

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of patients with chronic kidney disease (CKD) has increased in recent years, which has led to a rise in the number of patients on maintenance hemodialysis [1]. Adequate functional vascular access is vital for patients who have undergone maintenance hemodialysis. Vascular access dysfunction is associated with higher risks of both morbidity and mortality [23]. The overall patency rates for arteriovenous fistulas (AVFs) and arteriovenous grafts (AVGs) have been reported to be 55% and 40%, respectively at 2 years [4].
AVF using an autogenous vein is the preferred vascular access for hemodialysis owing to its higher patency and lower infection rates; however, it does carry a risk of maturation failure [5]. According to previous studies, only 60%–70% of AVFs mature to function [67]. Older age, female sex, diabetes mellitus, cardiovascular disease, and high body mass index have been reported to be predictive factors for AVF maturation failure; however, the results have not been consistent [178910]. Studies on the predictive factors regarding AVG patency were limited [11].
A meta-analysis showed that preoperative routine duplex ultrasound mapping prior to AVF creation substantially reduced its immediate failure rate [12]. A number of previous studies have shown that vein diameter is an independent predictor of functional AVF [131415]. Arterial diameter, AVF blood flow, and depth have also been reported as factors associated with AVF function [91516]. Although there is some controversy regarding the importance of each hemodynamic factor on AVF outcomes, duplex ultrasound study is widely performed before AVF or AVG creation in most centers.
The suitability of AVF for cannulation can be determined clinically and based on duplex ultrasound. The “Rule of 6s” has been widely accepted, that is 600-mL/min blood flow, 0.6-cm diameter, and 0.6-cm depth from the skin [1517]. Several studies have demonstrated that a minimum venous diameter of ≥0.4 cm and a flow volume of ≥500 mL/min, which have become known as the University of Alabama at Birmingham (UAB) criteria, would predict AVF maturation [18]. For AVG, a minimum access blood flow of 600 mL/min was suggested as a criterion for maturation; however, there are very limited studies on AVG maturation [19]. Once AVFs or AVGs are used for cannulation, surveillance can be based on clinical monitoring, blood flow measurement, and duplex ultrasound findings. Regular duplex ultrasounds and preemptive correction of stenosis do not improve vascular access outcomes, and thus are not recommended in a current guideline [172021].
Timely referral is important for functional vascular access at the initiation of hemodialysis. However, maturation failure or early occlusion of vascular access can negate the positive effects of timely referral and advanced placement of vascular access. Thus, predicting the early failure of AVFs and AVGs, as well as appropriate surveillance based on individual risks, are warranted. This study aimed to investigate the incidence of early failure of vascular access for hemodialysis and the associated factors. We also determined whether the hemodynamic factors measured in pre- and postoperative duplex ultrasounds could be used to predict the early failures of AVFs and AVGs.
Go to : 
METHODS
Ethics statement
The Institutional Review Board of Chung-Ang University Hospital approved the protocol of the present study (No. 2304-025-19469) and waived the requirement for informed patient consent due to its retrospective nature.
Study population
Patients who underwent AVF or AVG for hemodialysis at Chung-Ang University Hospital, a tertiary referral hospital in South Korea, were included in this study. Between September 2019 and January 2023, a total of 239 AVF or AVG had been created by a vascular surgeon. We performed a retrospective review of the patient’s medical records. Data were collected regarding baseline demographics, type of vascular access, prior history of vascular access, cause of CKD, and medical characteristics.
Preoperative assessment
Physical examination included palpation of brachial, radial, and ulnar artery pulses, as well as the Allen test. The cephalic and basilic veins were palpated to assess their continuities. Inspection of the chest walls and arm for signs of central venous stenosis was included. All patients underwent preoperative duplex ultrasounds. Duplex ultrasound was performed in the supine position with an elastic tourniquet. The diameters of the inflow artery and outflow vein were measured. The inner wall artery diameters for the radial artery at the wrist and the brachial artery at the antecubital fossa were measured. The inner wall diameter of the cephalic vein was measured from the wrist to the shoulder and recorded every 5 cm. The minimal diameter of the vein was defined as the preoperative venous diameter. When the minimal cephalic vein diameter was <2.0 mm, the diameters of the basilic and axillary veins were measured to select the vein for AVG. For those patients underwent who AVG, the diameter of the vein at anastomosis with a prosthetic graft was defined as the preoperative venous diameter.
