

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diabetes significantly increases the risk of a wide array of complications, affecting nearly every organ system in the body.1 The most well-known complications are microvascular conditions like retinopathy, neuropathy, and nephropathy, as well as macrovascular conditions such as cardiovascular disease and peripheral arterial disease. Beyond these, diabetes also heightens the risk of infections, oral health problems, and psychological issues, underscoring the need for comprehensive management strategies.234 Hence, one of the important treatment goals in patients with diabetes is the prevention and delay of these complications.
The relationship between glycemic control and oral health is particularly noteworthy. Oral health issues, such as periodontal disease, are more prevalent and tend to be more severe in individuals with diabetes.5 This is partly because high blood sugar levels can contribute to an environment that supports bacterial growth in the mouth, leading to infections and inflammation.6 Periodontal disease, in turn, can exacerbate diabetes by making it more difficult to control blood sugar levels, creating a bidirectional relationship between diabetes control and oral health.7
Studies have shown that individuals with well-controlled glycemia tend to have a lower incidence of oral health problems compared with those with poor glycemic control.8 Effective glycemic management can mitigate the risk of periodontal disease, as well as other oral health issues like tooth decay, fungal infections, and delayed wound healing in the oral cavity. Moreover, regular dental check-ups and good oral hygiene practices are crucial for individuals with diabetes, as they can help detect and manage oral health problems early, reducing the risk of complications. Diabetes guidelines recommend regular dental check-ups in patients with diabetes.9
Previous studies have established a link between diabetes and oral health; however, most of these studies focused on the presence or absence of diabetes.8 Hence, there is a significant gap in the literature regarding the evaluation of how different levels of glycemic control impact oral health outcomes. Furthermore, there is a notable scarcity of studies focusing on this association, specifically within the Korean diabetic population.10 Therefore, this study aimed to evaluate the association between glycemic control, as measured by glycated hemoglobin (HbA1c) levels, and oral health in Korean patients with diabetes.
METHODS
Study population
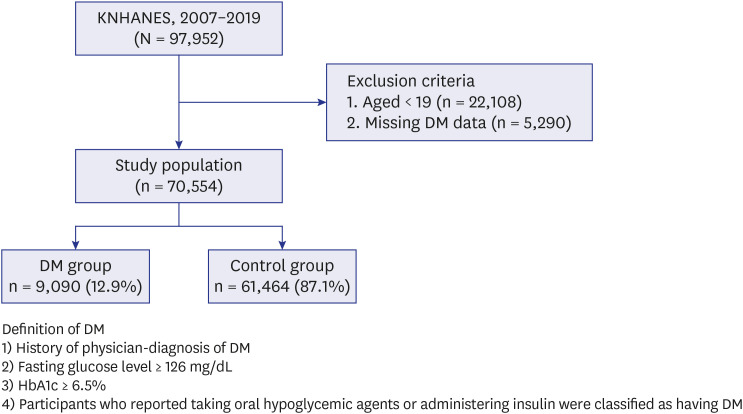
The Korea National Health and Nutrition Examination Survey (KNHANES) is a population-based nationwide survey conducted by the Korea Centers for Disease Control and Prevention. It is designed to measure the health and nutritional status of non-institutionalized individuals in Korea. We used data from the KNHANES IV to VIII (2007–2009, 2010–2012, 2013–2015, 2016–2018, and 2019). The study populations were surveyed based on a stratified multistage sampling method. Participants were divided into those with and without diabetes using KNHANES data for 13 years. Of these (n = 97,952), participants aged 19 years or under (n = 22,108) and with missing diabetes defining variables (n = 5,290) were excluded from the analysis, resulting in a total of 70,554 individuals in the final analysis. The criteria for defining diabetes included any of the following: a physician-confirmed diagnosis of diabetes, a fasting glucose level of at least 126 mg/dL, an HbA1c level of 6.5% or greater,11 or current use of oral hypoglycemic medications or insulin.12 The data included patients with diabetes (n = 9,090) (12.9%) and healthy controls (n = 61,464) (87.1%) (Fig. 1).
