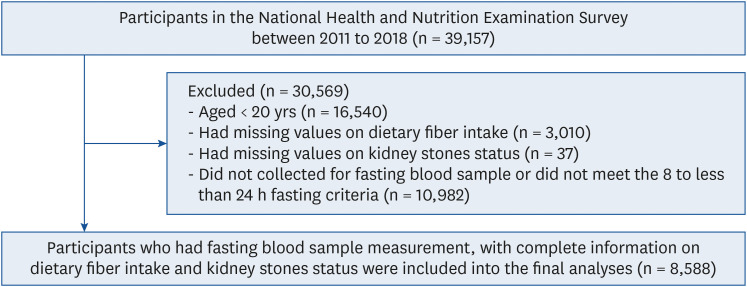
This cross-sectional study utilized data from 4 consecutive NHANES from 2011 to 2018. The surveys are conducted every 2 yrs by the National Center for Health Statistics (NCHS) which operates under the Centers for Disease Control and Prevention, USA. NHANES includes individuals of all age groups who are representative of the general, noninstitutionalized population. The survey applies a stratified, multi-stage, and clustered probability sampling design. It includes structured interviews performed at home, followed by a standardized health examination, including a physical examination, laboratory testing, and a dietary survey. The complete data collection process has been reported earlier [16]. Initially, we included participants recruited from 4 consecutive survey cycles from 2011 to 2018 (n = 39,157). Participants who were younger than 20 yrs of age (n = 16,540), or had missing values on dietary fiber intake (n = 3,010) and kidney stone status (n = 37), did not give fasting blood samples, or did not meet the 8 to less than 24 h fasting criteria (n = 10,982) were excluded from this study. Finally, 8,588 participants were included in the analyses (Fig. 1).
The original survey was approved by the NCHS Ethics Review Board, and written informed consent was obtained from all participants. The present analyses were approved by the Institutional Review Board of Peking University People’s Hospital (approval ID: 2020PHB 125-01).
Data collection
Standardized questionnaires were used to collect data on demographics, education level, smoking and drinking status, physical activities, medical history, and diet. During the participant's visit to the mobile examination center, height, weight, systolic and diastolic pressure were measured using a calibrated instrument based on the standard protocol. The venous blood samples were collected in a subsample of the total participants. The laboratory methods used to measure blood glucose, total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), creatinine, uric acid, blood urea nitrogen (BUN), aspartate aminotransferase (AST), alanine aminotransferase (ALT) and albumin are reported in an earlier study [17].
Evaluation of dietary fiber intake
The information on dietary fiber intake was obtained through 2 24-h diet recall surveys. The first survey was conducted in the mobile examination center, and the second was obtained over 3 to 10 days later through a telephone call. The dietary fiber intake of each participant was calculated based on the Food and Nutrient Database for Dietary Studies maintained by the US Department of Agriculture. Dietary fiber intake was categorized into 3 groups according to the 33.33% and 66.67% percentiles: tertile 1 (fiber intake < 12.1 g/day), tertile 2 (12.1 ≤ fiber intake < 19.1 g/day), and tertile 3 (fiber intake ≥ 19.1 g/day).
Assessment of kidney stone status
The subjects were queried on the health of the kidneys, including kidney stone status, by trained interviewers, using the computer-assisted personal interview system. Participants reported their kidney stone status by responding to the question: “Have you ever had kidney stones?.” Participants who answered “Yes” were defined as having a history of kidney stones [18].
