

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Antiplatelet therapy is one of the main pharmacotherapies in patients undergoing coronary revascularization. Antiplatelet agents reduce ischemic events including stent thrombosis and recurrent myocardial infarction (MI) but increases bleeding risk especially with a use of multiple antithrombotic agents.123 During the past years, therefore, clinical trials have focused on the minimal duration of multiple antiplatelet agents use after coronary revascularization.45
Atrial fibrillation (AF) is the most common important arrhythmia in clinical practice with a reported prevalence up to 12% in patients undergoing percutaneous coronary intervention (PCI).67 When a patient undergoes PCI and has AF with one or more risk factors, triple antithrombotic therapy including oral anticoagulant (OAC) and dual antiplatelet agents is required to prevent both thromboembolic events related with AF and ischemic coronary events. However, since triple antithrombotic therapy carries a high risk of bleeding,123 de-escalation of antithrombotic therapy is recommended after peri-PCI period considering bleeding and ischemic risks.8910
When patients have AF requiring anticoagulation and have a history of PCI, a remaining but important issue is to determine the intensity of antithrombotic therapy beyond 1 year after PCI. Observational studies have reported that compared with OAC plus antiplatelet agents, OAC alone has the advantage in reducing the risk of bleeding with similar efficacy.111213 In a recent randomized controlled trial, rivaroxaban monotherapy was noninferior to combination therapy of rivaroxaban and a single antiplatelet agent for efficacy and superior for safety.14 However, that trial included patients without a history of revascularization, and its findings were not supported by another trial.15
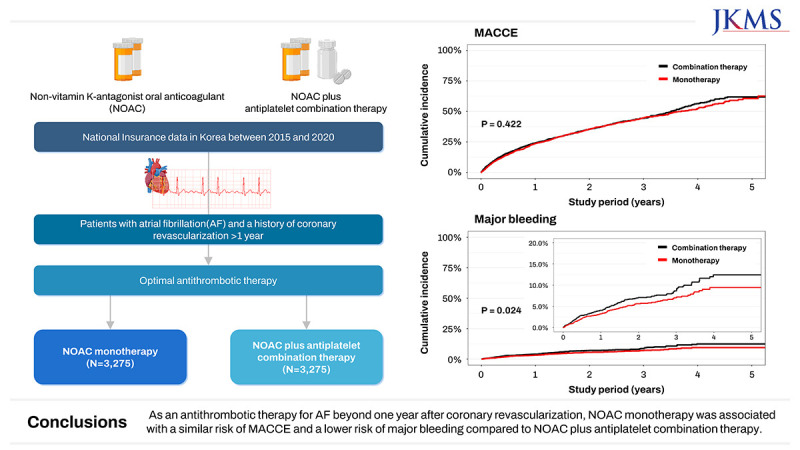
In the present study, therefore, we compared non-vitamin K-antagonist oral anticoagulant (NOAC) monotherapy with NOAC plus antiplatelet combination therapy for the optimal antithrombotic therapy beyond 1 year after coronary revascularization, using real world data from the Korean nationwide registry.
METHODS
Study setting and data sources
This cohort study obtained data from the Korean National Health Insurance Service (K-NHIS) database. The K-NHIS covers approximately 97% of Koreans, while the 3% of remaining Koreans who cannot afford national insurance are covered by the Medical Aid Program.16 Therefore, the K-NHIS database represents the entire population of South Korea and contained national records of all covered inpatient and outpatient visits, procedures, and prescriptions. The NHIS data includes modules on insurance eligibility and medical treatment. The insurance eligibility module contains information on age, sex, residential area, and income level. The medical treatment module contains information on treatments, including diseases and prescriptions.17
We created a cohort of all patients with AF (International Classification of Diseases [ICD] code: I48) aged 20 years or older who had had a history of coronary revascularization (PCI or coronary artery bypass graft). Then we selected patients who had received any NOACs (rivaroxaban, apixaban, dabigatran, or edoxaban) for at least 30 days beyond 1 year after revascularization between January 1, 2010 and December 31, 2020 (n = 5,962).