Classification of diabetes
The main exposure in this study was diabetes. According to the guidelines of the Korea Diabetes Association, the recommended optimal HbA1c level is less than 6.5% for patients with type 2 diabetes.13 Therefore, in this study, the severity of diabetes was empirically divided according to HbA1c level as good (HbA1c < 6.5% predicted), moderate (6.5% ≤ HbA1c < 8.0% predicted), or poor glycemic control (HbA1c ≥ 8.0% predicted).
Measurements of oral health
Oral health status was evaluated based on the frequency of tooth brushing, the presence of periodontitis, denture usage, the Decayed, Missing, and Filled Teeth (DMFT) index, the number of remaining teeth, and history of dental clinic visit within the last year.
Regarding periodontal disease and oral health-related habits, tooth brushing frequency and dental visit history over the past year were evaluated. The frequency of daily tooth brushing was classified as less than or equal to 2 times/day and more than or equal to 3 times/day.
Periodontitis was evaluated using the World Health Organization (WHO) Community Periodontal Index (CPI).14 The severity of periodontal disease was classified according to the CPI codes 0-4: normal (Code 0), bleeding periodontal tissue (Code 1), presence of calculus (Code 2), shallow periodontal pocket (> 3.5 mm, Code 3), or deep periodontal pocket (> 5.5 mm, Code 4), based on periodontal pocket depth measurements. The index teeth, according to the World Dental Federation (FDI) system, included teeth numbers 11, 16, 17, 26, 27, 31, 36, 37, 46, and 47.15 CPI probes were utilized in compliance with WHO guidelines.14 In this study, Codes 1 and 2 were categorized as normal, whereas Codes 3 and 4 were classified as periodontitis.
Denture use was assessed and classified into three categories: no dentures, removable partial dentures, and complete dentures. Removable partial denture status was defined as wearing denture with one or more remaining teeth, while complete denture status was defined as wearing a denture in an edentulous state.
The DMFT index, which represents oral health status, is calculated by summing the number of an individual’s decayed teeth, missing teeth, and filled permanent teeth.16 Among the methods for evaluating caries, the DMFT index is one of the simplest and most widely used indices in epidemiological investigations.17 The DMFT indexes were assigned with tertiles specified as 0–4, 5–9, and 10 or greater.
The number of remaining natural teeth was evaluated by a trained dentist according to the examination criteria of the National Oral Health Survey. This count included existing natural teeth, excluding third molars, omitted teeth lost due to caries, teeth lost for non-caries-related reasons, and unerupted teeth. This is known as functional dentition because previous studies have suggested that people can chew most of their food when they have more than 20 teeth.1819 The number of remaining natural teeth was divided into three groups: 0–19, 20–27, and 28.20
Other measurements
Body mass index (BMI), calculated as weight (kg) divided by height (m) squared, was classified based on Asian-specific criteria: underweight (< 18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23–24.9 kg/m2), and obese (25.0–29.9 kg/m2).21 Individuals who consumed more than 30 grams of alcohol per day were classified as heavy drinkers. Occupation type was classified into five groups based on the 6th Korean Standard Classification of Occupation: manager, professional, or office worker; service or sales worker; agriculture or fishery worker; skilled labor or machine operator; and manual laborer.22
The presence of comorbidities, including hypertension, dyslipidemia, cardiovascular disease (such as myocardial infarction or angina), osteoporosis, arthritis, and depression, was determined through self-reported physician diagnoses.2324 Hypertension was defined as having a self-reported diagnosis by a physician, taking antihypertensive medication, having a systolic blood pressure of 140 mmHg or more, or having a diastolic blood pressure of 90 mmHg or more.25 Dyslipidemia was diagnosed based on a serum total cholesterol concentration of 6.22 mmol/L or more, a fasting triglyceride concentration of 2.26 mmol/L or more, the use of lipid-lowering drugs, or a self-reported diagnosis by a physician.26
Statistical analysis
All statistical analyses accounted for the complex sample design and survey weights using the SAS survey procedures (version 9.4; SAS Institute, Cary, NC, USA). All data are presented as weighted percentages with standard errors (SE) for categorical variables. Data were compared using the Rao-Scott χ2 test for categorical variables and Student’s t-test for continuous variables. Multivariate logistic regression analysis was performed to assess the association between oral health and glycemic control. Adjusted odd ratios (aORs) and 95% confidence intervals (CIs) were estimated after adjusting for potential confounders. All analyses were adjusted for age, sex, BMI group (underweight, normal, or overweight/obese), smoking history (never and current- or ex-smoker), alcohol consumption (none, light-moderate, heavy), family income (low, high), education, type of occupation, and comorbidities (hypertension, dyslipidemia, cardiovascular disease including myocardial infarction or angina, osteoporosis, arthritis, and depression). All tests were two-sided, and a P value of less than 0.05 was considered statistically significant.