Assessment of covariates
Participants were classified based on sex. Age was analyzed as a continuous variable. Participants were classified according to race and ethnicity as follows: Non-Hispanic white people, non-Hispanic black people, Hispanics, and others. Participants were classified according to the level of education as follows: lower than 12th grade, high school, university level education, or higher. Participants were classified according to their smoking status into ‘never,’ ‘former,’ and ‘current’ smokers. Alcohol consumption of the participants was categorized as ‘not excess,’ and ‘excess’ (≥ 30 g/day for males, ≥ 20 g/day for females). Participants were classified based on the level of physical activities as ‘inactive’ (no moderate-to-vigorous physical activity) and ‘active’ (any moderate-to-vigorous physical activity in a week). Body mass index (BMI) was calculated as the body weight in kilograms divided by the square of the height in meters. It was categorized into non-obese (BMI < 30.0 kg/m2) and obese (BMI ≥ 30.0 kg/m2) according to the cutoff suggested by the World Health Organization [19]. Individuals were identified to be hypertensive if the systolic blood pressure was ≥ 140 mmHg or diastolic blood pressure was ≥ 90 mmHg or if they self-reported hypertension or were taking antihypertensive medication. Individuals were diagnosed with diabetes if their fasting blood glucose was ≥ 7.0 mmol/L, or if they self-reported diabetes or were using antidiabetic drugs. Dyslipidemia was diagnosed based on TC ≥ 6.2 mmol/L, TG ≥ 2.3 mmol/L, LDL-C ≥ 4.1 mmol/L, or HDL-C < 1.0 mmol/L. The estimated glomerular filtration rate (eGFR) was calculated according to the chronic kidney disease (CKD) epidemiology collaboration equation [20], and CKD stage 3–5 was defined as an eGFR < 60 mL/min/1.73 m2 [21]. The total energy intake and water intake were calculated as the average of 2 days of dietary recall data. The choice of covariates in this study was guided by traditional risk factors identified in previous research to influence kidney stone formation.
Statistical analyses
Due to the complex multi-stage (incorporating sample weights, stratification, and clustering) sampling design, proper weighting procedures were applied following the NHANES analytical guidelines. Sample weights were recalculated to merge 8 yrs of total survey data from the NHANES 2011 to 2018. Data are presented as weighted proportions (SE) for categorical variables and as weighted means ± SEs for continuous variables. Weighted logistic regression models were used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs). Model 1 was not adjusted. Model 2 was adjusted for age, sex, race and ethnicity, education level, smoking status, alcohol consumption, and physical activity. Model 3 was adjusted for age, sex, race and ethnicity, education level, smoking status, alcohol consumption, physical activity, BMI, hypertension, diabetes, dyslipidemia, daily water intake, CKD stage 3–5, and total energy intake. Trend tests were conducted by treating the tertiles as continuous variables, which were generated by assigning a median dietary fiber intake value to each tertile. We also treated the dietary fiber intake as a continuous variable to explore the association between every 5 g/day increment in fiber intake and the risk of kidney stones. We explored the shape of the dose-response between dietary fiber intake and kidney stones using restricted cubic splines with knots at the 5th, 27.5th, 50th, 72.5th, and 95th percentile. The model was stratified by important populational and medical characteristics as modifiers: age (< 40 or ≥ 40 yrs), sex (male or female), obesity (yes or no), and diabetes (yes or no). The multiplication interaction terms between these subgroups and the dietary fiber intake were added to a completely adjusted model. Models with and without interaction terms were compared. We conducted the following sensitivity analyses to test the robustness of the results: 1) uric acid, BUN, AST, ALT, and albumin were additionally adjusted into the regression model to minimize the potential for residual confounding; 2) to enhance the practical significance of the research findings, the dietary fiber intake was grouped into the high-level group (> 25 g/day) and the low-level group (≤ 25 g/day), which was consistent with the recommendations of the American Heart Association (AHA) [22].
All statistical analyses were performed using R version 3.6.2. The “survey” package in R was used to account for the survey design analyses of NHANES data. The “rms” package in R was used to conduct logistic regression analyses. The “rms” and “ggplot2” packages were used to perform restricted cubic spline analyses. All the P-values were 2-sided, and the statistical significance was defined as P < 0.05.
RESULTS
Characteristics of participants according to different dietary fiber intake tertiles
The characteristics of the participants are presented in Table 1. The study included 8,588 participants. The mean ± SE age was 47. 7 ± 0.3 yrs and 48.3% were male. In tertiles 1, 2, and 3, the mean ± SE of the dietary fiber intake was 8.4 ± 0.1 g/day, 15.4 ± 0.0 g/day, and 27.4 ± 0.2 g/day, respectively. Compared to participants who had a low level of dietary fiber intake (tertile 1), those with a higher fiber intake (tertile 2 or 3) were more likely to be male, Hispanic, with a higher education level, were less likely to be current smokers, and had a lower prevalence of obesity, diabetes, and CKD stage 3–5 (all P for trend < 0.05).
