

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus is a chronic metabolic disorder that has become a global epidemic [1]. In China, the diabetic population has reached 11.4 million, indicating a substantial escalation of its prevalence over the recent years [2]. Effective and cost-efficient prevention strategies are urgently needed, catering to the needs of public health and clinical practice.
A relationship between total homocysteine (tHcy) and coronary atherosclerotic disease has previously been recognized [23]. Elevated tHcy levels significantly increase the risk of coronary atherosclerotic disease, the leading cause of mortality among diabetic patients [4]. Subsequent studies have shown that individuals with type 2 diabetes are exposed to an elevated risk for cardiovascular disease (CVD) when their tHcy levels are moderately elevated [5]. Given the association between homocysteine and CVD, a potential association between diabetes mellitus and tHcy is plausible. While this relationship has been verified, the outcomes have differed among these studies [678]. For example, the plasma homocysteine concentration is inversely related to type 2 diabetes mellitus in middle-aged and elderly Chinese populations [9]. Therefore, the impact of elevated tHcy levels on the incidence of diabetes within the Chinese population has remained uncertain, given the controversial study findings.
The current study obtained data from the ‘H-type Hypertension Management and Stroke Prevention Strategic International Science and Technology Innovation Cooperation Project’ to investigate the relationship between diabetes mellitus and the tHcy level in rural Chinese people with H-type hypertension.
SUBJECTS AND METHODS
Study design and patient enrollment
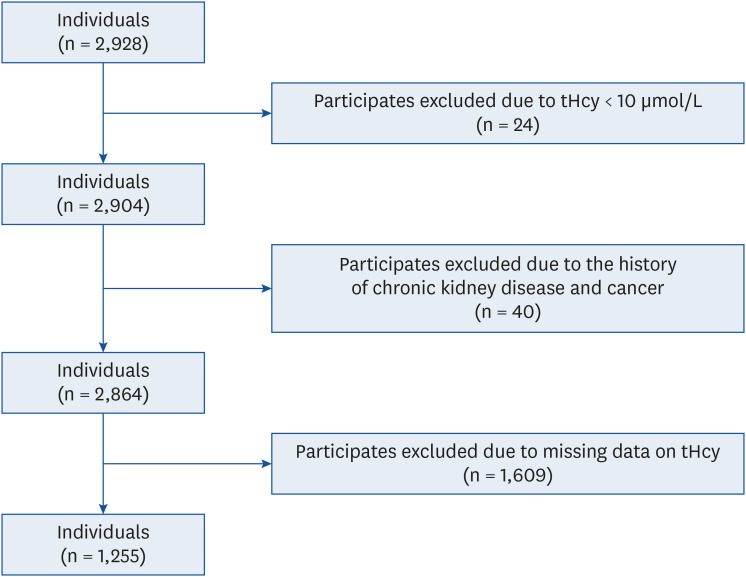
‘H-type Hypertension Management and Stroke Prevention Strategic International Science and Technology Innovation Cooperation Project’ (2016YFE0205400), which was conducted in Yichang City, Hubei Province, from June 9, 2020 to December 23, 2020. This included the following: community screening for high blood pressure; hypertension population in all health centers in Yichang City, Hubei province; Hospital treatment of the hypertension population in Yichang City, county and community of Hubei province; the study recruited 2,928 hypertensive patients who voluntarily participated and provided signed informed consent. The eligibility was determined by a history of hypertension, current anti-hypertensive medication usage, and a blood pressure reading of > 140/90 mmHg. Those with tHcy < 10 μmol/L, a history of chronic kidney disease and cancer, and those with missing glucose data were not included in the final analysis, leaving 1,255 participants (Fig. 1).
Ethics approval
All subjects signed the informed consent, and this study was conducted after receiving approval from the Ethics Committee of the People’s Hospital of Wufeng Tujia Autonomous County, the Fifth People’s Hospital of Yichang, Yidu Hospital of Traditional Chinese Medicine, the People’s Hospital of Zigui County and Zigui County Hospital of Traditional Chinese Medicine (2020-04).