Operation
The type of vascular access was determined by physical exam and duplex ultrasound findings. When the minimal cephalic vein diameter was ≥2.0 mm, AVF was planned; otherwise, AVG was selected. In general, an inflow artery diameter of ≥2.0 mm for the radial artery or ≥3.0 mm for the brachial artery was chosen. All AVFs and AVGs were created in the operating room under local anesthesia by a vascular surgeon with more than 10 years of experience. End-to-side anastomosis was done using running sutures. The patients’ veins were flushed with heparinized saline and systemic heparin was not used.
Postoperative duplex study and follow-up
Postoperative duplex ultrasound was performed at 6 and 3 weeks following AVF and AVG creation, respectively. The diameter and flow volume of each inflow artery were measured 5 cm proximal to the anastomosis site. The diameter and flow volume of the cephalic vein were measured at the anastomosis site and at every 5-cm segment, then averaged [16]. In AVG, the flow volume of the middle prosthetic graft was measured 3–5 times and averaged.
Early failure
Early failure was defined as any event that necessitated surgical or endovascular intervention within 6 months following AVF or AVG creation. It included maturation failure, failure of successful cannulation due to thrombosis or stenosis, and initial successful cannulations, that later required surgical or endovascular interventions to maintain patency. Maturation failure was defined as inability of the access to be used for hemodialysis with 2 needles for 75% of dialysis sessions over a continuous 4-week period [19]. Treatment indications for vascular access stenosis were inadequate flow volume to support dialysis, elevation of venous pressure, and delayed puncture site hemostasis [22]. Endovascular therapy was first attempted for AVF or AVG thrombosis or stenosis. Cases of superficialization for deep-seated veins and AVF ligation due to hand ischemia were included in the early failure group.
Statistical analysis
Continuous variables are presented as means and standard deviations and were compared using the 2-sampled Student t-tests. Categorical variables are presented as frequencies and percentages and were analyzed using the Pearson chi-square or Fisher exact tests. All analyses were performed with a statistical significance level of 0.05 and using 2-tailed tests. A logistic regression analysis was performed to investigate the independent contributions of variables to the likelihood of early failure. Variables from our univariable analyses with P-values of <0.10 were considered for inclusion in the final multivariable model. Receiver operating characteristic (ROC) curves analysis was performed to determine an appropriate cutoff value for further dichotomized analysis, as well as to analyze the associations of the parameters measured in the duplex ultrasounds with early failure. The Kaplan-Meier method was used to estimate primary, primary-assisted, and secondary patency. A P-value of <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics ver. 26.0 (IBM Corp.).
Go to :
RESULTS
Baseline characteristics
Among 239 patients who underwent AVF or AVG creation during the study period, 14 were lost to follow-up, 10 did not undergo postoperative duplex ultrasounds, and 1 died within 6 months. Twenty-five patients did not start hemodialysis within 6 months following vascular access creation. Excluding them, 189 patients were included in our final analysis. The mean age of the patients was 67.9 years and 59.3% were male.
Early failure
Early failure occurred in 36 patients (19.0%), which included 22 AVFs and 14 AVGs. Of the 22 AVFs with early failure, 4 were abandoned. Seven AVFs with delayed maturation could be cannulated after the intervention. Ten AVFs were successfully used for cannulation, however required balloon angioplasty or thrombectomy within 6 months to maintain patency. One patient underwent hematoma evacuation 3 weeks after AVF creation. Of the 14 AVGs, 5 underwent balloon angioplasty for venous anastomosis causing inadequate flow volumes for hemodialysis. Five patients had acute thrombosis and required thrombectomies to maintain patency. Four patients underwent AVG ligation due to hand ischemia, recurrent bleeding, or severe recalcitrant arm edema.
