

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Heart failure (HF) in older adults is a complex condition that is strongly influenced by aging, organ deterioration, frailty, and cognitive decline, and considerably impacting outcomes.1)2) The recent focus on malnutrition, frailty, and skeletal muscle issues, such as sarcopenia and cachexia, highlights their critical role in healthcare planning for this population. These conditions frequently overlap and are interrelated. After HF hospitalization, these conditions often lead to prolonged disability, poor quality of life, exercise intolerance, and higher rehospitalization and mortality rates.3)4)5)6)7) This review provides an overview of the epidemiology, assessment methods, overlaps, prognosis, and potential therapies for frailty, sarcopenia, cachexia, and malnutrition in patients with HF.
EPIDEMIOLOGY OF FRAILTY, SARCOPENIA, CACHEXIA, AND MALNUTRITION IN HEART FAILURE
Frailty
Frailty in HF is a state of increased vulnerability due to a decline in physiological reserves, which is often related to aging or the disease itself.8) It manifests with symptoms such as weakness, slow walking, and low physical activity.9) The prevalence of frailty in HF varies widely, mostly because of the different evaluation tools used, with reports ranging from 15% to 74%.10) Frailty is particularly prevalent in older adults, affecting approximately 20–60% of older patients with HF.8) This condition aggravates the burden of HF, leading to more frequent hospitalizations and a decline in the quality of life. Additionally, frailty in patients with HF is associated with increased morbidity and mortality, highlighting the need for early detection and management.10) Notably, the male–female health–survival paradox is evident in HF-related frailty, where women, despite their longer life expectancy, tend to have poorer health than men.11) Women with HF are more likely to experience physical frailty, primarily in terms of symptom severity, whereas physical frailty in men tends to manifest as deteriorating physiological functions.12) This sex disparity highlights the importance of sex-specific approaches in the management of frailty in patients with HF.
Sarcopenia
Sarcopenia, characterized by the progressive and generalized loss of skeletal muscle mass and strength, is a notable complication of HF. Its prevalence among patients with HF is reported to be approximately 34%, although the rates range widely from 10% to 68%, according to a recent study.13) This variation can be attributed to differences in diagnostic criteria, tools used to quantify muscle mass, patient demographics, and HF severity. Age plays a significant role in the development of sarcopenia in HF. This condition is more common in older adults because of age-related physiological changes that exacerbate muscle wasting and weakness associated with HF.14) Older patients with HF are especially susceptible to the negative consequences of sarcopenia, including decreased mobility, higher risk of falls, and diminished quality of life. Additionally, sex-specific trends have been observed in the prevalence of sarcopenia in patients with HF. Studies have shown that sarcopenia is more prevalent in men than in women.15)16) Men with HF tend to experience more pronounced muscle mass loss, whereas women often experience a greater decline in muscle function and strength.17) These sex disparities are likely due to the differences in body composition, hormonal factors, and potentially varying responses to HF therapy.
Cachexia
Cachexia in HF is a severe condition characterized by extensive weight loss and muscle wasting. It affects approximately 10–39% of patients with HF,18)19) particularly in advanced stages and in cases involving congestive right ventricular dysfunction.18) Distinct from sarcopenia, cachexia in HF leads to a reduction in both skeletal muscle and adipose tissue, whereas sarcopenia mainly involves the loss of muscle mass and strength due to aging.20)21) Cachexia in HF is symptomatic in the advanced stage of the disease and is associated with a decline in quality of life and increased mortality rates.19) Management involves addressing nutritional issues and the underlying inflammatory processes.22) Age plays a significant role in the development of cachexia in patients with HF, with older patients being more susceptible to age-related changes and comorbidities that worsen the impact.18) Sex differences have also been observed in the presentation of cachexia in patients with HF. Generally, men are more likely to develop cachexia than women, which could be attributed to sex-specific differences in body composition and metabolism.18) Men typically show a more marked loss of muscle mass, whereas women tend to have higher fat mass, which influences the development and progression of cachexia.
Malnutrition
Malnutrition is a significant concern in HF, driven by factors such as anorexia, malabsorption due to intestinal edema, increased energy demand, and cytokine-induced hypercatabolism. It is prevalent in up to 50% of HF cases and leads to weight loss, muscle wasting, and overall health deterioration.23) The risk of malnutrition is notably influenced by the severity of HF, comorbidities, and socioeconomic status and is particularly heightened in hospitalized patients. In patients with HF, the likelihood of malnutrition increases with the severity of the condition. Age is a crucial determinant in this context; older adults are especially prone to malnutrition due to age-related physiological changes, polypharmacy, and the presence of other chronic conditions that intensify nutritional deficiencies.24) Malnutrition has a severe impact, especially in older adults, with increased morbidity and mortality. Furthermore, sex-based differences have been observed in the prevalence and effect of malnutrition on HF. Women with HF may be at a higher risk of malnutrition, possibly due to longer life expectancy and differences in social and dietary habits compared with men.25) This elevated risk in women may also be associated with higher rates of comorbid conditions, which can contribute to or exacerbate malnutrition.
The interrelated conditions of frailty, sarcopenia, cachexia, and malnutrition significantly influence HF trajectory. Each condition exacerbates the others, leading to a vicious cycle that affects the patient’s health, quality of life, and survival. Understanding these differences and similarities can aid in tailoring more effective and personalized treatment strategies for both men and women with HF. Early detection and multidisciplinary management of these conditions are crucial for improving overall outcomes in patients with HF.