Physical examination, demographic characteristics, and laboratory assays
Trained interviewers conducted face-to-face interviews using standardized questionnaires. Information on the participants’ demographic characteristics, prior medical histories (including those for hypertension, diabetes mellitus, stroke, coronary heart disease, atrial fibrillation, dyslipidemia, chronic kidney disease, and malignancy), family history, smoking history, and drinking history were collected. A physical examination included measurements of the subjects’ height, weight, hip and waist circumferences, systolic blood pressure (SBP), diastolic blood pressure (DBP), and pulse rate. The body mass index (BMI) was defined as weight (kg)/square of height (m2). A 2 mL sample of whole blood was taken from each eligible participant to separate the serum, and the samples were stored in a refrigerator at temperatures ranging from 2 to 8°C. The tHcy level was measured on a Hitachi 7600 automatic biochemical analyzer (Hitachi, Tokyo, Japan) using a rating method.
Outcome
In the study analysis, diabetes mellitus was defined according to the criteria of the American Diabetes Association [10]. A participant was classified as having diabetes mellitus if they met any of the following criteria: fasting serum glucose ≥ 7.0 mmol/L, self-reported physician diagnosis of diabetes mellitus, or use of diabetic medication (insulin or oral hypoglycemic agent).
Statistical analysis
The mean ± SD for continuous variables and proportions (%) for categorical variables were used to present demographic characteristics by diabetes mellitus status. With the covariables adjusted, a generalized linear model was used to fit the smoothing curve between tHcy and diabetes mellitus. Multiple logistic regression models were used to determine the odds ratios (ORs) and 95% confidence intervals (CIs) of the association between the tHcy levels and diabetes mellitus. The dose-response relationship between the tHcy levels and diabetes was also analyzed using a trend test. All the smoothing and regression models were adjusted for sex, age, BMI, SBP, DBP, pulse, smoking status, alcohol drinking status, weekly fruit intake, stroke, coronary heart disease, dyslipidemia, glucose, cholesterol, triglycerides, high-density lipoprotein, and low-density lipoprotein.
Subgroup analyses were conducted to determine if any additional relevant variables could moderate the impact on the association between tHcy and diabetes mellitus. These factors included age (< 60 vs. ≥ 60 yrs), sex (male vs. female), BMI (< 24.77 vs. ≥ 24.77), SBP (< 142.50 vs. ≥ 142.50 mmHg), DBP (< 87.00 vs. ≥ 87.00 mmHg), pulse (< 76.75 vs. ≥ 76.75 bpm), current smoking status (yes vs. no), current alcohol drinking status (yes vs. no), and fruit intake (< 500 vs. 500–1,500 vs. ≥ 1,500 g). The cut points for BMI, SBP, DBP, and pulse variables were their medians.
All statistical studies used R software (version 4.2.1; R Foundation, Vienna, Austria), and a 2-tailed P < 0.05 was considered significant.
RESULTS
Outcome measurement
Table 1 lists the overall characteristics of patients. The mean ± SD age of the participants was 57.87 ± 11.72 yrs old, including 853 males (68%) and 402 females (32%). The age in diabetes patients was significantly higher than in patients without diabetes (59.20 ± 11.18 vs. 57.47 ± 11.84, P = 0.028), and the BMI, pulse, and percentage of dyslipidemia were significantly higher (P < 0.05). On the other hand, the blood pressure in patients with diabetes was significantly lower than in non-diabetics (P < 0.05). The proportions of the smoking or drinking status, history of stroke or coronary heart disease, and weekly fruit intake were similar in the 2 groups (P = 0.244). Compared to non-diabetics, patients with diabetes tended to have higher glucose, cholesterol, triglycerides, and low-density lipoprotein levels, but lower high-density lipoprotein levels. The mean ± SD tHcy level was 18.45 ± 12.15 μmol/L for the overall patients: 19.37 ± 12.95 μmol/L for males and 18.18 ± 11.89 μmol/L for females. The difference in tHcy levels between the 2 groups with and without diabetes was not significant (P = 0.146). When the overall patients were grouped according to the quartiles of tHcy levels (Supplementary Table 1), those with higher tHcy levels were more likely to be found among males (P < 0.001), older group (P < 0.001), CVD patients (P = 0.001), and those with a history of current smoking (P < 0.001) and alcohol consumption (P = 0.001).
