

 PDF
PDF Citation
Citation Print
Print


The genus Vanrija was initially characterized by Moore with Vanrija humicola designated as the type species [1,2]. Comprising basidiomycete fungi within the Trichosporonaceae family, Vanrija is widely distributed in the environment but an oppotunistic pathogen in severely debilitated hosts [3]. Among the nine recognized Vanrija species [4], V. humicola has previously been referred to as Cryptococcus humicola, Candida humicola, Cryptococcus humicolus, Torula humicola, Apiotrichum huicola, Azymoprocandida humicola, Mycotorula humicola, or Asterotremella humicola [5]. There is fewer than 10 cases published [2,3,6-9]. Systemic infections of V. humicola occur in immunocompromized hosts, such as central nervous system infections in HIV infected patients or cancer patients in literatures [9]. Until now, the only two reports regarding on urinary isolates were reported available in English [6,10], and there is still no report on a human infection in Korea. At our hospital, a tertiary care hospital in Seoul, Korea, V. humicola has been infrequently detected since it first appeared in 2021. This study therefore aims to elucidate the clinical significance of V. humicola isolated at our hospital.
All yeast isolates of clinical significance identified to species-level using Biotyper MALDI-TOF (Bruker Daltonics). The clinical characteristics of the patients with V. humicola were retrospectively reviewed through electronic medical records. Clinical relevance of V. humicola were evaluated with pathogenicity, infection types, risk factors of acquisition and epidemiological linkage between the cases. This study was approved by the Institutional Review Board of Asan Medical Center (No. 2024-0049) and the requirement for informed consent was waived. Two recent isolates were subcultured on blood agar plate (BAP), potato dextrose agar, and Sarbouraud dextrose agar (SDA) plate and colonial and microscopic growth was observed with incubation at both 25℃ and 37℃. Phenotypic tests were performed using the VITEK2 YST (bioMérieux), API 20C AUX (bioMérieux) and urease test tubes. Sequence analysis was carried for the internal transcribed spacer and D1/D2 regions of the 26S ribosomal DNA. Antifungal susceptibility test was performed using the Sensititre YeastOne YO10 AST (Thermo Fisher Scientific) with visual reading after 48 hours of incubation at 25℃.
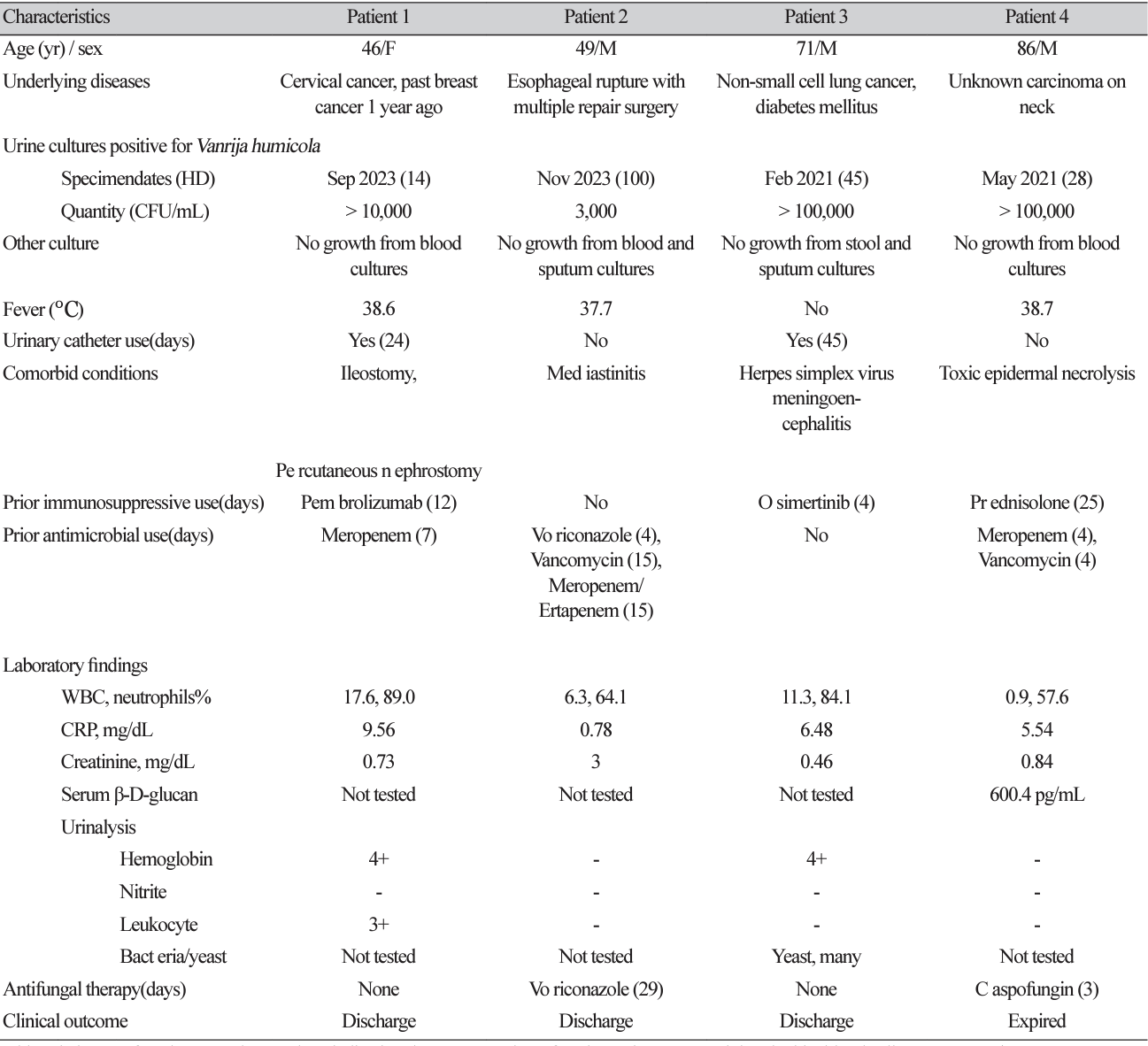
All four cases recovered V. humicola from urine cultures after hospitalization for 14-100 days due to serious underlying and comorbid diseases. None of them did not cluster during hospitalization (Table 1). All except one showed symptoms or signs of cystitis as well as urine cultures produced pure culture of V. humicola > 100,000 CFU/mL. A man with a traumatic esophageal rupture had 3,000 CFU/mL of V. humicola isolated from his urine, and the urine analysis was normal, suggesting that he was colonized with V. humicola. The other three were immunocompromized, of whom two were with cancer chemotherapy and one with pancytopenia and prednisolone treatment. Two indwelled foley catheter for 24 and 45 days, respectively, and developed hematuria. Although one patient received voriconazole due to Candida krusei isolated from mediastinitis sites, the only patient to receive antifungal treatment targeting V. humicola infection was an 86-year-old man with pancytopenia who received 60 mg prednisolone daily for 25 days. The patient was empirically treated with 50 mg caspofungin for three days, but died 4 days after isolation of V. humicola, before the species identification was reported. Three remaining patients were discharged with resolution of chief complaints without any treatment targeted for V. humicola (Table 1).
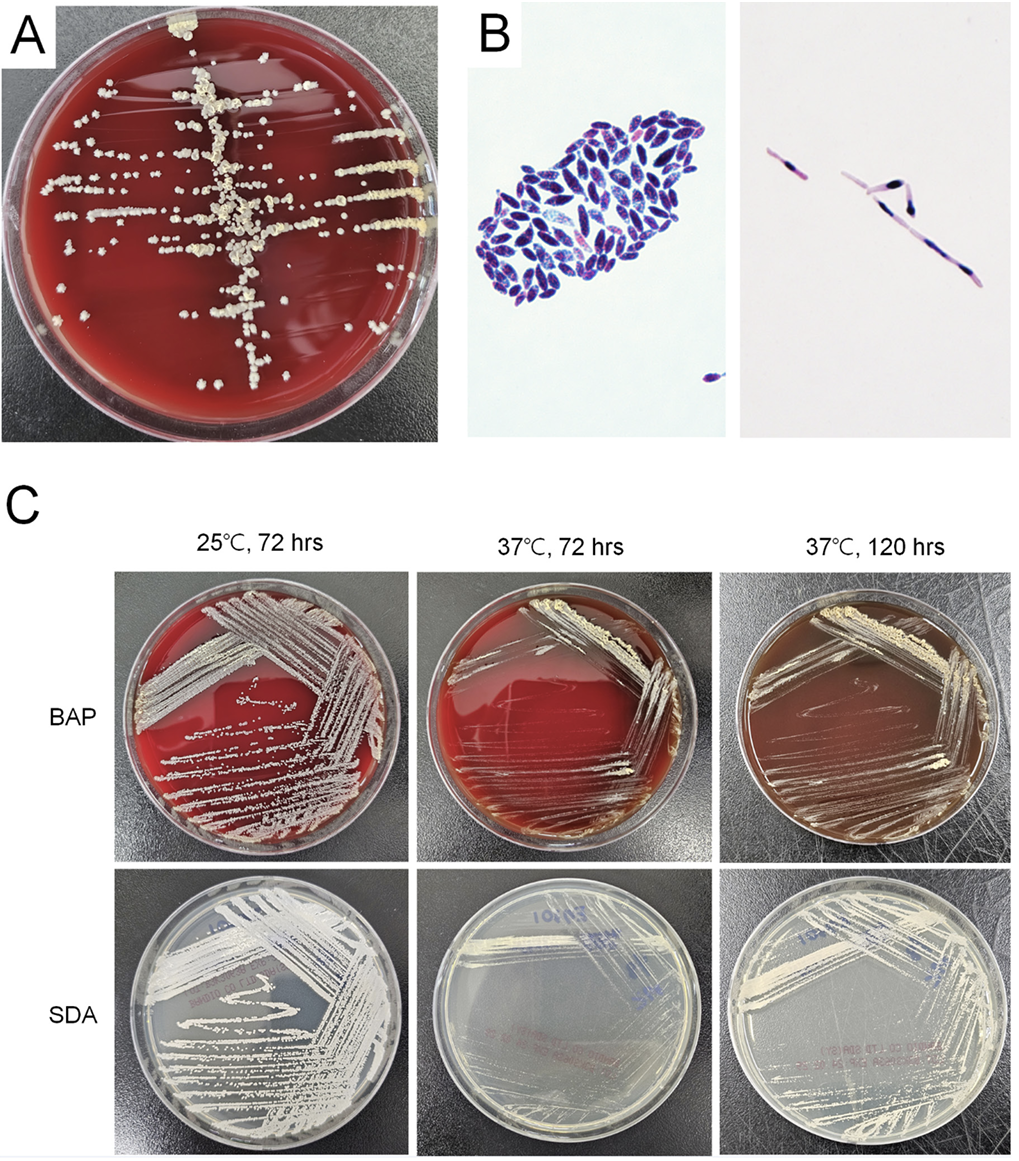
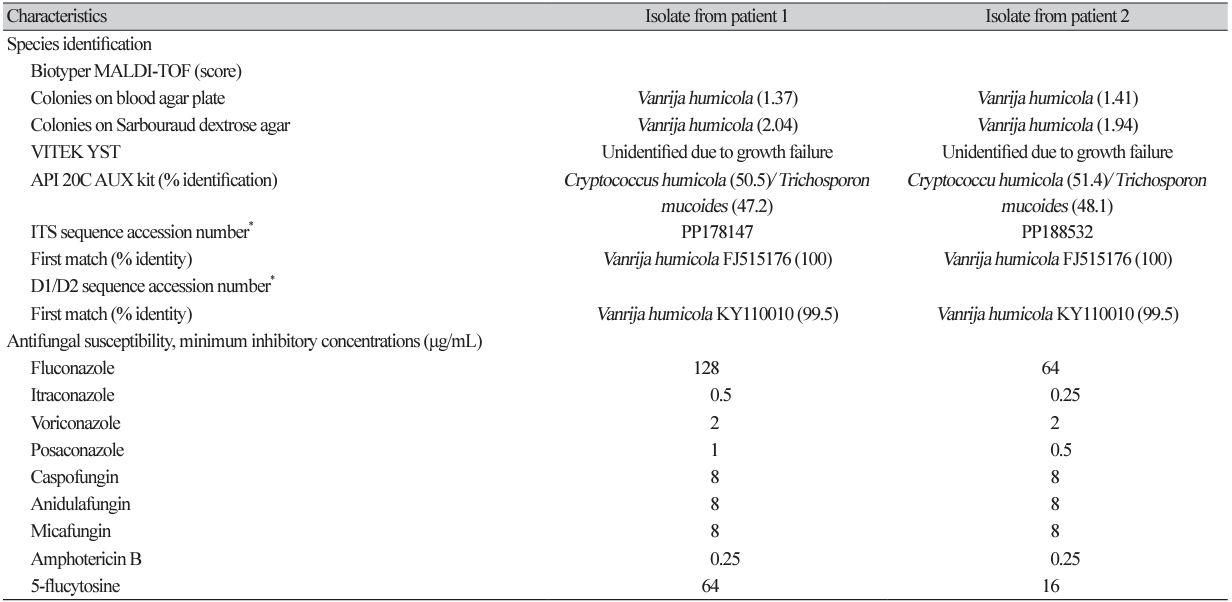