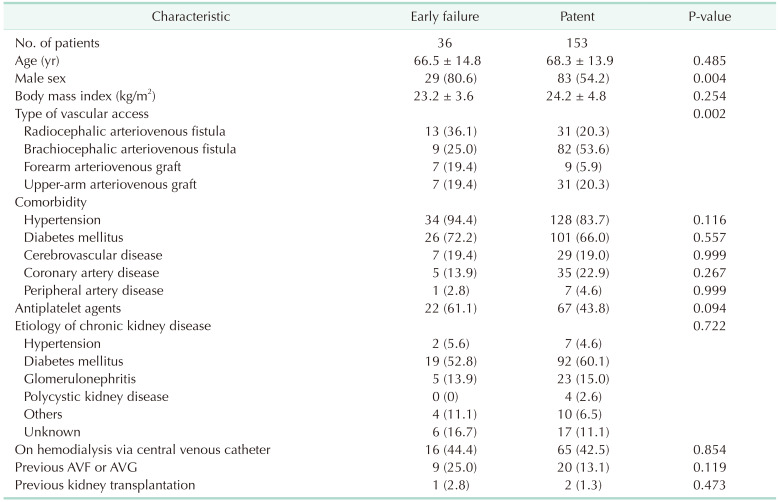
The rates of early failure tended to be higher in AVG compared to AVF (25.9% vs. 16.3%, P = 0.152). In AVF, early failure was significantly higher in radiocephalic AVF compared to brachiocephalic (29.5% vs. 9.9%, P = 0.006). The proportion of male patients was significantly higher in the early failure group compared to the patent group. No other significant differences were observed in terms of the baseline characteristics between the groups (Table 1).
Duplex study findings
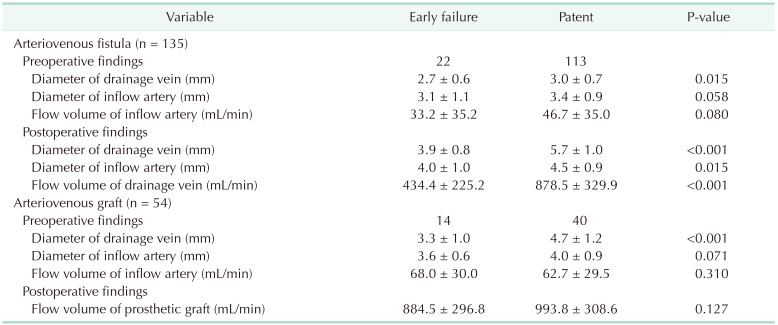
In the patients who underwent AVF, the mean preoperative venous diameter was significantly smaller in the early failure group compared to the patent group (2.7 ± 0.6 mm vs. 3.0 ± 0.7 mm, P = 0.015). The preoperative diameter and flow volume of the inflow artery tended to be smaller in the early failure group; however, these differences did not reach statistical significance. For the duplex studies performed 6 weeks following AVF creation, the diameters of the drainage vein and inflow artery, as well as the flow volume of the AVF, were all significantly lower in the patients with early failure compared to those without early failure. In the AVG group, the preoperative venous diameter was the factor that was found to show a significant difference between the 2 groups (3.3 ± 1.0 mm vs. 4.7 ± 1.2 mm, P < 0.001) (Table 2).
Sonographic score
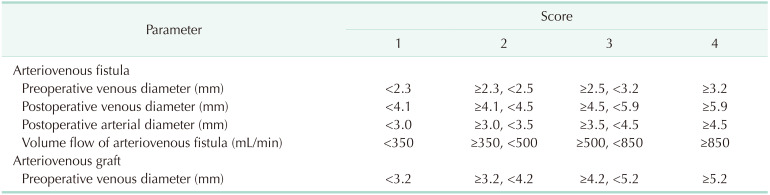
A sonographic score was defined based on the parameters in the pre- and postoperative duplex ultrasounds. For AVF, the preoperative venous diameter, postoperative venous and arterial diameter, and volume flow were included in the scoring system. Cutoff values in each parameter for early failure were determined using ROC analysis. Each parameter was classified into 2 groups according to the cutoff value, and then divided into 4 groups by the median value. For AVG, the sonographic score was defined based on preoperative venous diameter, which was the only parameter that was found to be associated with early failure. The cutoff values for preoperative venous diameter, postoperative venous and arterial diameter, and volume flow that were found to be associated with early failure of AVF were 2.5 mm, 4.5 mm, 3.5 mm, and 500 mL/min, respectively. The cutoff value for preoperative venous diameter was 4.2 mm in AVG. A detailed sonographic score definition is described in Table 3.