THE EVALUATION OF FRAILTY, SARCOPENIA, CACHEXIA, AND MALNUTRITION IN PATIENTS WITH HEART FAILURE
This section provides an overview of the primary diagnostic methods used to assess frailty, sarcopenia, cachexia, and malnutrition. Notably, no standard diagnostic criteria for these conditions have been established, specifically in patients with HF. The primary diagnostic criteria are listed in Table 1.
Table 1
Main diagnostic tools for frailty, sarcopenia, cachexia, and malnutrition in HF
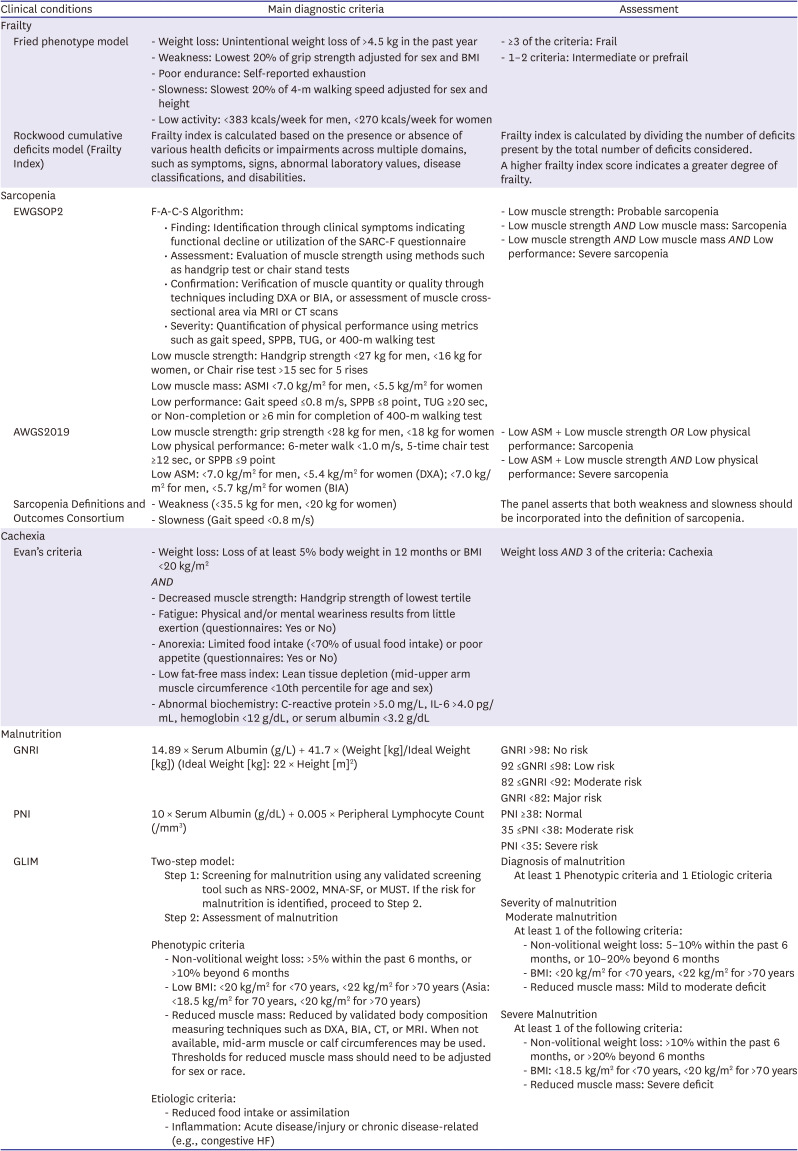
ASM = appendicular skeletal muscle; ASMI = appendicular skeletal muscle index; BIA = bioelectrical impedance analysis; BMI = body mass index; CT = computed tomography; DXA = dual-energy X-ray absorptiometry; GLIM = Global Leadership Initiative on Malnutrition; GNRI = Geriatric Nutritional Risk Index; HF = heart failure; IL-6 = interleukin-6; MNA-SF = Mini Nutritional Assessment-Short Form; MRI = magnetic resonance imaging; MUST = Malnutrition Universal Screening Tool; NRS-2002 = Nutritional Risk Screening-2002; PNI = Prognostic Nutritional Index; SARC-F = screening tool for sarcopenia; SPPB = short physical performance battery; TUG = Timed Up & Go Test.
Frailty
Assessing frailty in patients with HF, although challenging owing to the absence of a specific, universally accepted frailty parameter, is crucial for predicting patient prognosis and guiding treatment decisions. Despite the lack of frailty assessment tools tailored exclusively for patients with HF, alternative methods are available and widely utilized. Two commonly used assessment tools are the Fried phenotype model9) and the Rockwood cumulative deficits model, also known as the Frailty Index.26) The Fried phenotype model is grounded in the evaluation of clinical syndromes based on physical components such as unintentional weight loss, low physical activity, weakness, poor endurance, and slow gait speed. Conversely, the Frailty Index is a comprehensive assessment that accumulates various health deficits over a patient’s life course and provides a broader perspective on overall health status. Although these assessment methods may be complex and have certain limitations in their application to HF, they are invaluable for providing insights into the frailty status of patients. Their use facilitates a more nuanced understanding of the patient’s condition, enabling healthcare providers to tailor their approaches to patient care more effectively. Despite the challenges in frailty assessment in patients with HF, the information gleaned from these tools is instrumental in enhancing patient care and management.