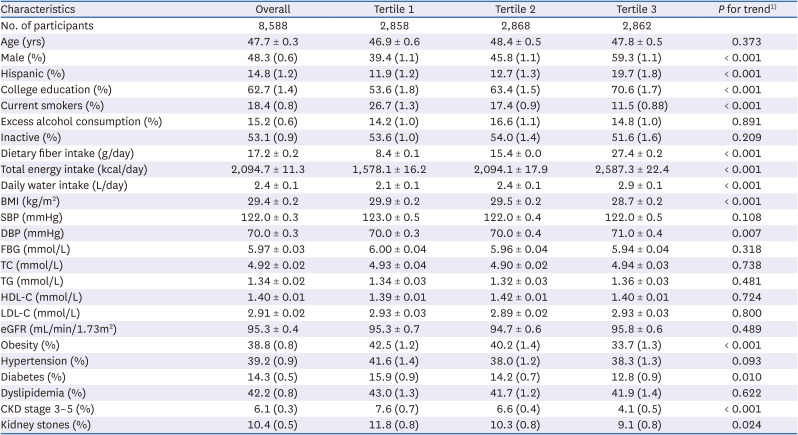
Table 1
Characteristics of the study participants according to their dietary fiber intake
Data are presented as the weighted mean ± SE or weighted prevalence (SE).
1)Trend tests were conducted by treating the tertiles as continuous variables, which were generated by assigning a median dietary fiber intake value to each tertile.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; TC, total cholesterol; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate; CKD, chronic kidney disease.
![]()
A total of 872 participants had a history of kidney stones (weighted prevalence [SE]: 10.4% [0.5%]). The weighted prevalence (SE) of kidney stones in tertiles 1, 2, and 3 was 11.8% (0.8%), 10.3% (0.8%), and 9.1% (0.8%), respectively (Table 1). A significant trend association was found between the dietary fiber intake tertiles and the prevalence of kidney stones (P for trend = 0.024).
Association between dietary fiber intake and kidney stones
The association between dietary fiber intake and kidney stones is presented in Table 2. After adjusting for age, sex, race and ethnicity, education level, smoking status, alcohol consumption, physical activity, BMI, hypertension, diabetes, dyslipidemia, daily water intake, CKD stage 3–5, and total energy intake, individuals with the highest tertile of fiber intake had a significantly lower risk of kidney stones than those in the lowest tertile (OR, 0.68; 95% CI, 0.48–0.95). The corresponding OR (95% CI) for the medium tertile of fiber intake was 0.82 (0.60–1.11). Significant trend associations were observed for fiber intake and kidney stones in the study participants (P for trend < 0.05). Every 5 g/day increment in dietary fiber intake was associated with a significantly lower risk of kidney stones (OR, 0.90; 95% CI, 0.83–0.98).

Table 2
The association between dietary fiber intake and kidney stones
Values are presented as odds ratio (confidence interval).
1)Model 1 was not adjusted.
2)Model 2 was adjusted for age, sex, race and ethnicity, education level, smoking status, alcohol consumption, and physical activity.
3)Model 3 was adjusted for age, sex, race and ethnicity, education level, smoking status, alcohol consumption, physical activity, body mass index, hypertension, diabetes, dyslipidemia, daily water intake, chronic kidney disease stage 3–5, and total energy intake.
4)Trend tests were conducted by treating the tertiles as continuous variables, which were generated by assigning a median dietary fiber intake value to each tertile.
![]()
Fig. 2 shows the results of the restricted cubic spline analyses. A nonlinear dose-response relationship between fiber intake and kidney stones was observed in the study participants (P for non-linearity = 0.025) (Fig. 2).
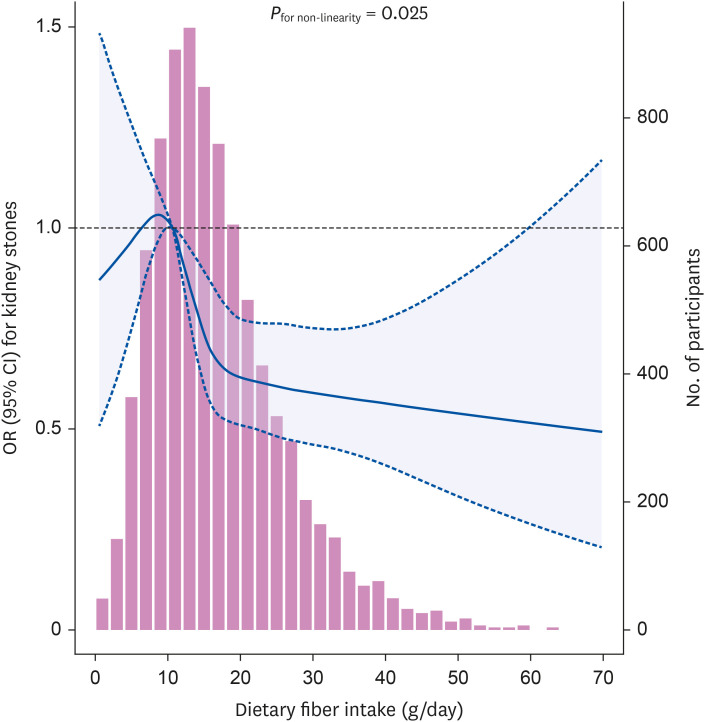
Fig. 2
Dose–response relationship between dietary fiber intake and kidney stones. The solid lines and shaded areas represent the ORs and the corresponding 95% CIs. The models were adjusted for age, sex, race and ethnicity, education level, smoking status, alcohol consumption, physical activity, body mass index, hypertension, diabetes, dyslipidemia, daily water intake, chronic kidney disease stage 3–5, and total energy intake. P-values for non-linearity were obtained using a chi-squared test to compare nested models.
