

 PDF
PDF Citation
Citation Print
Print


Introduction
With the exception of malaria, most parasitic infections are neglected tropical diseases (NTDs) that affect more than one billion individuals globally, predominantly in impoverished communities situated in tropical or subtropical regions [1]. The list of NTDs was recently expanded by the World Health Organization (WHO) to include 21 infectious diseases caused by viruses, bacteria, parasites, fungi and toxins, including 12 parasitic diseases [1]. Various stakeholders, including the WHO, developed countries, non-governmental organizations, and pharmaceutical companies, are working together to control, prevent, eliminate, and eradicate NTDs according to the NTD roadmap for 2021-2030 guided by the WHO [1].
A nationwide survey of intestinal parasitic infections conducted in Korea in 2012 revealed a prevalence of 2.6%, with Clonorchis sinensis having the highest infection rate of 1.9% [2]. Nationwide control measures for parasitic infections, such as mass stool examinations and selective drug treatment, have resulted in the successful control of soil-transmitted helminthiases, including Ascaris lumbricoides, Trichuris trichiura, and hookworms, in Korea [3]. However, parasites that live in tissues or are transmitted through food are still prevalent in Korea because of the cultural habits of eating raw fish or meat, and the diagnosis of these conditions is important. Instead of the invasive approach of obtaining worms or larvae from tissues, serodiagnosis has been developed for tissue helminthiases and is widely used to diagnose infections caused by tissue-invading parasites.
Serological tests are not as definitive as stool tests for the diagnosis of parasitic diseases. Instead, they are used as adjuncts to clinical symptoms, laboratory findings, and radiological imaging for the diagnosis of tissue-invading parasites [4,5]. The enzyme-linked immunosorbent assay (ELISA) is commonly used to detect specific IgGs against parasite antigens in the blood of suspected patients. This review discusses serological tests for the diagnosis of parasitic infections in Korea, with a special emphasis on ELISAs.
Multi-antigen ELISA
Tissue-invading parasites, including Clonorchis sinensis, Paragonimus westermani, the metacestodes of Taenia solium, and the plerocercoid larvae of Spirometra erinacei (sparganum), remain a significant public health issue in Korea. Clonorchiasis can lead to cholangiocarcinoma if left untreated, and the other abovementioned parasites are clinically significant because they can invade the nervous system and cause neurological symptoms, such as headaches, seizures, and paralysis. ELISAs have been developed to diagnose tissue-invasive parasitic infections. However, because cross-reactions between helminthiases are common, a multi-antigen ELISA that simultaneously detects antibody responses to four parasite antigens is recommended [4,5].
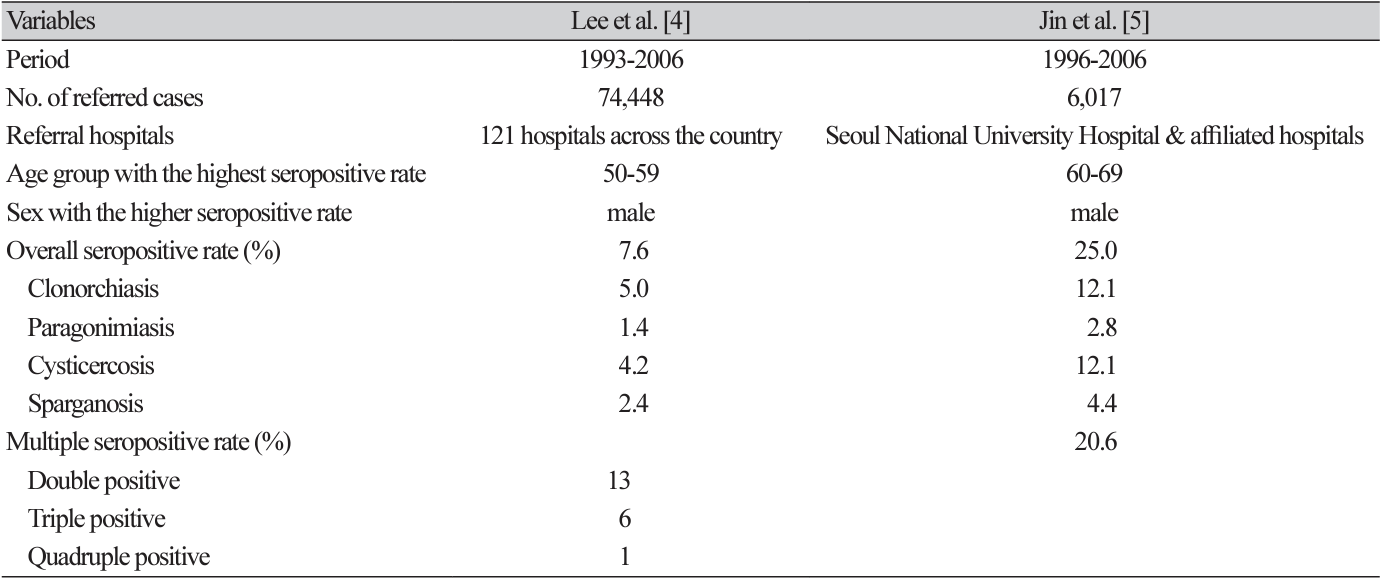
Two research groups in Korea have presented the results of multi-antigen ELISAs performed for over a decade (Table 1). In their analysis of ELISA results from 1993 to 2006, Lee et al. [4] (2010) found that 7.6% of 74,448 specimens were positive for antigens from any of the four tissue parasites. The antibody positivity rate showed a gradual decline from 18.7% in 1993 to 6.6% in 2006, and the positivity rate for individual parasites also gradually decreased. In contrast, Jin et al. [5] (2017) reported that 25% of 6,017 specimens from 1996-2006 were positive for one of the four parasites. The seropositivity rates for each parasite fluctuated, but slowly decreased after 2004, with considerable variation in the annual seropositivity rate, ranging from 12.1% to 35.7%.