Fried phenotype model: The Fried phenotype model is a widely recognized model for assessing frailty.9) It focuses on five physical domains: unintentional weight loss, low physical activity, weakness, poor endurance, and slow gait speed. The assessment classifies individuals as ‘frail’ if they present with more than three of these domains. Those exhibiting one or two of these domains are considered ‘pre-frail,’ indicating a less severe but still noteworthy level of frailty.
Cumulative deficits model: The cumulative deficits model, namely the Frailty Index, is based on the accumulation of health deficits across a wide range of domains, including symptoms, signs, functional impairments, and laboratory abnormalities.26) The Frailty Index is calculated by summing the number of deficits in an individual. A higher Frailty Index score indicates a greater degree of frailty.
Both methods provide valuable frameworks for assessing frailty although they focus on different aspects of health and functional status. The Fried phenotype model emphasizes immediate physical manifestations, and the Frailty Index offers a comprehensive overview of a person's health deficits over time. These tools are crucial in clinical settings, especially in older adults and those with chronic conditions such as HF, as they help tailor patient care and management strategies.
Sarcopenia
Sarcopenia is recognized as “muscle failure,” characterized by a progressive decline in muscle strength (dynapenia), muscle mass (quantity), and functionality (quality), leading to reduced physical capacity and a higher risk of disability, falls, and mortality.27) The diagnostic algorithms developed by the European Working Group on Sarcopenia in Older People 2 (EWGSOP2) and Asian Working Group for Sarcopenia (AWGS) are the most broadly implemented in clinical settings.28)29)
EWGSOP2 follows the Find, Assess, Confirm, Severity (F-A-C-S) algorithm, emphasizing sarcopenia screening via the self-administered SARC-F questionnaire.28) Progressing from its predecessor, the original EWGSOP,30) which primarily targeted individuals aged 65 and above, the revised criteria expanded the definition of sarcopenia to encompass all age groups. A significant development is the redefinition of sarcopenia as a progressive, systemic skeletal muscle disorder, moving away from its former classification strictly as a geriatric syndrome. Additionally, the concept of pre-sarcopenia, initially characterized by a reduction in skeletal muscle mass and included in the original EWGSOP, was omitted in the EWGSOP2. The updated guidelines prioritize muscle weakness over muscle mass as the primary diagnostic indicator. Consequently, a diagnosis of pre-sarcopenia can be made solely based on muscle weakness. For a conclusive diagnosis, a decrease in skeletal muscle mass is essential, and a reduction in physical function is sufficient to classify sarcopenia as severe.28)30)
In contrast to the EWGSOP, the AWGS proposed in 2019 (AWGS2019) set Asia-specific references for grip strength and skeletal muscle mass, acknowledging the differences in physique and lifestyle compared with Western populations. AWGS2019 continues the methodology of its predecessor, the AWGS, proposed in 2014 (AWGS2014), by maintaining that both skeletal muscle mass and function should be evaluated. However, pre-sarcopenia, defined solely by low skeletal muscle mass and included in the EWGSOP but not in EWGSOP2, was not adopted in AWGS2019 because of its lack of diagnostic value. A key revision from the AWGS2014 criteria is that the diagnosis of severe sarcopenia now demands a combination of muscle weakness, muscle mass loss, and a decline in physical function, thus aligning with the EWGSOP2.29)31)
The Sarcopenia Definitions and Outcomes Consortium (SDOC) is a collaborative initiative funded by the National Institute on Aging and the National Institutes of Health Foundation. This partnership seeks to establish consensus definitions and outcomes of sarcopenia by focusing on community-dwelling adults. It uniquely defines sarcopenia by decreased grip strength and walking speed without an explicit cutoff for these measures. Notably, unlike other consensus definitions, the SDOC does not advocate the measurement of appendicular skeletal muscle using dual-energy X-ray absorptiometry.32)33) The clinical and prognostic implications of sarcopenia as defined by the SDOC criteria are yet to be evaluated.
Cachexia
Many studies on patients with HF have investigated the prevalence and prognostic impact of cachexia. However, their definitions of cachexia were inconsistent, and most of them evaluated cachexia using weight loss and biochemical abnormalities alone.34)35)36)37)38) Only two studies on patients with HF defined cachexia using the Evans criteria, a comprehensive and established assessment tool.19)39) According to the Evans criteria, cachexia is defined by weight loss characterized by the presence of three or more of the following conditions: muscle weakness, fatigue, anorexia, decreased fat-free mass index, and abnormal biochemical profile (C-reactive protein >5.0 mg/L, interleukin-6 <4.0 pg/mL, hemoglobin <12 g/dL, or serum albumin <3.2 g/dL) (Table 1).22) The original Evans criteria defined weight loss as at least 5% decrease from the previous average weight within 12 months and/or a body mass index <20 kg/m2, while Maekawa et al.19) defined weight loss as at least 5% of weight loss within 12 months and/or body mass index <18.5 kg/m2 to account for differences in body size between Asian and Western people.22) This cutoff has not yet been validated, and more studies regarding the components of the Evans criteria are warranted.