All four isolates were identified to V. humicola first with a score of 1.37 - 1.85 by Biotyper, and ureasepositive when tested using the colonies on BAP. Culture growth of two recent isolates was better at 25℃ than 37℃. With an incubation at 25℃, it presented yellow, dry and cerebriform colonies with a fimbriate margin on day 5. Microscopic examination revealed budding yeasts of oval or ellipsoidal cell with pseudohyphae (Fig. 1). The VITEK2 YST card failed to identify species due to no active reaction, and API 20C AUX identified V. humicola with the first priority but not differentiated from Trichosporon mucoides. The colonies on SDA were better identified with the score values of 1.94 and 2.04, respectively, while those on BAP showed the score values of 1.41 and 1.37, respectively as a score value of Biotyper. Sequence analysis of both isolates yielded excellent identification of V. humicola (Table 2). Antifungal susceptibility of these two isolates showed high minimum inhibitory concentrations (MIC) to fluconazole, caspofungin, micafungin, anidulafungin and 5-FC (Table 2).
V. humicola was first described in 1975 in patients with conjunctivitis and ophthalmopathy [7]. Only two reports on urinary isolates have been published [2,10]. In a case of systemic infection, V. humicola is isolated from the blood, bone marrow, liver biopsy, lymph node, and urine [10]. In this study, all but one funguria of V. humicola were presumed to be a nosocomial urinary tract infection (UTI). Neither of VITEK2 YST or API 20 C identified V. humicola correctly, unlike previous reports where Candida humicola or Cryptococcus humicola were identified using the API 20 C or ID 32 C systems [2,10]. The biochemical profile of API 20C AUX showed that the two highest priority species, V. humicola and T. mucoides, were indistinguishable, which is not surprising given the fact that both species are closely related urease-positive yeasts [11]. Before introduction of MALDI-TOF in routine identification of yeast, this Candida-like yeast is probably underdetected due to relatively slow growth, although colony morphology is pathognomonic when it matured to yellow, dry and cerebriform colonies. Both mass spectrometric analysis and sequence analysis of 26S rRNA showed reliable identification. It is noteworthy that species identification by mass spectrometry was more successful for colonies grown on SDA than those grown on BAP, which is consistent with the previous study on culture yield of fungal keratitis [12]. Therefore, SDA-cultured colonies are preferred for appropriate identification of V. humicola by mass spectrometry.
