

 PDF
PDF Citation
Citation Print
Print


Introduction
Fecal microbiota transplantation (FMT) involves the transfer of fecal microbiota from healthy donors to patients to rectify dysbiosis and restore the functionality of the gut microbiota to a healthy state. FMT is indicated for conditions such as Clostridioides diff icile infection (CDI), inflammatory bowel disease, irritable bowel syndrome, and multidrug-resistant bacterial decolonization. In addition to gastrointestinal disorders, FMT is being applied to a wide range of conditions, including cancer therapy; metabolic, autoimmune, and inflammatory diseases; and neurological and psychiatric conditions [1-3].
Currently, there is growing interest in and perceived necessity for FMT in Korea, particularly indicated for recurrent or refractory CDI and ulcerative colitis [4-6]. Gweon et al. [7] conducted a survey among Korean physicians and reported that 62% of 107 respondents had performed FMT. Of these, 80% expressed their willingness to undergo FMT for CDI, and two-thirds considered it for recurrent cases with at least three recurrences. Notably, 72% of physicians considered FMT for non-CDI diseases when conventional treatments failed, with 97% expressing the need for a stool bank to facilitate FMT. The primary impediment was the absence of regulations and guidelines. In Korea, while blood banks are regulated by the Blood Management Act of the Blood and Organ Policy Division of the Ministry of Health and Welfare, tissue banking is governed by the Ministry of Food and Drug Safety, the absence of a specific legal framework for FMT was noted.
Nonprofit stool banks, such as Microbiotix, aim to provide secure and high-quality fecal microbiota solutions through a standardized banking process, ensuring a consistent supply of microbiota solutions. This enhances the accessibility of this potentially life-saving treatment and provides valuable data to fill the knowledge gaps in FMT and gut microbiota research. Various microbiota banks, including OpenBiome (founded in 2012), operate globally with indications for FMT, including recurrent or refractory CDI, clinical studies on inflammatory bowel disease, graft-versus-host disease, and control of multidrug-resistant organisms.
Donor selection and the implementation of rigorous quality control measures are important to minimize risks and guarantee the therapeutic efficacy of FMT. Despite the critical nature of these processes for the success and safety of FMT, universal guidelines for donor selection and quality control have yet to be established. In this study, the author reviews the guidelines for microbiota banks, focusing primarily on internationally recognized guidelines from the European Consensus Conference (2017)[8] and the International Consensus Conference (2019)[9], as well as the guidelines published in Korea (2022)[10], with particular emphasis on donor assessment. Additionally, the study introduces experiences from operating microbiota bank in Korea.
Guidelines for microbiota bank operation focusing on donor assessment
Donor selection for FMT is primarily focused on screening for potential infections. A consortium of gastroenterology and infectious disease organizations proposed a battery of screening tests including HAV IgM, HBsAg, anti-HCV, HIV EIA, and rapid plasma reagin for serum testing, and C. difficile toxin B (preferably by PCR), stool culture for enteric pathogens, ova, and parasite testing (if history indicates) for stool testing in 2013 [11]. Later recommendations put forward by a European Consensus Conference in 2017 provided a more comprehensive and potentially more expensive strategy [8]. The increased complexity included a preliminary interview to collect medical history, including exposure to infections, high-risk behaviors, and questions about gastrointestinal, metabolic, and neurological disorders as well as antibiotic and proton pump inhibitor therapy.
The blood tests recommended by the European Consensus Conference for screening include cytomegalovirus (CMV), Epstein-Barr virus (EBV), hepatitis A virus, hepatitis B virus, hepatitis C virus, hepatitis E virus, syphilis, HIV-1/HIV-2, Entamoeba histolytica, complete blood cell count with differential, C-reactive protein, erythrocyte sedimentation rate, albumin, creatinine, electrolytes, aminotransferases, bilirubin, gamma-glutamyltransferase, and alkaline phosphatase tests. Testing for human T-lymphotropic virus types I and II antibodies and Strongyloides stercoralis is recommended in specific situations according to the geographical area. In immunosuppressed recipients, CMV IgG, and EBV viral capsid antigen IgG are recommended. Opinions on CMV and EBV screening may differ among readers, particularly in South Korea.