Malnutrition
Various methods have been proposed to evaluate the nutritional status; however, no specific methods have been established for patients with HF. Body mass index (BMI) and body measurements including calf circumference and mid-upper arm circumference are readily measurable metrics for estimating nutritional status.40)41) Body composition analysis using dual-energy X-ray absorptiometry or bioelectrical impedance analysis is helpful in assessing fat mass and fat-free mass, which are often used to estimate nutritional condition.42) Regarding biomarkers, albumin or pre-albumin have been widely used in clinical practice; however, recent consensus statements do not recommend these markers to diagnose malnutrition because they do not change in response to changes in nutrient intake.43)44) Therefore, these biomarkers should be used cautiously. Furthermore, multidimensional assessment systems, including the Geriatric Nutritional Risk Index and Mini Nutritional Assessment, are useful for HF.45)
Recently, the first international diagnostic criteria for malnutrition, the Global Leadership Initiative on Malnutrition (GLIM) criteria, was proposed, whereby in patients with diseases associated with inflammation, such as HF, malnutrition is diagnosed based on weight loss over the past 6 months, body mass index, and muscle mass.40) Notably, the criteria did not include biomarkers such as serum albumin.
OVERLAP IN FRAILTY, SARCOPENIA, CACHEXIA, AND MALNUTRITION IN PATIENTS WITH HEART FAILURE
The definitions of these four entities share many common characteristics. Unintentional weight loss is a required diagnostic parameter for cachexia in the Evans criteria,22) while it is one of several components to determine physical frailty proposed by the Fried phenotype model,9) and malnutrition defined by the GLIM criteria.40) Low muscle mass is required to establish sarcopenia and is a possible diagnostic component of malnutrition. Cachexia, as defined by the Evans criteria, requires an underlying chronic/acute disease, which is also a diagnostic criterion for malnutrition. Physical functional impairments, including low gait speed or weak handgrip strength, increase the likelihood of sarcopenia and frailty. Accordingly, these four conditions are sometimes misunderstood or regarded as one another.46)
To the best of our knowledge, no study on patients with HF has investigated the relationship/coexistence of these four entities simultaneously; however, some studies have examined the overlap in two entities. Nearly half of the patients with HF and comorbid sarcopenia have cachexia, while approximately one-third of the patients with cachexia have sarcopenia.36)39) Approximately 40% of outpatients with sarcopenia and HF have frailty, and almost 50% of the frail outpatients have sarcopenia.47) More than 60% of frail patients with HF have malnutrition, and approximately 80% of malnourished patients have physical frailty.48) These results indicate that these four entities are similar but distinct comorbidities in patients with HF.
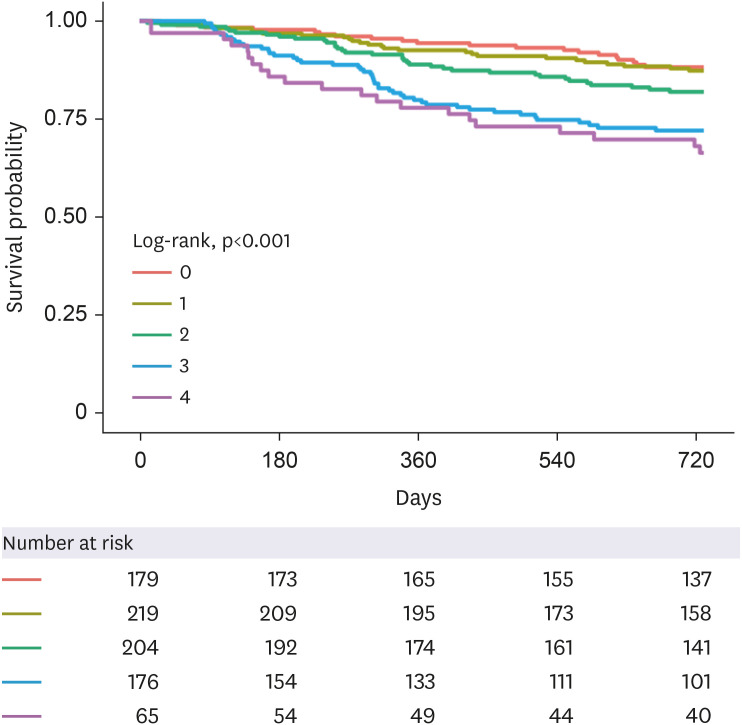
Additional analyses were performed using the data from the FRAGILE-HF registry.49) FRAGILE-HF is a prospective multicenter observational study aimed at assessing the prevalence, interplay, and prognostic significance of physical, social, and cognitive frailty among older patients with HF. In total, the study enrolled 1,332 hospitalized patients with HF aged 65 years or older, who were capable of ambulation upon discharge, from 15 hospitals across Japan.49)50)51) Using the data, we created an overlap diagram, as shown in Figure 1. Our group previously highlighted the significance of multidomain frailty (i.e., physical, cognitive, and social domains) assessed by both the cumulative deficit and phenotypic models49)52); however, physical frailty defined by the Fried phenotype model is regarded as frailty in this analysis to enable the easy understanding of the interaction of these four entities.9) Regarding the other conditions, we defined malnutrition based on the GLIM criteria, cachexia by the Evans criteria, and sarcopenia according to AWGS2019. Of 851 patients aged ≥65 hospitalized for HF who were able to ambulate upon discharge and had no missing data concerning the diagnostic criteria for the four conditions, 469 (55%), 199 (23%), 287 (33%), and 476 (56%) patients had frailty, sarcopenia, cachexia, and malnutrition, respectively. These prevalence rates are consistent with those of our earlier studies.19)49)53)54) The frequencies of the identified conditions were 0, 1, 2, 3, and 4 in 21%, 26%, 24%, 21%, and 8% of the patients, respectively. Notably, this result demonstrated that nearly 80% of the patients have at least one of the four comorbid conditions, all of which were associated with higher mortality. Moreover, the number of identified entities provided prognostic information for predicting all-cause mortality, as shown in Figure 2. Kaplan–Meier analysis also showed that the presence of 0–1 entities was associated with comparatively lower mortality, whereas the presence of 3–4 entities had comparatively higher mortality. These findings suggest that a comprehensive assessment, including nutritional status or body composition, can help identify patients at high risk of mortality among those with HF.