Ethics statement
This study was reviewed and approved by the Institutional Review Board of Chungbuk National University Hospital (approval number: 2024-04-008). The National Health and Nutrition Examination Survey received approval from the relevant Institutional Review Board, and all participants provided written informed consent.
RESULTS
Baseline characteristics
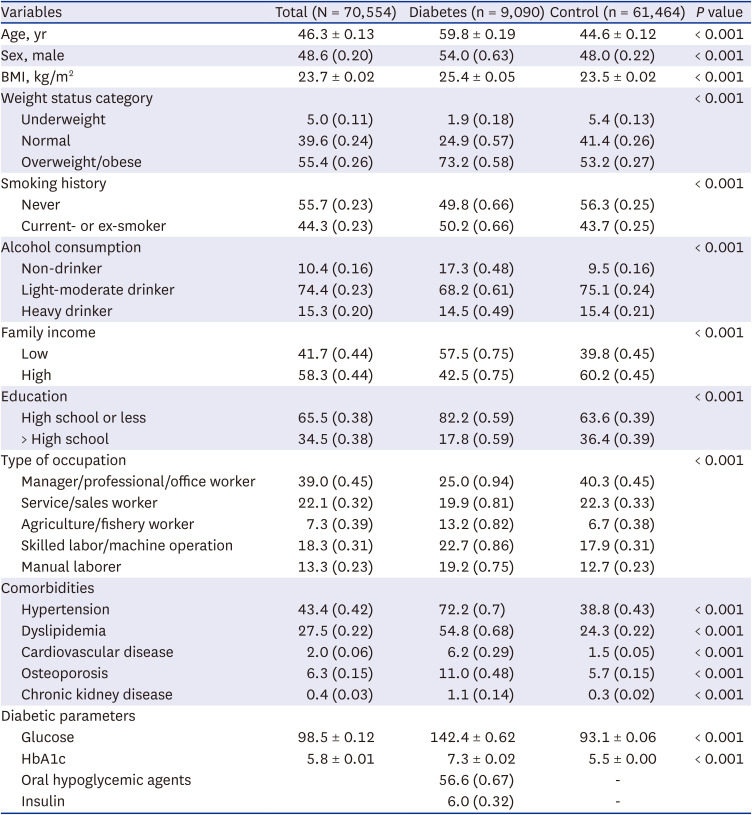
The baseline characteristics of the study population are shown in Table 1. Of a total of 70,554 participants, about 9,090 (12.9%) were allocated to the diabetes group. The mean age and BMI were significantly higher in the diabetes group compared with the control group (59.8 ± 0.19 vs. 44.6 ± 0.12 years and 25.4 ± 0.05 vs. 23.5 ± 0.02 kg/m2, respectively; P < 0.001 for both). The proportion of men was also higher in the diabetes group than in the control group (54% vs. 48%, respectively; P < 0.001). Socioeconomic parameters such as smoking, alcohol consumption, family income, and education showed significant difference between the two groups. The diabetes group had lower family incomes and a lower level of education than the control group (P < 0.001 for all variables). Regarding comorbidities, the diabetes group had a higher proportion of hypertension (72.2% vs. 38.8%, respectively), dyslipidemia (54.8% vs. 24.3%, respectively), and cardiovascular disease (6.2% vs. 1.5%, respectively) than the control group (P < 0.001). In the diabetes group, the mean fasting plasma glucose and HbA1c levels were 142.4 ± 0.62 mg/dL and 7.3 ± 0.02%, respectively. Regarding the type of diabetic managements, about 56.6% of patients were treated with oral hypoglycemic agents and 6.0% were treated with insulin.