The discrepancy in seropositivity rates between the two studies is believed to be attributable to differences in referral sources and the types and numbers of specimens analyzed. Lee et al. [4] (2010) analyzed specimens from 121 hospitals across the country, including serum, cerebrospinal fluid (CSF), or both. Approximately one-sixth of the samples were CSF samples from patients with suspected parasitic infections of the central nervous system, including the brain. In contrast, Jin et al. [5] (2017) analyzed samples from Seoul National University Hospital and its affiliated hospitals that were referred for differential diagnosis of suspected tissue helminthiases, including those affecting the liver, lungs, and central nervous system. Although there was a discrepancy in the seropositivity rates between the two studies, clonorchiasis and cysticercosis exhibited higher positivity rates than the other two helminthiases. The highest antibody positivity rates were observed in men in their 50s and 60s.
The possibility of polyparasitism and cross-reactivity should be considered [5]. If a multi-antigen ELISA yields seropositive results with more than two parasite antigens, the antigen with the strongest reaction is considered the causative infection, whereas a weak positive reaction is regarded as a cross-reaction. It is important to interpret serological test results in conjunction with other clinical symptoms and laboratory data, including radiological imaging and biopsy interpretation, to identify the causative parasitic infection.
Cross-reactions has been observed in approximately 20% of cases, mainly between helminths of the same class, such as between clonorchiasis and paragonimiasis, or between sparganosis and cysticercosis (Table 1) [4,5]. In an analysis of cases with double-positive reactions, clonorchiasis cross-reacted, in the following order, with cysticercosis, paragonimiasis, and sparganosis, while paragonimiasis cross-reacted mainly with clonorchiasis [5]. Cysticercosis cross-reacts with either clonorchiasis or sparganosis, whereas sparganosis cross-reacts with either cysticercosis or clonorchiasis [5].
Another limitation of serological tests, including ELISA, is the difficulty of differentiating between past and present infections [5]. Positive results for clonorchiasis may include both past and present infections, as clonorchiasis is the most common parasitic infection in Korea. Some cases of neurocysticercosis are not newly diagnosed, but have been diagnosed in the past and were found to be seropositive during work-up for other neurologic diseases [6].
Clonorchiasis
Clonorchiasis is prevalent among residents of riverside areas who consume raw freshwater fish, especially in the southern areas of Korea along the Nakdong and Seomjin Rivers [7]. Although stool examination remains the gold standard for diagnosis, ELISA using crude or excretory-secretory antigens is a valuable tool for the diagnosis of clonorchiasis. To improve diagnostic accuracy, it is recommended that both stool examination and ELISAs be performed simultaneously, as most cases of clonorchiasis are more likely to be light-infected and the sensitivity of these tests may decrease [5,8].