Figure 1
Overlap among frailty, sarcopenia, cachexia, and malnutrition in the FRAGILE-HF study.
This Venn diagram shows the number of overlaps among frailty, sarcopenia, cachexia, and malnutrition using data from the FRAGILE-HF study. A total of 851 patients hospitalized with heart failure were analyzed.
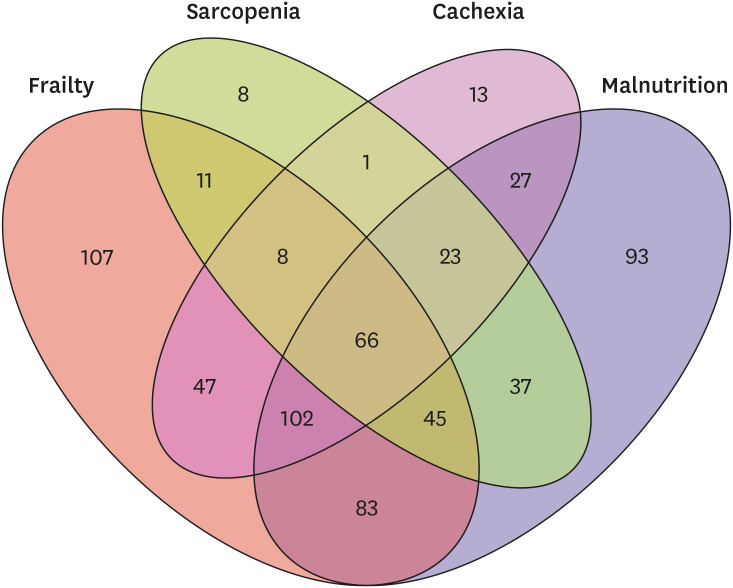
Figure 2
Kaplan–Meier curves for all-cause mortality based on the number of the presence of frailty, sarcopenia, cachexia, or malnutrition.
This figure is illustrated using data from the FRAGILE-HF study. The patients were divided into five groups according to the presence of frailty, sarcopenia, cachexia, and malnutrition.
PROGNOSTIC IMPACT OF FRAILTY, SARCOPENIA, CACHEXIA, AND MALNUTRITION IN HEART FAILURE
Numerous studies have indicated the prognostic significance of these four entities in patients with HF. Herein, we mainly present the results of meta-analyses.
Frailty
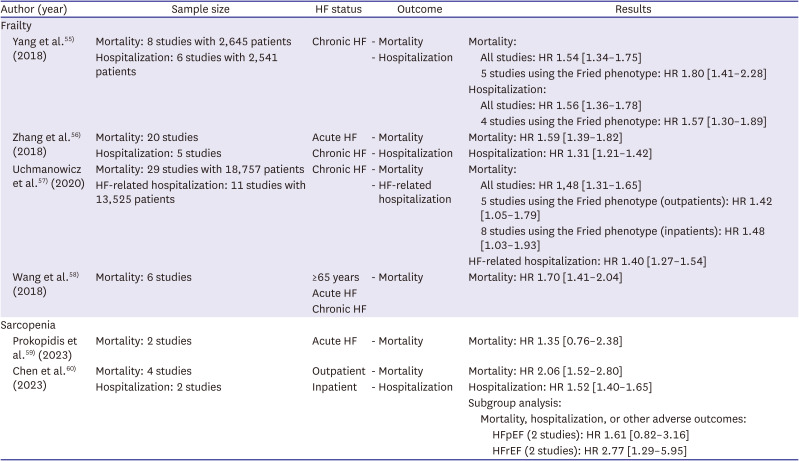
Multiple studies have evaluated the association between frailty and the prognosis of patients with HF. Previous meta-analyses have consistently shown that frailty and HF are significantly associated with increased mortality55)56)57)58) and all-cause hospitalization,55)56)57) respectively. Although these studies used a variety of diagnostic methods for frailty, the results were consistent among studies employing the Fried phenotype model.55)57) A summary of previous meta-analyses of frailty is presented in Table 2.