Table 1
Baseline characteristics of the study population
Comparison of oral health according to the presence of diabetes
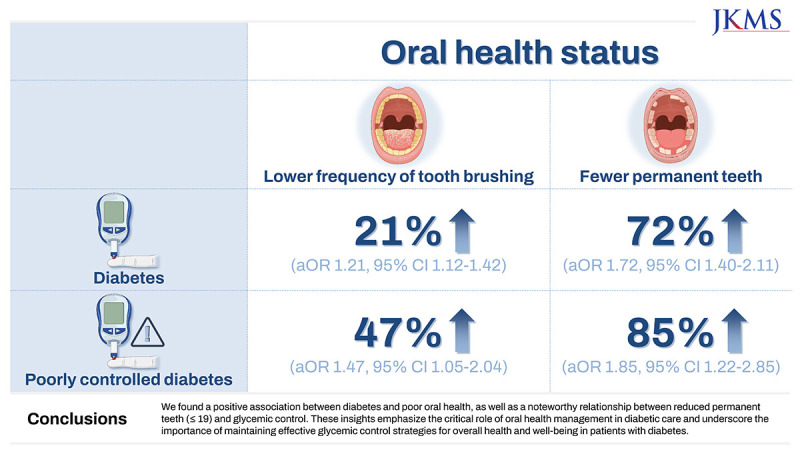
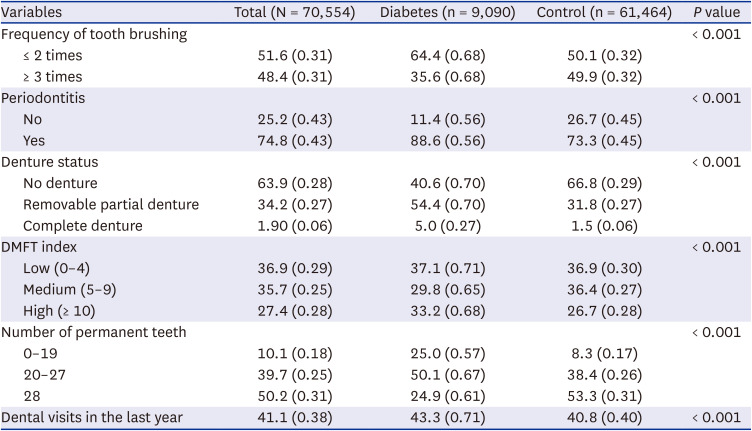
Oral health comparisons between the diabetes and control groups are detailed in Table 2. Relative to the control group, the diabetes group had a lower frequency of tooth brushing (≤ 2 times/day: 64.4% vs. 50.1%) and higher rates of periodontitis (88.6% vs. 73.3%), complete dentures (5.0% vs. 1.5%), and a higher DMFT index (33.2% vs. 26.7%) (P < 0.001 for all variables). The diabetes group had significantly fewer permanent teeth compared to the control group (28 permanent teeth: 24.9% vs. 53.3%, respectively; P < 0.001). Moreover, the diabetes group reported more frequent dental visits in the past year than the control group. (43.3% vs. 40.8%, respectively; P = 0.0004).
Table 2
Comparison of oral health between the diabetes and control groups
Association between oral health and glycemic control
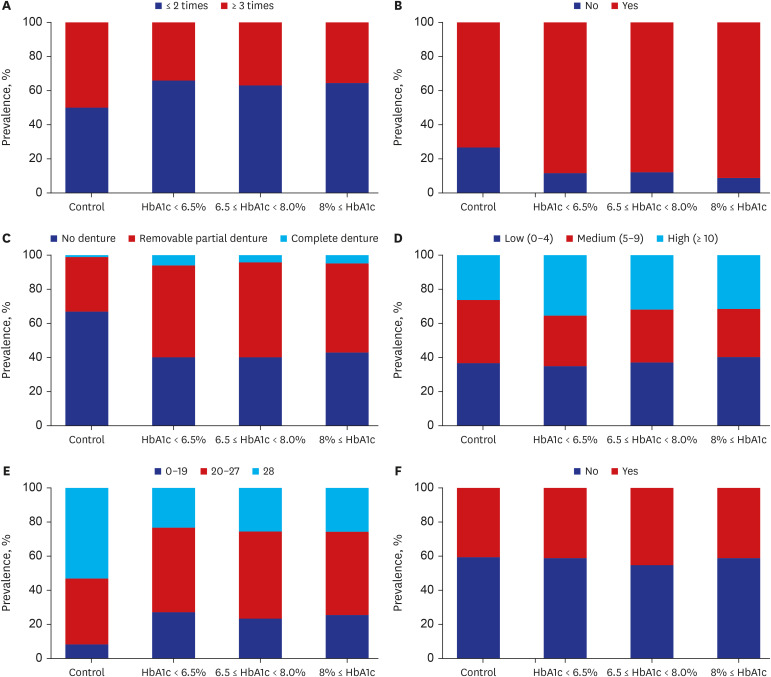
Fig. 2 shows the distribution of dental status in patients with diabetes, categorized based on their glycemic control. As the HbA1c level increased, the prevalence of periodontitis and lower number of permanent teeth showed increasing trends. Other parameters, including frequency of tooth brushing, denture use, and DMFT index, did not show different distributions according to glycemic control in the diabetes group.