The recommended stool tests proposed by the European Consensus Conference include screening for C. difficile enteric pathogens, such as Salmonella, Shigella, Campylobacter, Escherichia coli O157 H7, and Yersinia. Additionally, screening included vancomycin-resistant Enterococci (VRE), methicillinresistant Staphylococcus aureus (MRSA), gram-negative multidrug-resistant bacteria, norovirus, Giardia lamblia, Cryptosporidium parvum, protozoa (including Blastocystis hominis), helminths, and fecal occult blood tests. Additional stool testing is recommended in specific situations, such as immunosuppressed recipients, detection of Vibrio cholera and Listeria monocytogenes, antigens and/or acid-fast staining for Isospora and Microsporidia, calprotectin, Helicobacter pylori fecal antigen, and rotavirus. However, there are disagreements regarding the routine use of calprotectin measurements. Notably, the specific methods used for each test item were not addressed.
In 2019, the International Consensus Conference updated existing European guidelines proposed by the European Consensus Conference with a simplified list of tests and tighter criteria for antibiotic-resistant bacteria [9]. The guidelines recommend a pragmatic approach to testing given the low percentage of eligible donors and the psychological impact of meaningless incidental findings among healthy donors. The International Consensus Conference recommended blood tests for hepatitis A, hepatitis B, hepatitis C, hepatitis E viruses, HIV-1 and HIV-2, Treponema pallidum, nematodes (S. stercoralis), and complete blood cell counts with differential, creatinine, aminotransferase, and bilirubin levels. The International Consensus Conference recommend stool test items include the following: C. difficile, common enteric pathogens, including Salmonella, Shigella, Campylobacter, Shiga toxin-producing E. coli, Yersinia and V. cholerae, antibiotic-resistant bacteria (including VRE, MRSA, gram-negative antibiotic-resistant bacteria, norovirus, rotavirus, adenovirus, Giardia lamblia, Cryptosporidium spp., Isospora and Microsporidia), protozoa and helminths/va and parasites (including B. hominis and Dientamoeba fragilis), H. pylori fecal antigen (for upper route of FMT delivery). Gram-negative antibiotic-resistant bacteria are specifically described as extendedspectrum β-lactamase (ESBL)-producing Enterobacterales, and carbapenem-resistant Enterobacterales (CRE)/carbapenemase-producing Enterobacterales (CPE). This reflects the recommendations of a recent United States Food and Drug Administration (FDA) alert regarding stool donor screening and testing for multidrug-resistant bacteria. The FDA recommends supplementary screening for multidrug-resistant organisms (MDROs) in stool analyses, based on two prior case reports indicating FMT-associated ESBLproducing E. coli bacteremia [12]. Consequently, MDRO screening has been integrated with evaluation of other viral, parasitic, and bacterial infections.
The emergence and global dissemination of severe acute respiratory syndrome coronavirus 2 (SARSCoV-2), leading to the coronavirus disease 2019 (COVID-19) pandemic, have prompted concerns regarding its presence in stools. Evidence suggests the detection of SARS-CoV-2 RNA and/or the virus itself in the stools of infected individuals, even when respiratory tract samples yield negative results [13,14]. Therefore, screening for SARS-CoV-2 is advisable for both donors and recipients during this pandemic.
A minireview published in 2017 summarized the guidelines [15], emphasizing the lack of complete agreement on screening tests and checkpoints, indicating controversies. Nevertheless, most guidelines agree on ruling out certain infections such as syphilis; hepatitis A, B, C; and HIV. According to most guidelines, stool testing includes C. difficile testing and enteric pathogen cultures. Based on our data, culture-based methods may lack sensitivity for the identification of certain bacterial pathogens in feces. In this study, a realtime PCR platform was used for donor screening. Parasite testing, primarily utilizing enzyme immunoassay platforms, is commonly recommended in various guidelines, mainly using enzyme immunoassay platforms; however, their sensitivity is questionable.
Guidelines for FMT in Korea
In 2022, the Korean FMT guidelines for CDI were published [10]. The Gut Microbiota and Therapy Research Group of the Korean Society of Neurogastroenterology and Motility had a pivotal role in its development, followed by significant contributions from medical societies, including the Korean Society of Gastroenterology, Korean Society of Infectious Diseases, and Korean Society for Laboratory Medicine. These guidelines comprise 18 statements derived from a comprehensive review of 103 scholarly articles.