Measurements
NHIS claims for inpatient and outpatient visits, procedures, and prescriptions were coded using the ICD, 10th Revision.18 As the NHIS routinely audits the claims, such data are considered reliable and used in numerous peer-reviewed publications.1920 In a validation study, the accuracy of diagnosis of MI in NHIS data was 93%.21
The primary efficacy end point was major adverse cardiac and cerebrovascular events (MACCEs) defined as a composite of all-cause death, MI, and stroke. Vital status and cause of death were obtained from death certification collected by the Statistics Korea at the Ministry of Strategy and Finance of South Korea.19 The secondary efficacy end points were individual components of primary end point, and repeat revascularization. The safety end point was major bleeding, defined as intracranial bleeding or gastrointestinal bleeding requiring hospitalization (Supplementary Table 1).
Study exposure was monotherapy of NOAC vs. combination therapy of NOAC plus antiplatelet agent beyond 1 year after revascularization. Patients were defined as the monotherapy group if they had not received any antiplatelet agents for the next 90 days from NOAC treatment according to previous study,22 and as the combination therapy group otherwise.
Baseline characteristics included age, sex, and comorbidities (MI, stroke, hypertension, venous thromboembolism, thrombosis, chronic obstructive pulmonary disease, liver disease, diabetes, renal disease, cancer, alcohol abuse and anemia). Comorbidities were defined by diagnosis codes, prescription records, and inpatient and/or outpatient hospital visits within 1 year before the index date (Supplementary Table 1). The CHA2DS2-VASc score was calculated by assigning 2 points each for 75 years or older age, and previous stroke, transient ischemic attack, and/or systemic thromboembolism, and 1 point each for 65 to 74 years of age, female sex, heart failure, hypertension, diabetes, and vascular disease (peripheral artery disease or previous MI).23 Concomitant medication included angiotensin II receptor blocker, angiotensin-converting enzyme inhibitor, beta-blocker, calcium channel blocker, and statin. Concomitant medication use was defined as when a patient was prescribed medication within 90 days prior to the index date.
Assigned groups and follow-up
We emulated a pragmatic sequence of trials or pseudo-trials by aligning the eligibility window, treatment assignment, and start of follow-up between the study arms.24 To emulate a trial of monotherapy vs. combination therapy, we exploited the experiences of patients after their first year after revascularization. Specifically, we identified all prescriptions of NOAC in patients who met eligibility criteria at least 1 year after revascularization (baseline) and followed the patients until MACCE identification or December 31, 2020, whichever occurred first. Next, using an approach previously described,25 we emulated a second trial using the day after the first trial as a baseline, and so on for every day. Patients who had MACCE or major bleeding or were assigned to the monotherapy group in the previous trial were excluded, and all others were reclassified into the combination therapy group or the monotherapy group depending on whether they received antiplatelet agents or not. Each patient contributed to as many trials as possible if eligible. We repeated the entire process resulting in a total of 2,192 emulated trials. Because discontinuation was defined if the patient did not receive antiplatelet agents for the next 90 days, 90-day landmark analyses were performed for each trial. Thus, patients with efficacy or safety end points within 90 days of each trial were censored (n = 50,948 nonunique individuals). Emulation of sequential trials is a valid and efficient procedure if patients meet eligibility criteria at several time points.26
Statistical analysis
Propensity score matching was performed to minimize the potential impact of confounders on outcomes. In the analysis, covariates were updated at the start of each trial. Multivariable logistic regression estimated the propensity score for the monotherapy group using the following variables at each trial entry date: age, sex, comorbidities, CHA2DS2-VASc score, medications, days from revascularization, and year-month at entry of trial. Matching was performed using a greedy algorithm with a caliper of 0.1. The combination therapy group was matched 1:1 with the monotherapy group within each trial. A standardized mean difference between the monotherapy and the combination group was estimated to compare the distribution of variables used for matching. Covariates with standardized mean difference more than 0.1 that could provide evidence of imbalance between matched groups were included in survival analyses.