Fig. 2
Distribution of dental status in patients with diabetes according to glycemic control. (A) Frequency of tooth brushing, (B) periodontitis, (C) denture status, (D) DMFT index, (E) number of permanent teeth, and (F) dental visits in the last year.
HbA1c = glycated hemoglobin, DMFT = Decayed, Missing, and Filled Teeth.
The multivariate analysis, after adjusting for parameters including age, sex, obesity, smoking history, alcohol consumption, family income, education, type of occupation, comorbidities, oral hypoglycemic agents and insulin is shown in Table 3. A low probability of having no dentures (aOR, 0.784; 95% CI, 0.627–0.979) and a reduced number of existing permanent teeth (0–19: aOR, 1.474; 95% CI, 1.085–2.003) were strongly linked to glycemic control.
Table 3
Adjusted odds ratios and 95% confidence intervals for dental status according to glycemic control
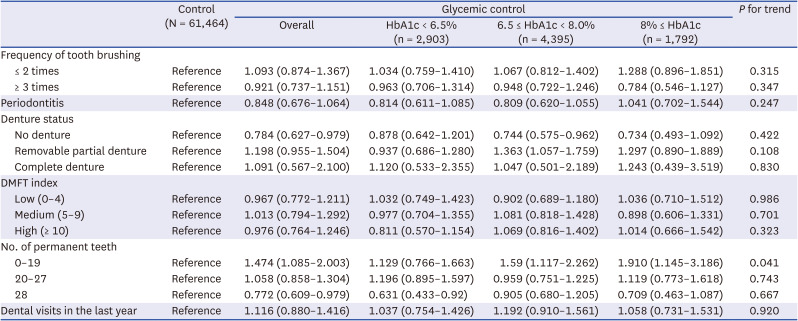
Data are presented as adjusted odds ratios (95% confidence intervals).
All models are adjusted for age, sex, obesity, smoking history, alcohol consumption, family income, education, type of occupation, comorbidities, oral hypoglycemic agents and insulin.
DMFT = Decayed, Missing, and Filled Teeth, HbA1c = glycated hemoglobin.
When compared with the control group, patients with moderate glycemic control were more frequently found to have removable partial dentures (aOR, 1.230; 95% CI, 1.002–1.509). Glycemic control was notably associated with a decreased number of permanent teeth (0–19): in the moderate and poor glycemic-control groups, the aOR was 1.590 (95% CI, 1.117–2.262) and 1.910 (95% CI, 1.145–3.186), respectively (P for trend = 0.041).
DISCUSSION
By analyzing nationally representative data in Korea, the present study demonstrated the association between glycemic control and oral health outcomes in patients with diabetes. Lower tooth brushing frequency and higher rates of periodontitis and complete dentures were observed in the diabetes group compared with the control group. Moreover, the multivariate analysis revealed that poor glycemic control (HbA1c ≥ 8%) was related to fewer permanent teeth.