To develop a serologic diagnostic test for clonorchiasis, a search was conducted for antigens that are sensitive to and specific for the disease [9-12]. ELISA using excretory-secretory antigens showed superior results, with a sensitivity of 92.5% and specificity of 93.1%, compared to 88.2% and 97.8% for ELISAs using crude antigens [8]. Antigens suitable for serodiagnosis include the 7-kDa protein of the excretorysecretory product as well as the omega-class glutathione transferases and cysteine proteinase of C. sinensis [9-11]. The recombinant 7-kDa protein demonstrated a sensitivity of 81.3% and a specificity of 92.6% using ELISA [11]. The sensitivities of two recombinant forms of C. sinensis omega-class glutathione transferases (rCsGSTo1 and rCsGSTo2) were 92.3% and 93.2%, respectively, with specificities of 89.7% (rCsGSTo1) and 97.6% (rCsGSTo2) [9]. Shen et al. [12] (2009) evaluated the applicability of four recombinant proteins, including a 7-kDa protein, 28-kDa cysteine protease, and 26- and 28-kDa glutathione S-transferases, for serodiagnosis. The crude antigen demonstrated the highest sensitivity (92.7%) and specificity (100%), whereas the sensitivities of the four recombinant proteins were significantly lower, with specificities exceeding 94.5%. These results suggest that a cocktail or chimeric antigen may provide a more effective serodiagnostic approach for clonorchiasis than a single recombinant antigen in ELISAs [12].
Paragonimiasis
Paragonimiais is a disease that occurs when humans consume raw or undercooked freshwater crustaceans, such as crabs and crayfish, containing metacercariae of P. westermani or when they ingest undercooked meat from paratenic hosts, such as wild boars, deer, and rodents [13]. In Korea, cases of paragonimiasis have decreased in recent years because of a decrease in the population of freshwater crustaceans caused by water pollution [4]. It is challenging to differentiate pulmonary paragonimiais from tuberculosis or lung cancer. Additionally, the patient’s symptoms, clinical findings, and laboratory findings are not easily differentiated from other diseases, which often results in the delayed diagnosis of paragonimiasis using ELISA [13]. Paragonimiasis should be included in the differential diagnosis of parasitic diseases in patients with pulmonary lesions associated with eosinophilia and/or elevated IgE levels [4]. It is common for the metacercariae of P. westermani to fail to reach the lungs during migration within the human body [14]. Instead, they become trapped in other organs, such as the brain, liver, and abdominal wall, resulting in the development of ectopic paragonimiasis, which presents diagnostic and therapeutic challenges.
Cho et al. [15] (1981) reported that an ELISA using the crude antigen of P. westermani is a highly sensitive (86%) and specific (100%) method for diagnosing paragonimiasis without cross-reactions with other parasite antigens. ELISA using recombinant P. westermani yolk ferritin demonstrated 100% sensitivity and 97.2% specificity for sera, and 97% sensitivity and 92.5% specificity for CSF [16]. This assay is highly effective for the serodiagnosis of both early and chronic cerebral paragonimiasis.
Jin et al. [5] (2017) analyzed the correlation between seropositivity and clinical diagnoses in 165 patients whose medical records were available. The results indicated that paragonimiasis showed the highest correlation rate (81.8%). Of the 685 cases of pleuropulmonary paragonimiasis analyzed over a 22-year period, Ahn et al. [13] (2021) found that only 20 tested negative by ELISA. These studies indicate that ELISA is a reliable diagnostic method for paragonimiasis.
Cysticercosis
The prevalence of taeniasis and cysticercosis in Korea has declined significantly, with an egg positive rate of 0.04% in 2012 [2]. A prevalence survey of neurocysticercosis conducted on 2,667 randomly selected patients with epilepsy from 1987 to 1990 yielded a positivity rate of 4.0% [17]. The highest prevalence (8.4%) was observed in patients residing in Cheju-do. Statistical analysis of data provided by the Health Insurance Review and Assessment Service in Korea showed a notable decrease in the number of cysticercosis cases from 642 in 2011 to 433 in 2018; however, a significant proportion of these were considered to be previous infections found during follow-up for other neurological conditions [6]. This dramatic change in the prevalence of taeniasis and cysticercosis is thought to be due to changes in pig production, improvements in sanitation and waste disposal systems, the introduction of effective anthelmintics (praziquantel), and improvements in radiological imaging.