The primary analysis was intention-to-treat analysis. Cumulative incidence of each outcome was estimated by the Kaplan-Meier method and log rank tests were applied to evaluate differences between groups. We calculated hazard ratios (HRs) with 95% confidence intervals (CIs) for incidence of clinical outcomes using the Cox regression model. We examined the proportional hazards assumption using plots of the log-log survival function and Schoenfeld residuals.
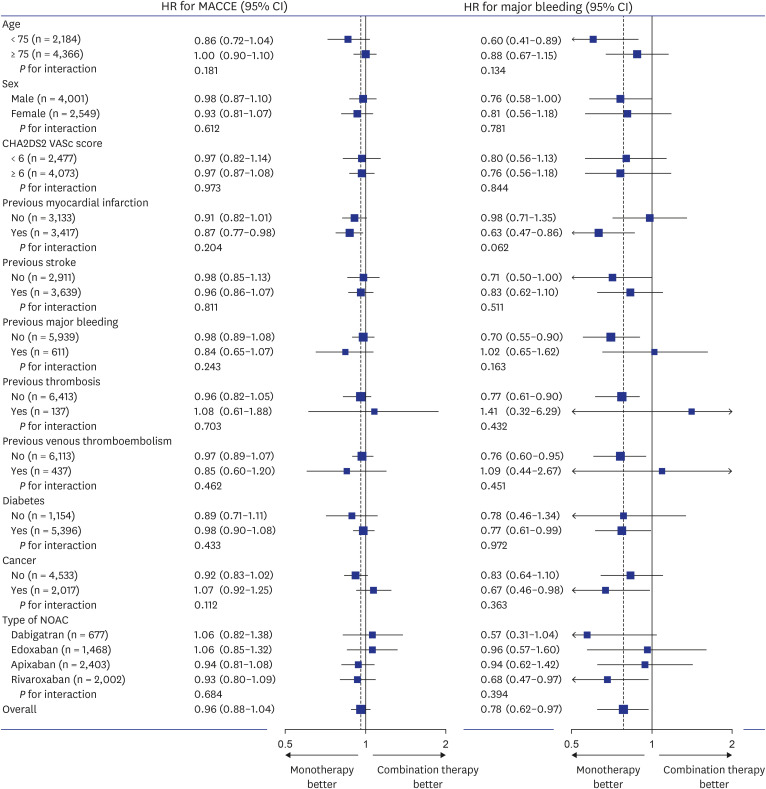
Furthermore, we conducted subgroup analyses by age (age < 75 vs. ≥ 75), sex, CHA2DS2-VAS score (< 6 vs. ≥ 6), previous MI, previous stroke, previous major bleeding, previous thrombosis, previous venous thromboembolism, diabetes, cancer, or type of NOACs.
All P values were 2-sided, and P values less than 0.05 were considered significant. Analyses were performed with the use of SAS® Visual Analytics (SAS Institute Inc., Cary, NC, USA) and R 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
Use of the K-NHIS database is permitted if the study protocols are reviewed and approved by both the government’s official review committee (protocol number: NHIS-2019-1-088) and the local Institutional Review Board. Informed consent was waived as we used de-identified administrative data.
RESULTS
Patients
Of 257,355 potential person-trials (5,647 individuals), 50,948 person-trials (1,182 individuals) which had MACCE or major bleeding events within 3 months were excluded from analysis. Finally, 206,407 person-trials (4,465 individuals) met the eligibility criteria. Of them, there were 3,275 pairs of the monotherapy group and the matched combination therapy group (Fig. 1). The mean age was 77.3 years and 61% were men. Standardized mean differences of all variables were less than 0.1 (Table 1, Supplementary Fig. 1).