The association between diabetes and oral health involves intricate mechanisms rooted in hyperglycemia-induced immune dysfunction, chronic inflammation, and alterations in the oral microbiota.272829 Persistent high glucose levels impair immune responses and wound healing, increasing susceptibility to oral infections like periodontal disease and candidiasis. The chronic low-grade inflammation in diabetes exacerbates oral inflammatory conditions, while an altered oral microbiota composition favors the growth of pathogenic bacteria. Additionally, diabetes-related changes in salivary function and impaired wound healing contribute to oral health complications. Notably, the bidirectional relationship between diabetes and oral health underscores the importance of comprehensive dental care and glycemic control in managing oral health outcomes in individuals with diabetes.330
Previous studies have demonstrated the association between diabetes and oral health.6810 In a meta-analysis assessing approximately 20 previous studies, patients with diabetes exhibited poorer oral hygiene and greater severity of gingival and periodontal diseases; however, the extent of periodontal diseases was similar to that of non-diabetics.8 Similar to previous studies, our study showed that patients with diabetes showed poor oral hygiene compared with those without diabetes. However, in contrast to most present studies focused on oral outcomes such as periodontitis, we tried to investigate comprehensive parameters for oral outcomes and behaviors resulting in those outcomes.
It was noteworthy that poor oral health was associated with poor glycemic control in the present study. Some previous studies evaluated oral health according to glycemic control.313233 A previous study demonstrated that the frequency of tooth brushing is linked to a reduced risk of new-onset diabetes, whereas the presence of periodontal disease and missing teeth may elevate the risk of developing new-onset diabetes.34 In a similar context, this study showed a lower frequency of tooth brushing in patients with diabetes, and a lower number of existing permanent teeth was strongly linked to glycemic control. Further, a study in Brazil showed that poor glycemic control in patients with diabetes was related to a higher prevalence of edentulism.31 However, this study assessed glycemic control according to fasting glucose levels, not HbA1c, and only assessed edentulism for oral health in a relatively small number of patients. Another study in the US, using the National Health and Nutrition Examination Survey, showed that flossing habits were related to a lower probability of developing periodontitis and more effective glycemic control.32 This study differs from ours because it focused on the effect of oral behaviors like flossing on glycemic control. The results from the meta-analysis, defining uncontrolled diabetes as an HbA1c level of more than 9% or a fasting plasma glucose level of more than 126 mg/dL, indicated that poor glycemic control correlated with a higher prevalence of coronal caries as well as a higher DMFT mean than controlled diabetes.33
However, in the present study, periodontitis did not show a significant correlation with glycemic control. Chronic periodontitis is classified into slight (clinical attachment loss: 1–2 mm), moderate (clinical attachment loss: 3–4 mm), and severe (clinical attachment loss ≥ 5 mm) based on the amount of clinical attachment loss according to disease progression.3536 However, during a clinical diagnosis, it is difficult to subdivide the diagnosis into slight, moderate, and severe chronic periodontitis because the chronic periodontitis code integrates all these into one. Therefore, this study investigated a broad spectrum of periodontitis without classifying it, which may have diluted the results. Nevertheless, the correlation between poor glycemic control and tooth brushing frequency and the number of remaining permanent teeth was found to be significant. It implicates that lower tooth brushing frequency results in the accumulation of plaque, causing periodontal disease to worsen, which eventually leads to tooth loss. Therefore, the significant results of these two factors may indicate a correlation between plaque control and diabetes.
One notable strength of this study is its utilization of KNHANES data, which enabled the inclusion of a large population in the analysis and comprehensive assessment of oral health outcomes. Moreover, the investigation focused on glycemic control, an important factor in patients with diabetes. However, this study also has a few limitations. First, the study was conducted using a representative sample from Korea, which may limit the generalizability of our findings to other ethnic groups or populations. Second, it is challenging to validate causality due to the cross-sectional nature of the data. Finally, as previously mentioned, variations in the definition of parameters, such as periodontitis, among physicians may have impacted the results, highlighting a potential source of bias. Future research involving various ethnic groups and longitudinal studies is warranted to validate our results.
In conclusion, this study demonstrated a significant association between diabetes and poor oral health status. Additionally, having fewer permanent teeth (≤ 19) showed a significant correlation with glycemic control. Consequently, physicians managing patients with diabetes should emphasize oral health and strive to maintain optimal glycemic control.
 XML Download
XML Download