Table 2
Meta-analyses of the prognostic impact of frailty and sarcopenia in HF
| Author (year) | Sample size | HF status | Outcome | Results | |||
|---|---|---|---|---|---|---|---|
| Frailty | |||||||
| Yang et al.55) (2018) | Mortality: 8 studies with 2,645 patients | Chronic HF | - Mortality | Mortality: | |||
| Hospitalization: 6 studies with 2,541 patients | - Hospitalization | All studies: HR 1.54 [1.34–1.75] | |||||
| 5 studies using the Fried phenotype: HR 1.80 [1.41–2.28] | |||||||
| Hospitalization: | |||||||
| All studies: HR 1.56 [1.36–1.78] | |||||||
| 4 studies using the Fried phenotype: HR 1.57 [1.30–1.89] | |||||||
| Zhang et al.56) (2018) | Mortality: 20 studies | Acute HF | - Mortality | Mortality: HR 1.59 [1.39–1.82] | |||
| Hospitalization: 5 studies | Chronic HF | - Hospitalization | Hospitalization: HR 1.31 [1.21–1.42] | ||||
| Uchmanowicz et al.57) (2020) | Mortality: 29 studies with 18,757 patients | Chronic HF | - Mortality | Mortality: | |||
| HF-related hospitalization: 11 studies with 13,525 patients | - HF-related hospitalization | All studies: HR 1,48 [1.31–1.65] | |||||
| 5 studies using the Fried phenotype (outpatients): HR 1.42 [1.05–1.79] | |||||||
| 8 studies using the Fried phenotype (inpatients): HR 1.48 [1.03–1.93] | |||||||
| HF-related hospitalization: HR 1.40 [1.27–1.54] | |||||||
| Wang et al.58) (2018) | Mortality: 6 studies | ≥65 years | - Mortality | Mortality: HR 1.70 [1.41–2.04] | |||
| Acute HF | |||||||
| Chronic HF | |||||||
| Sarcopenia | |||||||
| Prokopidis et al.59) (2023) | Mortality: 2 studies | Acute HF | - Mortality | Mortality: HR 1.35 [0.76–2.38] | |||
| Chen et al.60) (2023) | Mortality: 4 studies | Outpatient | - Mortality | Mortality: HR 2.06 [1.52–2.80] | |||
| Hospitalization: 2 studies | Inpatient | - Hospitalization | Hospitalization: HR 1.52 [1.40–1.65] | ||||
| Subgroup analysis: | |||||||
| Mortality, hospitalization, or other adverse outcomes: | |||||||
| HFpEF (2 studies): HR 1.61 [0.82–3.16] | |||||||
| HFrEF (2 studies): HR 2.77 [1.29–5.95] | |||||||
Sarcopenia
In contrast to the general notion, the prognostic impact of sarcopenia in patients with HF is controversial considering the available study results. A meta-analysis of two clinical studies showed that sarcopenia was not significantly associated with mortality.59) Another meta-analysis indicated that sarcopenia increased the risk of poor prognosis (mortality, hospitalization, or other adverse outcomes; hazard ratio [HR], 1.64; 95% confidence interval [CI], 1.20–2.25) in patients with HF.60) However, when subgroup analysis was performed, sarcopenia was significantly associated with poor prognosis in those with HF with reduced ejection fraction (HFrEF; HR, 2.77; 95% CI, 1.29–5.95), whereas not in those with HF with preserved ejection fraction (HFpEF; HR, 1.61:95% CI, 0.82–3.16).60) In contrast, data from the FRAGILE-HF study revealed that sarcopenia defined using the AWGS2014 criteria was significantly associated with 1-year mortality, regardless of the type of HF.53) Additional research is required to elucidate the prognostic impact of sarcopenia in patients with HF. A summary of previous meta-analyses of sarcopenia is presented in Table 2.
Cachexia
Data on the prognosis of patients with cachexia and HF are limited. In particular, literature on cachexia diagnosed using a comprehensive assessment is scarce. A retrospective cohort study of 370 patients with chronic HF revealed that those diagnosed with cachexia using the Evans criteria had a 1.89-fold higher risk of mortality.34) Recently, we conducted a sub-analysis of the FRAGILE-HF study.19) In 1306 older patients hospitalized with HF, cachexia assessed using the Evans criteria was independently associated with both cardiovascular mortality (adjusted HR, 1.46; 95% CI, 1.05–2.02) and non-cardiovascular mortality (adjusted HR 1.56; 95% CI, 1.09–2.24).19)
Malnutrition
Although a gold standard assessment tool has not yet been established, malnutrition has consistently been reported to be associated with poor outcomes in patients with HF. Malnutrition, as assessed using the GLIM criteria, is associated with mortality.54)61) Furthermore, previous meta-analyses indicate that malnutrition, as defined by the Geriatric Nutritional Risk Index,62)63)64)65)66) Controlling Nutritional Status score,65)66)67) prognostic nutritional index,65)66)68)69) Mini Nutritional Assessment,62)65) or Mini Nutritional Assessment Short-Form,62)65) is associated with mortality.
Prognostic impact of a combination of the conditions
A combination of these conditions has the potential for a worse prognosis. For instance, patients with malnutrition and frailty exhibited higher mortality rates compared with those with either malnutrition or frailty alone, or with neither48) in patients with acute HF. Moreover, the combination of sarcopenia and cachexia is a significant risk factor for 2-year mortality in patients hospitalized with HF.39) From this perspective, a comprehensive assessment of patients with HF is essential.