OR, odds ratio; CI, confidence interval.
![]()
In the sensitivity analyses (Supplementary Table 1), the results were largely unchanged when additionally adjusted for serum analytes, including uric acid and BUN. When using the cutoffs of dietary intake recommended by the AHA, the multivariate-adjusted OR (95% CI) comparing individuals with fiber intake > 25 g/day to ≤ 25 g/day was 0.72 (0.52–0.99).
Subgroup analyses are presented in Table 3. No significant interactions were found between dietary fiber intake and sex, age, obesity, or diabetes regarding the risk of kidney stones (all Ps for interactions > 0.05).
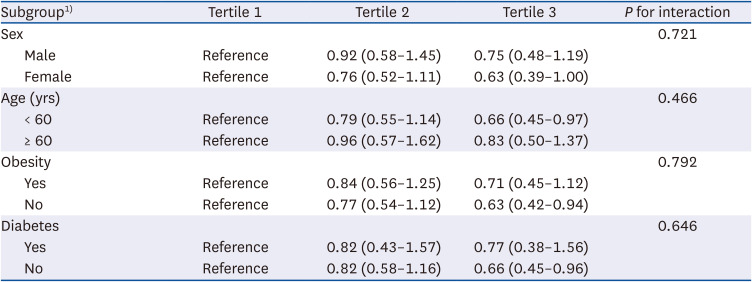
Table 3
Subgroup analyses of the association between dietary fiber intake and kidney stones
Values are presented as odds ratio (confidence interval).
1)Multivariable model was adjusted for age (except for age subgroups), sex (except for sex subgroups), race and ethnicity, education level, smoking status, alcohol consumption, physical activity, body mass index (except for obesity subgroups), hypertension, diabetes (except for diabetes subgroups), dyslipidemia, daily water intake, chronic kidney disease stage 3–5, and total energy intake.
![]()
DISCUSSION
In this study, a high intake of dietary fiber compared to low intake was associated with a significantly lower risk of kidney stones. The association between dietary fiber intake and kidney stones was evident in different subgroups of sex, age, obesity, and diabetes. These findings suggest that, after adjusting for traditional risk factors, dietary fiber intake was an independent predictive factor of kidney stones. To the best of our knowledge, this is the first study using a nationally representative sample to explore the association and the dose–response relationship between dietary fiber intake and kidney stones.
However, we found that the dose–response relationship between dietary fiber intake and kidney stones was non-linear. As the intake of dietary fiber gradually increased from approximately 10 g/day, the risk of kidney stones decreased significantly. When the intake of dietary fiber intake increased from 10 g/day to 15 g/day, the risk of kidney stones decreased dramatically. The risk continued to decline when dietary fiber intake continued to increase over 15 g/day, but the trend of the association was less prominent. These findings suggest that for adults with a dietary fiber intake of approximately 10 g/day, a slight increase in the intake may have an obvious preventive effect on kidney stones. In the study population, the CI of the association between dietary fiber intake below 10 g/day and kidney stones was wide and included the null effect, which may be due to the small sample size in this range of fiber intake.