Table 1
Characteristics of the study participants by diabetes mellitus
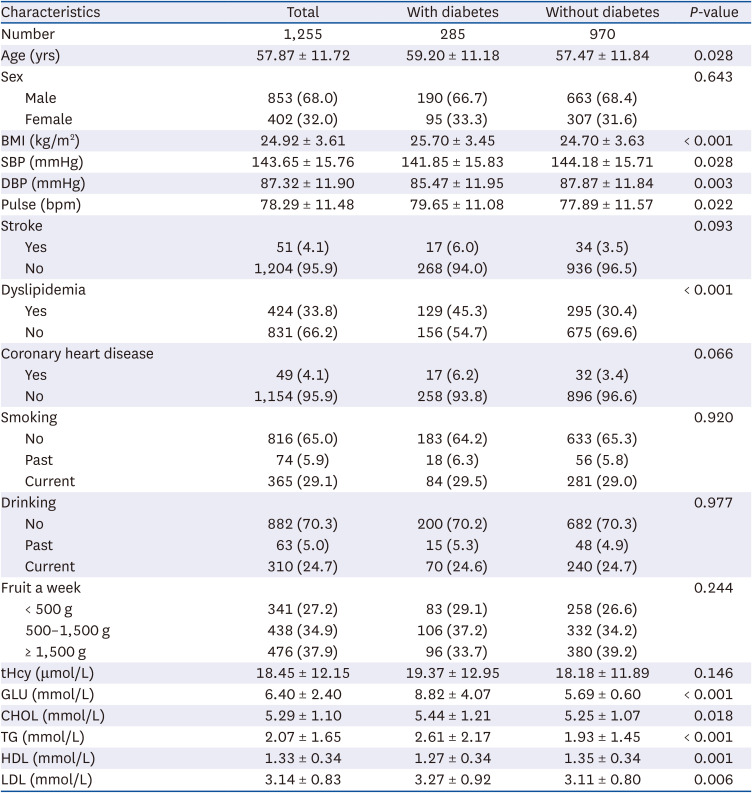
Data are presented as the mean ± SD or numbers (%). Diabetes was defined as a fasting serum glucose ≥ 7.0 mmol/L, self-reported use of hypoglycemic agents or insulin, or physician-diagnosed diabetes. Smoking: smoking at least one cigarette per day, more than 1 yr, or a total of 18 packs/year or more. Drinking: drinking 2 or more times per week on average for more than 1 yr.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; tHcy, total homocysteine; GLU, glucose; CHOL, cholesterol; TG, triglycerides; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Correlation between tHcy and diabetes
Fig. 2A presents a smooth curve of tHcy levels and the OR of diabetes mellitus (adjusted for covariables), and the 95% CI is shown as dashed lines. A significant positive association (per interquartile range increment; OR, 1.17; 95% CI, 1.01–1.35) was observed between the tHcy levels and the OR of diabetes (Table 2). When tHcy was divided further into quintiles, with quintile 1 serving as the reference group (< 12.04 μmol/L). The ORs of diabetes in quintiles 2 (12.04–14 μmol/L), 3 (14.00–16.20 μmol/L), 4 (16.20–20.60 μmol/L), and 5 (≥ 20.60 μmol/L) were 1.39 (95% CI, 0.61–3.18), 1.61 (95% CI, 0.70–3.73), 0.92 (95% CI, 0.37–2.32), and 2.86 (95% CI, 1.22–6.69), respectively. The patients in quintile 5 had a significantly higher risk of diabetes than those in quintile 1 (P = 0.016). Consistently, when tHcy was grouped by 15 μmol/L and 20 μmol/L, a significantly (P = 0.037) higher risk of diabetes was observed in patients in group 3 (≥ 20 μmol/L; OR, 2.03; 95% CI, 1.04–3.96) compared to those of group 1 (< 15 μmol/L).
Fig. 2
Smoothing curves derived from generalized linear models illustrating the association between the tHcy levels (as a continuous variable) and diabetes mellitus, with an adjustment for age, sex, body mass index, systolic blood pressure, diastolic blood pressure, pulse, smoking status, alcohol drinking status, weekly fruit intake, stroke, coronary heart disease, dyslipidemia, glucose, cholesterol, triglycerides, high-density lipoprotein and low-density lipoprotein.
tHcy, total homocysteine.