INTERVENTION METHODS, INTERVENTION TRIALS, AND RESULTS IN PATIENTS WITH COMPLICATED FRAILTY, SARCOPENIA, CACHEXIA, AND MALNUTRITION IN HEART FAILURE
Given that it is challenging to intervene separately for frailty, sarcopenia, cachexia, and malnutrition, this section explores comprehensive intervention strategies. The clinical presentation of malnutrition varies from loss of appetite and/or weight to severe cardiac cachexia, including the loss of muscle mass in sarcopenia.4)70) Current clinical practice guidelines recommend initiating nutritional support during hospital stay for patients at risk of malnutrition to prevent its adverse outcomes.71)72) However, evidence specific to patients with HF is limited. A notable exception is a preplanned secondary analysis of a randomized multicenter trial in Switzerland that investigated the effect of nutritional support during hospital stay compared with usual care on mortality and other clinical outcomes in patients with HF.73) This study, which involved 645 patients from the EFFORT trial, divided the participants into a group that received personalized nutritional guidance and a control group that received standard hospital meals. The results showed that higher malnutrition severity correlated with increased mortality over 180 days, and personalized nutrition significantly reduced mortality and major cardiovascular events in patients with high nutritional risk compared with standard hospital meals.73) These findings underscore the importance of early nutritional screening and tailored nutritional strategies for this patient group, highlighting their potential for improving survival rates. In addition, it is crucial to explore the role of protein intake in muscle development. Some studies, including one conducted in the United States, have focused on the relationship between protein intake and muscle mass in community-dwelling adults.74) This longitudinal study of community-dwelling older adults found a significant association between dietary protein intake and changes in lean mass, including muscle mass. Participants with higher protein intake, especially from animal sources, experienced smaller losses in lean mass over a three-year period, even after accounting for changes in fat mass. These findings suggest that dietary protein intake is associated with the preservation of muscle mass in older adults, and highlight the potential importance of adequate protein intake in reducing the risk of sarcopenia. Ensuring adequate protein intake may be a modifiable factor to consider when caring for patients with frailty to help maintain muscle mass and overall physical function.74)
Nutrition is not the only intervention to increase muscle mass; muscle training also contributes to improved muscle mass. However, many clinical studies have excluded patients with frailty and muscle training interventions for frailty are scarce. A multicentric prospective observational study conducted in nursing homes in Spain involved 91 institutionalized older adults aged 70 years and above, meeting at least three of the Fried phenotype model criteria.75) They underwent a 12-week intervention that included the daily consumption of two 200-mL bottles of an oral nutritional supplement rich in protein, fiber, vitamin D, and calcium, alongside a standardized physical exercise program. This study found significant improvements in functional status as measured by the Short Physical Performance Battery and Short-Form-Late-Life Function and Disability Instrument, with a substantial percentage of participants showing improvement. Additionally, the participants experienced an enhanced quality of life, increased nutritional status, weight gain, higher body mass index, and improved Mini-Nutritional Assessment scores. These positive outcomes were particularly notable in individuals meeting a higher number of frailty criteria, lower functional abilities, lower vitamin D levels, and poorer nutritional status. The 12-week intervention of oral nutritional supplementation and physical exercise proved effective in enhancing the overall well-being of institutionalized frail older adults.75) Based on the results of these interventional studies, comprehensive interventions such as nutritional guidance and exercise therapy may be essential for patients with HF, frailty, sarcopenia, and cachexia.
Cardiac rehabilitation, which includes these interventions, is a comprehensive treatment option.76)77) However, it is challenging for patients with HF and concomitant frailty, sarcopenia, or cachexia to participate in outpatient cardiac rehabilitation, and few interventional studies have used cardiac rehabilitation as a treatment. Nevertheless, studies have validated the effectiveness of cardiac rehabilitation using modern technology to overcome barriers, such as transportation. Specifically, a study conducted in Japan evaluated the effectiveness and safety of a comprehensive home-based cardiac rehabilitation (HBCR) program for patients with HF and frailty using information and communication technology (ICT).78) Conducted between April and November 2020, it involved 30 outpatients with chronic HF and physical frailty, randomized into a control group receiving standard care and an HBCR group receiving individualized cardiac rehabilitation, including exercise and nutrition guidance via ICT tools like Fitbit®. This study found significant improvements in exercise tolerance (measured by the 6-minute walking distance) and lower extremity muscle strength in the HBCR group, suggesting that individualized ICT-based programs are a safe and effective approach for managing patients with HF and frailty. The use of ICT, including wearable devices and smartphone applications, facilitates patient self-management and regular communication with healthcare providers and contributes to the program’s success.78)
In conclusion, although interventional studies on HF and sarcopenia are limited, efforts are being made in many countries to overcome this problem. However, as noted by Vest et al.,4) clinical research in nutritional therapy may continue to face challenges due to funding issues. Nevertheless, it remains a pressing global issue and we hope that it will continue to be actively addressed.