Few studies have explored the effect of dietary fiber on kidney stones, and the results of these studies have been controversial. Some studies have demonstrated that a fiber-rich diet is associated with an increase in the excretion of oxalic acid which could promote the formation of kidney stones [1213]. However, consistent with our results, a study conducted in the United Kingdom found that fiber intake was associated with a significantly reduced risk of kidney stones (hazard rate [HR] per 10 g/day, 0.82; 95% CI, 0.77–0.87) [23]. A study by Sorensen et al. [14] involving 83,922 postmenopausal women with a self-reported history of the presence of kidney stones found that women in the highest dietary fiber intake quintile (≥ 21.9 g/day) were 22% less likely (HR, 0.78; 95% CI, 0.67–0.92) to report an incident kidney stone event compared to women with the lowest fiber intake quintile (< 10.6 g/day). A study by Turney et al. [15] involving 51,336 adults found that when compared with individuals with a median dietary fiber intake of 13.3 g/day, the HR (95% CI) for incident kidney stones in those with a median dietary fiber intake of 27.0 g/day was 0.72 (0.52–1.00), ssuggesting a lower risk of developing kidneys stones. Consistent with their study, we also found that adults with a fiber intake ≥ 19.1 g/day were associated with a 32% lower risk of kidney stones compared with those with a fiber intake < 12.1 g/day. Moreover, this study found that with every 5 g/day increment in fiber intake, the subject was 10% less likely to develop kidney stones. Of note, we adjusted various traditional risk factors in the multivariate regression model, including age, sex, race and ethnicity, smoking status, alcohol consumption, physical activity, BMI, hypertension, diabetes, dyslipidemia, daily water intake, and total energy intake. Despite this, the association between dietary fiber intake and kidney stones was still significant. Together, these results suggest that an adequate intake of dietary fiber is an independent protective factor against the development of stones.
The AHA recommends a dietary fiber intake of at least 25 g/day for adults to prevent cardiovascular disease [22]. The present study first evaluated the significance of this cutoff point in preventing kidney stones. The risk of kidney stones for adults who achieved a fiber intake of 25 g/day decreased by approximately 30% compared to the reference group. Our results highlight the benefits of adherence to the recommendations of the AHA to prevent kidney stones.
Although many questions remain on the link between dietary fiber intake and the development of kidney stones, there are potential mechanisms that may explain how fiber intake contributes to kidney stone prevention. It has been suggested that calcium oxalate crystals could be mechanically trapped within the fiber network [24]. Through this binding mechanism, the excretion of calcium oxalate crystals increases, which reduces the risk of stone formation [12]. In addition, adequate dietary fiber intake has been proven to reduce the risk of hypercalciuria [1225]. By combining phytic acid with dietary calcium in the intestine, dietary fiber promotes the formation of calcium phytate and increases its excretion [26]. However, foods with a high content of dietary fiber are usually rich in oxalic acid, and an increase in oxalic acid absorption increases oxaluria, which could raise the risk of stone formation. Therefore, prospective studies exploring the underlying mechanisms of the effect of dietary fiber on stone prevention are needed.
The male sex, age, obesity, and diabetes are well-known risk factors for kidney stone disease [24]. This study found no significant interactions between the aforementioned factors and dietary fiber intake in the development of kidney stones. Among males, in participants aged 60 yrs and above, and participants with obesity and diabetes, the observed association between dietary fiber intake and kidney stones included a null effect, potentially attributable to the reduced statistical power caused by the relatively small sample sizes within these subgroups.
The strengths of this study include the analysis of the association in various subgroups, further assessment of the dose–response pattern of the association, and adjustment for confounders such as demographic characteristics, lifestyle information, and comorbidities. However, several limitations should be mentioned. First, recall bias may have been introduced because the assessment of kidney stones was based on the self-reported history in NHANES. However, this method has been proven to be reliable in previous studies, with 97% of the patients who reported having stones being confirmed to have a history of the condition in their medical records [2728]. Second, the causal association between dietary fiber intake and kidney stones could not be evaluated due to the cross-sectional design. Further studies using a prospective cohort design will clarify this causal relationship. Third, unfortunately, the NHANES data did not have information on the composition of kidney stones. Therefore, we could not further explore the association between fiber intake and different types of stones, which may have helped provide valuable evidence and clues to the physiological mechanisms involved in the role of dietary fiber and stones of different compositions.
In conclusion, in this nationally representative population of the US, an increase in dietary fiber intake was associated with a decrease in the risk of kidney stones. These findings suggest that adults who maintain an adequate dietary fiber intake have a lower risk of developing kidney stones. Our results provide evidence of the need for a nutrition management strategy for the prevention of kidney stones. Also, increasing dietary fiber intake should be emphasized in public health policies to prevent kidney stones.
 XML Download
XML Download