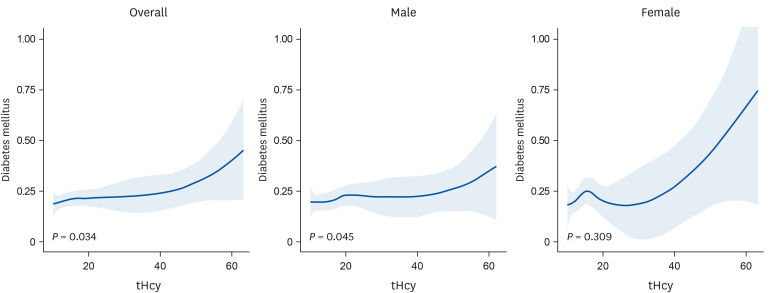
Table 2
Association between tHcy and diabetes mellitus
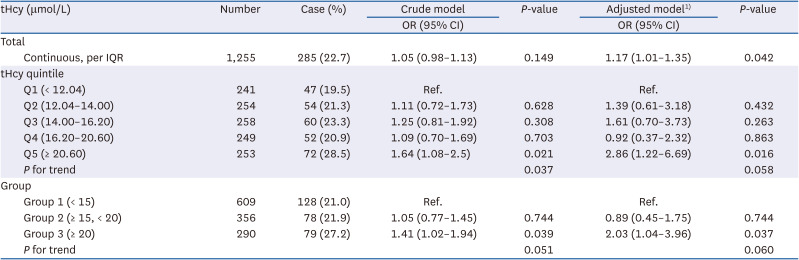
tHcy, total homocysteine; OR, odds ratio; CI, confidence interval; IQR, interquartile range.
1)Adjusted for age, sex, body mass index, systolic blood pressure, diastolic blood pressure, pulse, smoking status, alcohol drinking status, weekly fruit intake, stroke, coronary heart disease, dyslipidemia, glucose, cholesterol, triglycerides, high-density lipoprotein, and low-density lipoprotein.
A similar smoothing curve of the tHcy levels and OR of diabetes was found in males and females (Fig. 2) compared to the overall patients. When the tHcy levels were analyzed according to the groups, the ORs of diabetes in males were 0.62 (95% CI, 0.26–1.48) in group 2 (15–20 μmol/L) and 2.02 (95% CI, 0.90–4.54) in group 3 (≥ 20 μmol/L), compared to those in group 1 (< 15 μmol/L) (Supplementary Table 2). The corresponding results for the diabetes risk in females were also consistent, with an OR of 1.48 (95% CI, 0.47–4.71) for patients in group 2 (15–20 μmol/L) and 1.64 (95% CI, 0.44–6.08) for patients in group 3 (≥ 20 μmol/L) compared with group 1 (< 15 μmol/L) (Supplementary Table 2).
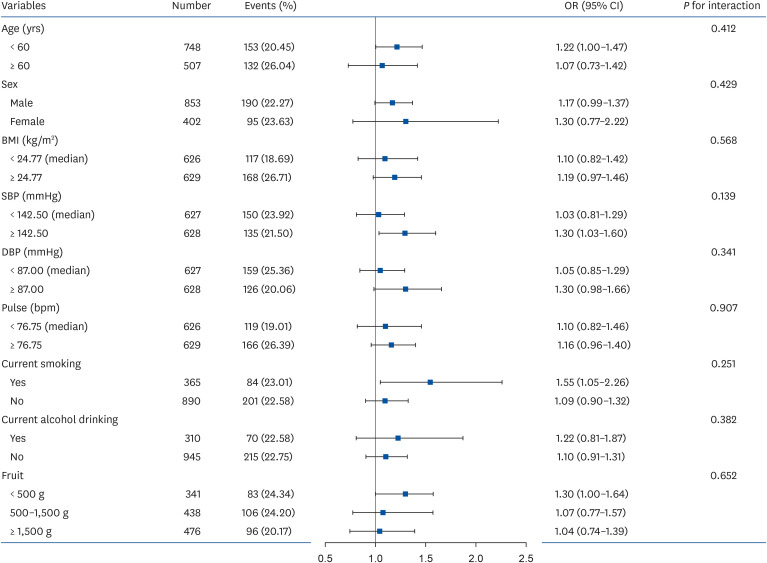
Subgroup analysis
Fig. 3 shows the outcomes of subgroup analyses. None of the following variables investigated significantly modified the relationship between tHcy levels and diabetes mellitus: age (P interaction, 0.412), sex (P interaction, 0.429), BMI (P interaction, 0.568), SBP (P interaction, 0.139), DBP (P interaction, 0.341), pulse (P interaction, 0.907), current smoking (P interaction, 0.251), current alcohol drinking (P interaction, 0.382), and weekly fruit intake (P interaction, 0.652).