IMPACT OF FRAILTY, SARCOPENIA, CACHEXIA AND MALNUTRITION ON THE GUIDELINE-DIRECTED MEDICAL THERAPY EFFECTIVENESS
The therapeutic benefits of renin-angiotensin-aldosterone system inhibitors (RAASi), including angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, angiotensin receptor-neprilysin inhibitors (ARNI), as well as beta-blockers and mineral corticoid receptor antagonists (MRA), are well established in the management of HFrEF.79)80) These benefits have been validated in numerous trials and are strongly recommended by clinical guidelines.81)82)83) Recent studies have shown that sodium-glucose cotransporter 2 inhibitors (SGLT2i) are effective in improving patient outcomes across a broad spectrum of ejection fractions.84) However, there is a notable disparity, and mostly a lower rate, in the prescription rates of these HF medications among patients with frailty. Harada et al. observed that physical frailty was significantly associated with the lack of implementation of guideline-directed medical therapy (GDMT), including RAASi and beta-blockers, regardless of factors such as advanced age or severe renal dysfunction.85) Similarly, Sze et al.86) found that frail patients were less likely to receive standard HF medications. Furthermore, Kondo et al.87) reported that the severity of physical frailty was correlated with a decrease in the number of HF medications used. These findings highlight a crucial gap in the management of HF in frail patients and suggest the need for more tailored approaches to ensure optimal treatment outcomes in this subgroup.
Patients with HF-related wasting disorders including frailty, sarcopenia, and cachexia have historically been underrepresented in large clinical trials, often due to advanced age or the presence of multiple comorbidities. This has led to a scarcity of evidence regarding the effect of frailty on the effectiveness of GDMT in this group. We focused on the influence of physical frailty as a comorbidity of HF on the efficacy of GDMT in hospitalized older patients, particularly in those with HFrEF and HF with mildly reduced ejection fraction (HFmrEF). Our findings indicate that the presence or absence of frailty does not significantly alter the association between RAASi and beta-blocker combination therapy and mortality in patients with HFrEF and HFmrEF.88) Kondo et al.87) further explored this subject and found that the suboptimal use of HF medications was associated with a worse prognosis regardless of the severity of physical frailty. These findings underscore the importance of optimizing medication management in patients with HF, including those with frailty, to improve outcomes.
Mechanism of renin-angiotensin-aldosterone system inhibitors and beta-blocker combination therapy
The exact mechanism by which RAASi and beta-blockers affect patients with HF concomitant with physical frailty remains unclear. Onder et al.89) suggested that angiotensin-converting enzyme inhibition may slow muscle strength decline in older women without HF, possibly through effects on inflammation and insulin resistance.90) Beta-blockers may stimulate an anabolic response in skeletal muscles, enhancing protein synthesis, and reducing degradation.90) Additionally, carvedilol enhances skeletal muscle contractility in murine models.91)
Mineral corticoid receptor antagonists in older patients with heart failure
In older patients with HF, the use of MRAs is less frequent than that of other HF medications including RAASi or beta-blockers, with prescription rates decreasing with age.92)93) Despite higher mineralocorticoid receptor activity in older adults,94) indicating the potential for MRA therapy,95) there is limited evidence on the relationship between MRA and frailty. However, a sub-analysis of the TOPCAT trial suggested that the efficacy of spironolactone in patients with HFmrEF and HFpEF was not influenced by frailty severity.96) This highlights the need for careful consideration of MRAs in the management of older patients with HF, particularly those with frailty.
Angiotensin receptor-neprilysin inhibitors in heart failure with reduced ejection fraction
The PARADIGM-HF and ATMOSPHERE studies revealed that ARNIs, which are more effective than enalapril in improving cardiovascular death or HF hospitalization outcomes in patients with HFrEF, were not influenced by frailty.97)
Sodium-glucose cotransporter 2 inhibitors in elderly patients with heart failure
Concerns that SGLT2is, a newer addition to GDMT for HF, may exacerbate frailty due to energy loss have been investigated. A study of older Japanese adults with type 2 diabetes found that SGLT2is led to significant reductions in body weight, fat mass, and total body water, but muscle mass changes and physical function tests (grip test and sit-to-stand test) were not significantly different between the SGLT2i and placebo groups.98) Sub-analysis of DAPA-HF showed consistent benefits of SGLT2is for clinical events and health status in patients with HFrEF without increased discontinuation or serious adverse events due to frailty.99) Similarly, the EMPEROR-Preserved trial demonstrated the efficacy of SGLT2is across a range of frailty severities in patients with HFpEF and HFmrEF.100) The ongoing debate surrounding the use of SGLT2is in frail patients with HF underscores the importance of a cautious and personalized approach to treatment. Current findings indicate that frailty does not significantly affect the efficacy of HF medications; however, more research is needed to fully understand their effects on this specific patient demographic.
Although concerns persist that the presence of frailty may alter the effectiveness of GDMT, some studies have demonstrated its potential efficacy in patients with both HF and frailty. Given the substantial benefits of GDMT in improving the prognosis of individuals with HF, it is vital to consider administering these therapies after considering the challenges faced by frail patients. Cachexia, sarcopenia, and malnutrition may also influence the effects of GDMT in patients with HF; however, no study has explicitly focused on this hypothesis. Although conducting randomized controlled trials in this demographic is challenging, insights from cohort and observational studies are eagerly anticipated. These studies are crucial for enhancing our understanding of and developing more effective and tailored treatment strategies for this vulnerable group of patients.
CONCLUSIONS
The prevalence of frailty, sarcopenia, cachexia, and malnutrition among patients with HF is considerable and is expected to persistently increase with an aging society. It could be hypothesized that recognizing these conditions as early as possible and instituting early interventions may be advantageous. More data, particularly, well-powered large-scale randomized-controlled studies are needed to develop better individualized HF treatment strategies in older patients with HF.
 XML Download
XML Download