The Korean FMT guidelines include a table delineating the specific elements for the clinical evaluation of potential donors. These elements were categorized as general questions, inquiries related to infectious/ transmissible diseases, and gastrointestinal queries. Accounting for endemic diseases unique to each country, in addition to addressing common screening parameters, is imperative during donor screening. In Korea, screening for H. pylori infection is recommended, considering the elevated prevalence of gastric cancer.
These guidelines recommend serological and stool tests for donor candidates. For serological testing, viral tests, including screening for hepatitis viruses, HIV, EBV, and CMV, with syphilis as a mandatory exclusion criterion. Furthermore, the guidelines recommend additional blood tests (including routine chemistry tests for calcium, inorganic phosphate, glucose, blood urea nitrogen, creatinine, uric acid, total cholesterol, total protein, albumin, alkaline phosphatase, aspartate transaminase, alanine aminotransferase, serum glutamate-pyruvate transaminase, and total bilirubin), amylase/lipase, C-reactive protein, LDL/HDL cholesterol, triglyceride, antinuclear antibody tests, erythrocyte sedimentation rate, insulin, and a complete blood count.
Recommendations for stool testing provide the targets for screening and specific testing methods. For viral tests, rotavirus, norovirus, adenovirus, and astrovirus are recommended to be tested by reverse transcriptionPCR, and for parasitic tests, Ascaris lumbricoides, C. parvum/hominis, Ancylostoma duodenale, Necator americanus, S. stercoralis, G. lamblia, Entamoeba histolytica, Trichuris trichiura, Clonorchis sinensis, Diphyllobothrium latum, and B. hominis are recommended to be tested by multiplex-PCR. Testing for H. pylori is mandatory, and nest PCR is recommended. Testing is also recommended for bacteria associated with diarrhea, Salmonella spp., Shigella spp., Vibrio spp. Campylobacter spp. (C. jejuni and C. coli), Y. enterocolitica, and Aeromonas spp. were tested using PCR in the stool samples. For multidrug-resistant bacteria, including MRSA, CRE, VRE, and ESBL-producing Enterobacterales, stool culture was the primary test of choice, with PCR performed for CRE and VRE. Additionally, fecal white blood cells and occult blood were assessed.
In addition to serological and stool tests, the guidelines suggest chest radiography as an additional test. The authors also suggested testing for SARs-CoV-2 during the COVID-19 pandemic.
The experience of microbiota bank operation in Korea
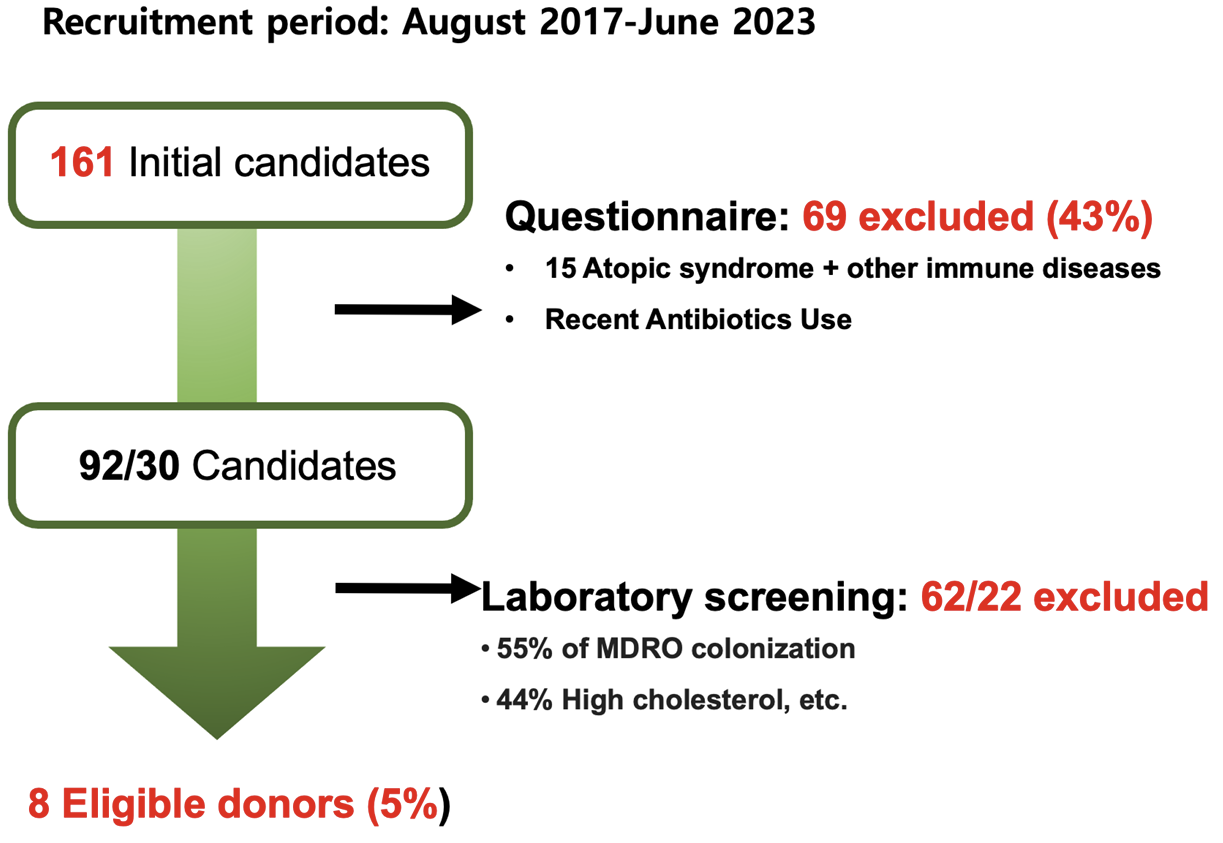