Fig. 3
Subgroup analyses on the association between the total homocysteine levels and ORs of diabetes Mellitus with an adjustment for age, sex, BMI, systolic blood pressure, diastolic blood pressure, pulse, smoking status, alcohol drinking status, weekly fruit intake, stroke, coronary heart disease, dyslipidemia, glucose, cholesterol, triglycerides, high-density lipoprotein, and low-density lipoprotein.
OR, odds ratio; CI, confidence interval; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure.
DISCUSSION
The present cross-sectional study revealed a positive association between high-level tHcy and the risk of diabetes, which was independent of conventional cardiometabolic risk factors.
Several studies showed that diabetics have higher tHcy levels than non-diabetics, similar to the present findings [6781112]. On the other hand, some studies reached an opposite conclusion [131415]. One of the 2 studies conducted in China reported a negative correlation between tHcy levels and diabetes risk [9]. In contrast, the other study showed that the tHcy levels were unrelated to diabetes [16]. Ndrepepa et al. [7] reported a higher tHcy level in diabetics than non-diabetics. They also observed a change in this relationship when the population was grouped according to glomerular filtration rate (GFR). In particular, the tHcy levels for the group of non-diabetics are slightly higher than in people with diabetes when with a GFR ≥ 90 mL/min. The relationship between diabetes and the tHcy levels is complex, with the diversity among the populations studied resulting in varied outcomes [481718]. A study conducted in China reported that the current drinking status could significantly affect the relationship between the tHcy levels and the risk of diabetes. A previous clinical study also confirmed that the tHcy levels are higher in the non-drinking population [19], which may be caused by the disturbance of a one-carbon metabolism [20].
Consistent with the results of previous studies [92122], the present study showed high tHcy concentrations in older Chinese males. In the present study, the mean tHcy level in males and females was 19.8 μmol/L and 15.6 μmol/L, respectively. The sex-related differences in the tHcy level may be attributed to the influence of estrogen in females [23]. An epidemiological study reached a similar conclusion that the levels of tHcy in males are higher than in females. On the other hand, incorporating creatinine into the model reduced the observed sex differences in the tHcy levels [21]. In the current study, higher tHcy levels were observed with age, possibly caused by the impaired organ function and reduced metabolic rate [242526]. In addition, the level of tHcy was negatively correlated with fruit intake, and the tHcy levels tended to be higher when the weekly fruit intake was less than 500 g. This result is similar to previous studies. In 2017, a Chinese study showed the potential importance of increasing daily fruit and vegetable intake as a prevention strategy for Hcy [27]. A study conducted on the Serbian adult population in 2020 found that low fruit and vegetable intake was an independent risk factor for hyperhomocysteinaemia (HHcy). Moreover, dark green leafy vegetables are a particularly good source of folate. They reported that adequate folate levels can reduce the risk of HHcy [28]. Dietary folate improves the methylenetetrahydrofolate reductase (MTHFR) C677T genotype-specific status and Hcy levels in plasma folate. In addition, dietary folic acid increases the absorption of vitamins, minerals, and other essential nutrients that effectively reduce the Hcy level [29]. Deficiencies in B vitamins, such as folic acid, may be detrimental to the single-carbon cycle, which leads to Hcy accumulation [30].
A vitamin B12 and folic acid deficiency may contribute to high tHcy levels in diabetes [631]. People with diabetes have lower vitamin B12 and folic acid levels than people without diabetes [611]. Vitamin B12 and folic acid are critical substances involved in the metabolism of tHcy in the body, and their concentrations are inversely correlated with the tHcy levels in the blood [323334]. On the other hand, some studies reported that high tHcy levels were associated with diabetes or diabetes-related complications [12]. Ala et al. [6] reported higher tHcy levels in diabetics and that these levels increased as insulin resistance increased and with inadequate glycemic management. This is also the case in the current study. When the overall patients were grouped according to the quartiles of tHcy levels (Supplementary Table 1), the mean ± SD of glucose in the Q4 group was 6.47 ± 3.59, which was higher than that in the Q1 group with a glucose of 6.34 ± 1.61. That is, patients with higher tHcy levels may also have higher glucose values, even though the causal relationship between high-Hcy levels and hyperglycemia is unknown. Other studies reported high tHcy levels in patients with diabetic retinopathy, diabetic nephropathy, and diabetic peripheral neuropathy [353637].