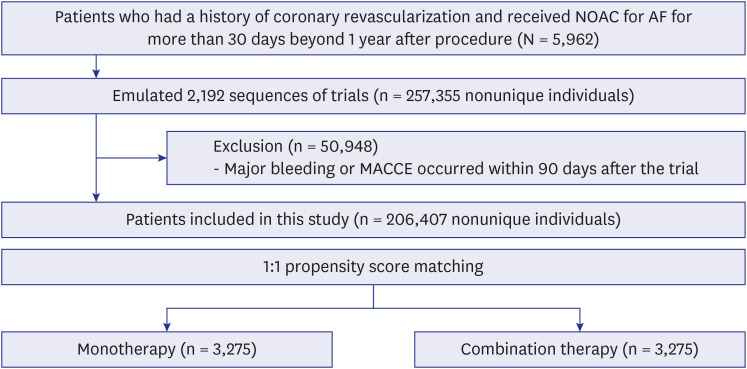
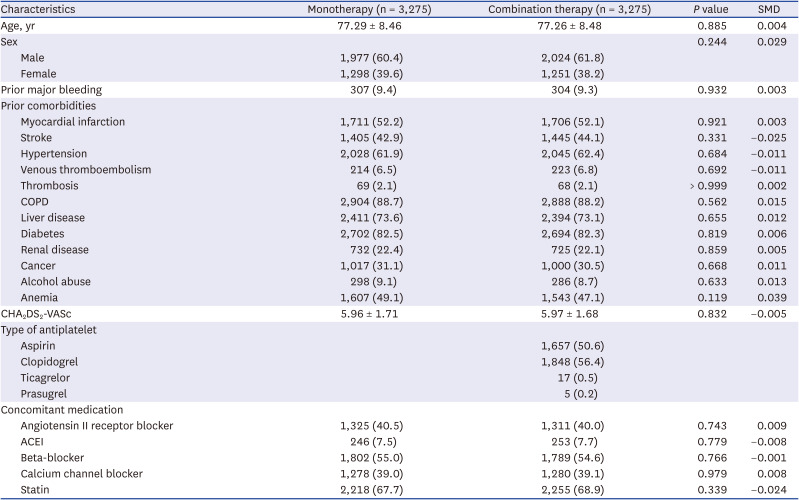
Fig. 1
Study flow.
NOAC = non-vitamin K-antagonist oral anticoagulant, AF = atrial fibrillation, MACCE = major adverse cardiac and cerebrovascular event.
![]()
Table 1
Baseline characteristics
Values are frequency (percentage) or mean ± standard deviation.
SMD = standardized mean difference, COPD = chronic obstructive pulmonary disease, ACEI = angiotensin-converting enzyme inhibitor.
![]()
Efficacy end points
During a median follow-up of 1.24 years (maximum 5.65 years), a total of 1,962 events of MACCE were observed. MACCE occurred in 963 patients in the monotherapy group and in 999 patients in the combination therapy group with corresponding incidence rates of 19.4% and 20.0% per patient-year, respectively (HR, 0.96; 95% CI, 0.88–1.05; P = 0.422) (Table 2, Fig. 2A).