Cystic fluid from T. solium metacestodes is the most commonly used antigen for cysticercosis ELISAs, with a sensitivity of 90.1% and a specificity of 88.5% [18]. CSF shows higher sensitivity than serum, indicating the potential benefit of using both serum and CSF in a serological test to differentiate neurocysticercosis from other neurological diseases [18]. Serological follow-up assessments for neurocysticercosis should be performed annually for at least 5 years to differentiate between patients who have been cured and those who still have chronic symptoms and slowly calcifying lesions [19,20].
Cross-reactivity may occur with other larval cestode infections, such as echinococcosis and sparganosis. These reactions are induced by several proteins that are usually high-molecular-weight proteins of T. solium metacestodes. In contrast, low-molecular-weight proteins (7-24 kDa) in cystic fluid have been shown to elicit specific antibody responses [20]. Proteomic analyses have shown that the majority of the low-molecularweight proteins may originate from two macromolecules of 120 kDa (consisting of 14-38 kDa subunits) and 150 kDa (7-15 kDa subunits) present in the cyst fluid of T. solium metacestodes [20,21]. These two glycoproteins elicit strong antibody responses against sera from patients with neurocysticercosis [20,21]. Bae et al. [21] (2008) constructed a recombinant chimeric antigen from four representative proteins (one from the 120 kDa protein and three from the 150 kDa protein) with different epitope specificities. The recombinant chimeric protein ELISA showed sensitivity comparable to that of the cystic fluid ELISA in the diagnosis of neurocysticercosis, but a markedly different specificity, with a significant reduction in cross-reactivity between neurocysticercosis and echinococcosis. Their study clearly demonstrated that recombinant chimeric antigen could replace native cystic fluid as a reliable antigen source for neurocysticercosis diagnostic platforms [21].
Sparganosis
At least 438 cases of sparganosis were documented in Korea between 1924 and 2015 [22]. The ingestion of raw or undercooked frogs, snake flesh, or other paratenic hosts, and drinking water containing cyclops infected with the procercoid larvae of S. erinacei are two common modes of human infection in Korea [22]. Sparganosis is most common in men aged > 50 years, and most cases involve subcutaneous tissue, followed by the central nervous system [22]. Since the 1980s, the number of cases diagnosed prior to surgical intervention has increased significantly because of the availability of serological and imaging diagnostics, such as ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) [22]. A crude saline extract of sparganum has been used as an antigen for ELISA. Seroepidemiological studies conducted on healthy individuals in Korea indicated that the seropositivity rates for sparganosis range from 1.7% to 4.2% [23-25]. Cross-reactions have been observed in more than 50% of serum samples that are positive for sparganosis, with cysticercosis and clonorchiasis being the most common [5].
Other tissue parasitic infections
Toxocariasis
The epidemiological features of toxocariasis differ between Western and Eastern countries. In Western countries, children are more likely than adults to contract Toxocara canis infections because of their greater level of exposure to soil contaminated with T. canis eggs, which may result from geophagy, poor hygiene, or contact with dogs [26]. Conversely, adults have a higher incidence of toxocariasis than children in Eastern countries such as Korea and Japan. Adults contract toxocariasis as a food-borne infection through the consumption of raw meat or liver from animals infected with T. canis larvae [27,28].
Toxocariasis can be diagnosed based on a patient’s medical history, clinical and laboratory findings, and serological tests [27]. A commercial ELISA kit is widely used for the serodiagnosis of toxocariasis. It uses the excretory-secretory antigen derived from second-stage larvae of T. canis to detect T. canis-specific IgG with 91% sensitivity and 86% specificity [29]. Jin et al. [30] (2013) developed an ELISA using the crude antigen of T. canis larvae and showed that it has a sensitivity of 92.2% and specificity of 86.6%, which is comparable to that of a commercial ELISA kit.