Though three were compatible with UTI, only one of them treated with antifungal therapy and the other two were uneventful without treatment. Therefore, clinical outcome of V. humicola UTI may not be dependent on appropriate antifungal therapy. This is plausible considering that antifungal therapy is not always warranted for Candida UTI [13]. However, an elderly patient with pancytopenia receiving caspofungin was fatal. Considering that both isolates tested for antifungal susceptibility were resistant to all echinocandins, it was likely that this case was inadequately treated. Only three reports detailing the antifungal susceptibilities of V. humicola have been published to date [6,8,14]. It is susceptible to amphotericin B and itraconazole [6], but consistently resistant to echinocandin and 5-FC [14], like as two closely related genera, Cryptococcus and Trichosporon species, are intrinsically resistant to echinocandin [3]. Of a few fatal cases in previous reports, the isolate from a case with pulmonitis and meningitis showed high MIC across all tested antifungals, including fluconazole, itraconazole, caspofungin, and amphotericin B [8], and a case of meningitis in an AIDS patient is fatal despite fluconazole therapy over a 4-week period [9,10]. Therefore, antifungal susceptibility testing is required for appropriate therapy for the V. humicola infection of critically ill patient.
In conclusion, V. humicola emerged as a pathogen of UTI in Korea. This UTI presented as a nosocomial infection in hospitalized patients with immunocompromised conditions. For funguria of V. humicola, timely species identification based on MALDI-TOF mass spectrometry and antifungal susceptibility testing should be available in a clinical microbiology laboratory.
 XML Download
XML Download