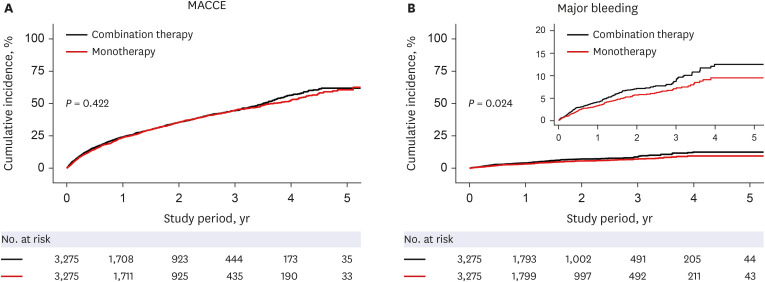
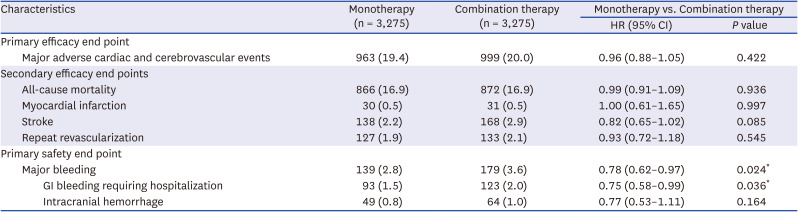
Fig. 2
Clinical outcomes between NOAC monotherapy and NOAC plus antiplatelet combination therapy. (A) MACCE, a composite of all-cause death, myocardial infarction, and stroke; (B) Major bleeding.
NOAC = non-vitamin K-antagonist oral anticoagulant, MACCE = major adverse cardiac and cerebrovascular event.
![]()
Table 2
Clinical outcomes according to antithrombotic therapy
Values are presented as number of event (% per patient-year). Major adverse cardiac and cerebrovascular events were composite of all-cause death, myocardial infarction, and stroke.
HR = hazard ratio, CI = confidence interval, GI = gastrointestinal.
*P < 0.05.
![]()
There were no significant differences in the incidence rates of all-cause death (16.9% vs. 16.9% per patient-year; HR, 0.99; 95% CI, 0.91–1.09; P = 0.936), MI (0.5% vs. 0.5% per patient-year; HR, 1.00; 95% CI, 0.61–1.65; P = 0.997), or stroke (2.2% vs. 2.9% per patient-year; HR, 0.82; 95% CI, 0.65–1.02; P = 0.085) between the monotherapy group and the combination therapy group. Additionally, the incidence rate of repeat revascularization was not significantly different between the two groups (1.9% vs. 2.1%; HR, 0.93; 95% CI, 0.72–1.18; P = 0.545).
Subgroup analyses
Fig. 3 presents subgroup analyses. The efficacy of monotherapy for MACCE was consistent across various subgroups. There was also consistent safety of monotherapy for major bleeding across subgroups.
DISCUSSION
This nationwide cohort study compared the efficacy and safety of NOAC alone versus NOAC plus antiplatelet agent beyond 1 year after coronary revascularization in patients with AF. Compared with combination therapy, NOAC monotherapy was associated with a similar risk of MACCE and a lower risk of major bleeding.
In general, ischemic risk is highest within 1 month after PCI, and the risk is reduced thereafter.27 In the presence of AF, the risk of thromboembolism remains high without anticoagulation therapy, but anticoagulation therapy markedly increases the risk of bleeding when combined with antiplatelet agent. Therefore, finding optimal antithrombotic strategies without increase in bleeding is the cornerstone in management for patients with AF requiring anticoagulation therapy and undergoing PCI. However, there are limited data on the optimal antithrombotic therapy beyond 1 year after coronary revascularization in patients with AF.