The most common genetic cause of tHcy is a TT purity of the MTHFR C677T heat-stable variant, a key enzyme in the homocysteine metabolism. MTHFR polymorphisms have been associated with the cardiovascular risk because of the high tHcy levels in TT carriers who are pureblooded, especially when the folate status is abnormal [38]. Dietary folic acid may improve the Hcy levels in males (CC, CT, and TT) and females with the TT phenotype [29]. There is increasing evidence that the plasma tHcy concentrations are influenced by sex steroid hormones, particularly estrogen status in females [21]. Hence, the effect of the tHcy levels on diabetes in different sexes may be due to MTHFR C677T or sex hormones. In the present study, the sex-specific association was not significant.
Some studies have shown that the plasma Hcy levels increase with age [39], possibly due to nutritional deficiencies and decreased renal function in the elderly. The prevalence of impaired fasting glycemia was significantly higher in almost every age group [40]. Some findings have shown a positive correlation between smoking and Hcy concentration [41]. On the other hand, the precise mechanism through which smoking increases the plasma Hcy levels has not been determined, but cigarette smoke may inhibit enzymes, such as methionine synthase (MS) [42], or cause a vitamin B deficiency. The National Health and Health Commission released a report showing that smoking causes damage to vascular endothelial function, leading to atherosclerosis and a variety of cardiovascular and cerebrovascular diseases. Moreover, Hcy can also cause endothelial cell damage. Therefore, smoking may have a synergistic effect with the Hcy levels and lead to diabetes mellitus. Chronic alcohol intake is also associated with increased Hcy levels [43]. Increased alcohol intake also causes impaired intestinal digestion and the absorption of nutrients, decreased hepatic uptake, and deficiencies of vitamin B12, folic acid, and pyridoxal phosphate with increased urinary excretion. In addition, prolonged alcohol abuse can also cause a decrease in the enzyme MS activity of the hepatocytes, which can ultimately increase the Hcy levels.
One study of obese and insulin-resistant rats (a hallmark of type 2 diabetes) reported lower serine and glycine concentrations compared to the controls [44]. Yang et al. [45] reported that serine is the major donor of single-carbon units to the folate cycle through a single-carbon metabolism. The serine metabolism also crosses over to the methionine cycle through the action of MTHFR, which catalyzes the irreversible conversion of 5,10-methylene-THF to 5-methyl-THF. Homocysteine is then remethylated in a vitamin B12-dependent reaction using widely expressed MS. One isotope tracer study showed that most of the methyl groups used for systemic homocysteine remethylation were derived from serine [46]. Therefore, blood glucose can affect the single-carbon metabolism and homocysteine production, which will be verified in future studies.
The present study has several advantages. First, the sample size was 1,255, which was larger than other cross-sectional studies. Thus, the results have more statistical power. Second, compared with similar studies, this study innovatively examined the effects of weekly fruit intake on the relationship between the tHcy levels and the risk of diabetes. Third, an extensive number of potential confounders were adjusted in the multivariate model, minimizing residual risk.
Nevertheless, this study had some limitations. First, the study was cross-sectional; it did not examine whether there was a causal relationship between high tHcy levels and the risk of diabetes. Second, diabetes is commonly known as a metabolic disease with a complex etiology that affects many organs of the body and leads to complications [4748]. On the other hand, the limited information collected in the present study impedes further exploration of whether the changes in the tHcy levels in diabetics mellitus are influenced by diabetes mellitus itself or by its complications. More studies will be needed to probe this question.
In conclusion, this study shows a nonlinear positive association between the tHcy levels and diabetes in rural Chinese hypertensive patients with elevated tHcy levels. The likelihood of developing diabetes mellitus is associated with higher tHcy levels. Moreover, this correlation is unaffected by other tested risk factors. The findings from the present study provide key evidence and insights for further investigation into whether lowering the tHcy levels could prevent the incidence of diabetes mellitus. These findings offer an excellent basis and prospects for further explorations of whether reducing the tHcy levels can prevent the development of diabetes mellitus.
 XML Download
XML Download