The experience of Microbiotix Inc. in operating a fecal microbiota bank in Korea in 2017 is shown in Fig. 1. A total of 161 potential FMT donors were evaluated between August 2017 and June 2023. Sixty-nine candidates (43%) were excluded during clinical assessments, primarily because of a high body mass index and recent antibiotic use. Of the remaining 92 candidates, 62 (67%) did not meet the laboratory test criteria, resulting in a qualification rate of 19%. Monthly donor requalification identified only eight individuals (5%) as eligible for repeated donations. Notably, a significant prevalence of multidrug-resistant organisms (55%) and high cholesterol levels (44%) were observed among qualified donors. These results highlight the necessity for continuous donor recruitment to avert shortages of donors and FMT materials.
Two studies discussed the treatment of multidrug-resistant bacteria using Microbiotix fecal microbiota products [16,17]. The first paper focused on the prospective use of FMT in 35 individuals carrying CPE and VRE [16]. They observed decolonization rates of 67% and 33% in the upper and lower gastrointestinal tracts, respectively. Furthermore, significant differences in AST and ALT levels were noted between the responders and non-responders. No adverse events were observed. The overall decolonization rates were 53% for VRE and 75% for CPE, with responders and donors exhibiting higher alpha diversity than non-responders. The median time to decolonization was significantly shorter in the FMT group (42 days) than that in the nonFMT group (205 days).
In another study, FMT was performed on ten CPE carriers [17]. They reported an eradication rate of 40% within 1 month and 90% within 10 months. Alpha diversity increased after FMT, which was similar to the pattern observed in CDI. Early responders with eradication within 4 weeks exhibited higher Bacteroidetes and lower Klebsiella levels, suggesting a potential biomarker for predicting FMT response.
Conclusion
FMT requires extensive questionnaires and screening tests to ensure its safety. The screening spectrum is constantly evolving, as observed during the outbreak of Shiga toxin-producing E. coli and enteropathogenic E. coli (EPEC) infections in patients provided with fecal microbiota by OpenBiome in 2019, which prompted product recall. Ongoing discussions regarding the inclusion of EPEC in the screening spectrum persist, because it is not typically detected using microbiological techniques. The future of FMT remains uncertain, with possibilities ranging from continuation to restrictions, and the development of synthetic microbiota preparations. Legislative support is crucial for advancing this field and providing hope and a potential cure for previously incurable patients.
 XML Download
XML Download