In a multicenter registry that enrolled 4,149 outpatients with stable coronary artery disease,12 warfarin plus antiplatelet therapy was associated with an increased bleeding risk but did not decrease the risk of cardiovascular death, MI, or stroke compared with warfarin alone. However, only 11.1% of all patients enrolled in the study received anticoagulants eligible for analysis, and only 7.2% had AF. In addition, more than half of the patients received bare metal stents, which were rarely used in the contemporary drug-eluting stent era. In a Danish registry including 950 patients with stable coronary artery disease and taking warfarin for AF, adding antiplatelet agents to warfarin was not associated with a reduction in the ischemic risk, whereas it increased the bleeding risk. Although the above 2 observational studies reported favorable outcomes with OAC alone over OAC plus antiplatelet agents, not all patients had a history of coronary revascularization, and only warfarin was included as an OAC. Patients who had not undergone coronary revascularization are less likely to benefit from anticoagulation therapy with antiplatelet therapy. In addition, NOACs are currently preferred anticoagulants over warfarin because of their lower risk of bleeding.2829
Our findings are in line with the Atrial Fibrillation and Ischemic Events with Rivaroxaban in Patients with Stable Coronary Artery Disease (AFIRE) study. AFIRE, a multicenter, open-label trial that enrolled 2,215 patients with AF and stable coronary artery disease found that rivaroxaban monotherapy was noninferior for the risk of death or ischemic events to combination therapy and superior for the risk of major bleeding.14 However, there are substantial differences between the AFIRE study and our study. In the AFIRE study, the rates of mortality and cardiovascular events with the combination therapy were 3.4% and 5.8%, respectively, which were much lower than those with the combination therapy in our study (16.9% and 20.0%, respectively). Our study included an unselected cohort from real-world patients resulting in older age (77 vs. 74 years) and a higher thromboembolic risk (CHA2DS2-VASc score, 6 vs. 4) compared with AFIRE study. Moreover, approximately 20% of patients in the AFIRE study did not have a history of coronary revascularization. The results of our study are expected to strengthen the real-world evidence for NOAC monotherapy beyond 1 year after coronary revascularization in patients with AF.
The Optimizing Antithrombotic Care in Patients With Atrial Fibrillation and Coronary Stent (OAC-ALONE) study was another open-label trial comparing OAC alone vs. combined OAC and antiplatelet agent in 696 patients with AF and stable coronary artery disease beyond 1 year after coronary stenting.15 Although the OAC-ALONE study did not establish the noninferiority of OAC alone to combined OAC and antiplatelet agents for the risk of mortality and ischemic events, it was prematurely terminated before enrollment of designed 2,000 patients and 75.2% of the study patients received warfarin.
In recent clinical trials,1415 observational study,13 and our study, the rates of bleeding events appeared to warrant attention during OAC-based antithrombotic therapy in patients with AF and stable coronary artery disease. In the Danish registry,30 rates of major bleeding in patients with AF increased with the number of concomitantly used anticoagulants or antiplatelet agents, and fewer bleeding events occurred in NOAC users than in warfarin users. Therefore, NOAC monotherapy may be a reasonable antithrombotic regimen beyond 1 year after PCI in patients with AF.
Our study has limitations. First, we could not identify reasons for using monotherapy or combination therapy in this study. Although we performed propensity score matching and variables were balanced between the groups, there might be a selection bias induced by unrecorded confounders. Information on angiographic severity, anthropometric or behavioral factors were lacking. Coronary lesion complexity can influence the clinical decision regarding the antithrombotic strategy. Nevertheless, recent randomized studies have suggested that intensified antiplatelet therapy does not significantly reduce ischemic events.531 Furthermore, considering the elevated bleeding risk in our study population due to additional anticoagulation therapy for AF, patients may derive limited benefits from intensified antiplatelet therapy.32 Second, we focused only on intracranial bleeding and gastrointestinal bleeding requiring hospitalization as safety end point. But the definition and incidence rates of major bleeding in our study were similar with those of previous study.30 Although there may have been unrecorded cases of non-major bleeding events in this nationwide registry, the risk of life-threatening bleedings rather than minor bleedings is a reasonable factor for determining the antithrombotic regimen in patients at high ischemic risk, such as concomitant AF and a history of coronary revascularization. Third, the follow-up duration was relatively short because the use of NOACs increased significantly since 2015, following the extension of national health insurance coverage for NOACs, irrespective of warfarin use, in South Korea. A further study with extended follow-up may be warranted to confirm our findings.
In this nationwide registry, there was no significant difference in MACCE between NOAC monotherapy and NOAC plus antiplatelet combination therapy beyond 1 year after coronary revascularization in patients with AF. Compared with combination therapy, NOAC monotherapy was associated with a lower risk of major bleeding.
 XML Download
XML Download