The relationship between toxocariasis and patients’ place of residence, whether urban or rural, is a topic of debate in Korea. Previous studies have reported a higher prevalence of toxocariasis in rural areas than in urban areas [31,32]. In contrast, other studies have found that the seropositivity rate was approximately 5% among adults in rural areas [33], and 65.0% among healthy people with eosinophilia living in Seoul [34]. The observed discrepancies in the seroprevalence of toxocariasis with respect to residential areas are likely attributable to cultural preferences for consuming raw animal liver in Korea, rather than to the risk of exposure to T. canis eggs in the environment.
In Korea, toxocariasis is the most prevalent causative parasite in patients with suspected parasitic infections and eosinophilia, particularly in those with a history of consuming raw meat or livers of animals [27,35,36]. The seroprevalence of toxocariasis exhibits considerable variability among subjects with eosinophilia [27,28,31,34-38]. The rates have ranged from 8.7% to 86.7%, with most participants exhibiting seroprevalence rates exceeding 45%. Despite considering cross-reactions and past infections, the high prevalence of antibody positivity for toxocariasis indicates that toxocariasis should be differentiated in patients presenting with eosinophilia. Regardless of the treatment, most cases of eosinophilia associated with toxocariasis have a self-limiting course with a median duration of 3 months, suggesting a 3- or 4-month follow-up interval for patients with eosinophilia [27,36].
Trichinellosis
Since the first reported case of human infection with Trichinella spiralis in 1997 [39], there have been eight documented outbreaks of human trichinellosis in Korea [40-44]. These infections are transmitted through the ingestion of raw meat from wild boars or soft-shelled turtles. The diagnosis in these cases was based on the identification of T. spiralis larvae in the muscle and/or the use of ELISA with crude T. spiralis larval antigen [39-44].
Fascioliasis
Humans can become infected with Fasciola hepatica, a trematode of cattle and sheep, by ingesting water or raw water vegetables contaminated with metacercariae [45]. Since the first human case reported in Korea in 1976 [46], cases have been sporadically documented [47-53]. Ectopic fascioliasis is common and has been found in various organs, including the cecum [47], abdominal muscles [52], pancreas [50], and eyes [48]. Fascioliasis can be diagnosed by direct identification of worms or eggs from surgical specimens, serological tests, imaging findings, and histopathological observation [47-53]. Currently, fascioliasis is mainly diagnosed by ELISA using crude antigens, excretory-secretory antigens, or recombinant antigens [53-55], and less than half of the reported cases have been diagnosed by ELISA [47-53].
Echinococcosis
The diagnosis of echinococcosis caused by either Echinococcus granulosus or E. multilocularis may be based on clinical findings, serological analysis, and radiological imaging techniques such as ultrasonography, CT, and MRI [56]. Most cases in Korea have been imported, with the exception of two cases in which the origin of infection was not clearly identified [57]. Consequently, a history of travel or residence in areas where echinococcosis is endemic should be investigated for diagnosis. Serological testing is useful as an adjunct to the diagnosis of echinococcosis and as a monitoring method to observe the progress of surgery or drug treatment for cystic echinococcosis [56]. The sensitivity and specificity of ELISA using the hydatid cyst fluid of E. granulosus are 91.5% and 96%, respectively, and cross-reactivity with cysticercosis or clonorchiasis has been observed [57]. The ELISA absorbance of cystic echinococcosis patients was found to be the highest with antigen B purified from sheep E. granulosus cystic fluid antigen, followed by cystic fluid antigens from humans, sheep, mice, and cows, in descending order [57]. These findings suggest that ELISA using antigen B from sheep E. granulosus cystic fluid antigen may offer an improved serodiagnostic approach.
Conclusion
ELISA is the recommended diagnostic method when a tissue-invading parasite infection is suspected. It is advisable to perform an ELISA for suspected parasitic infections in conjunction with a multi-antigen ELISA, rather than as a standalone test, to eliminate the possibility of cross-reactions. Furthermore, obtaining a comprehensive history of the transmission mode of the suspected parasites and the patient’s residence or travel to an endemic region may assist in reaching a definitive diagnosis. In Korea, in cases where eosinophilia is present in patients with suspected parasitic infections, it is crucial to perform ELISA for the differential diagnosis of toxocariasis. The results of serological tests are not necessarily conclusive and should be interpreted in the context of other symptoms, as well as clinical and imaging findings.
 XML Download
XML Download