For AVF, the postoperative venous diameter was highly predictive of early failure among the parameters measured in duplex ultrasounds (area under the curve [AUC], 0.92). The sonographic score which was the combination of preoperative venous diameter, postoperative venous and arterial diameter, and volume flow was found to be predictive of early failure (AUC, 0.82). For AVG, the preoperative venous diameter was fairly predictive of early failure (AUC, 0.82) (Fig. 1).
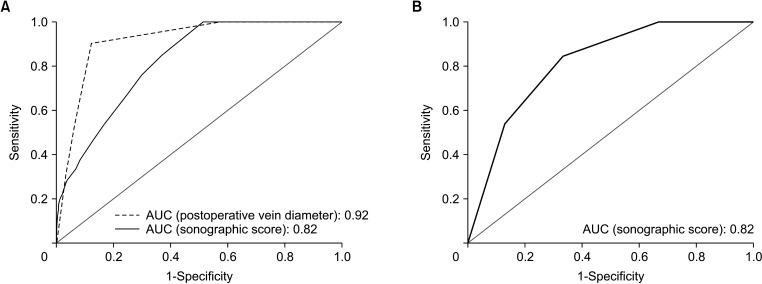 | Fig. 1Receiver operating characteristic (ROC) analysis and definition of an appropriate cutoff value for the sonographic score with regard to predicting the early failure of (A) arteriovenous fistula (AVF) and (B) arteriovenous graft (AVG) for hemodialysis. The sonographic score consists of the preoperative venous diameter, postoperative venous and arterial diameter, and volume flow for AVF and preoperative venous diameter for AVG. AUC, area under the curve.
|
Factors associated with early failure
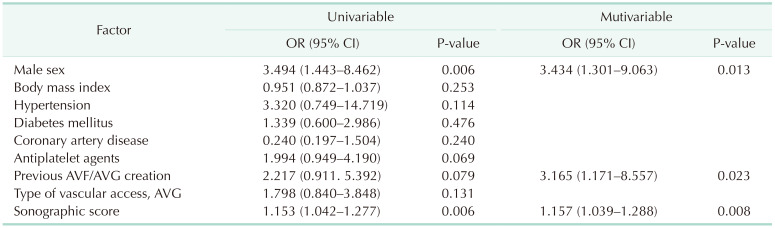
A logistic regression analysis was performed. Male, the use of antiplatelet agents, a previous history of vascular access creation, and the sonographic score from our univariable analysis were included in the multivariable model. In our multivariable analysis, 3 factors were associated with early failure. The sonographic score defined above was found to be a significant predictor of early failure (odds ratio, 1.157; 95% confidence interval, 1.039–1.288; P = 0.088). A previous history of AVF or AVG creation and male sex were associated with early failure (Table 4).
Go to :
DISCUSSION
Functional vascular access is crucial for patients undergoing hemodialysis. However, maturation failure and recurrent stenosis reduce the patency of permanent vascular access. This study demonstrated that approximately 20% of newly created vascular accesses required surgical or endovascular interventions within 6 months to maintain patency. Radiocephalic AVFs had the highest risk of early failure among the different types of vascular accesses. The most noteworthy finding of this study was that the postoperative venous diameter in AVF and the preoperative venous diameter in AVG were highly predictive of early failure. In addition, male sex and a previous history of vascular access creation were also associated with early failure.
Radiocephalic AVF had a higher risk of early failure than brachiocephalic AVF in this study. Previous studies have also reported worse outcomes for forearm AVFs than those in the upper arm [2324]. A distal-to-proximal approach to AVF creation provides the best opportunity to preserve vessels for future vascular access sites. However, it should not be insisted upon in all cases, and the selection of an optimal AVF site should be individualized. If distal forearm AVFs were attempted in all patients, this could lead to longer times to successful cannulation and higher rates of maturation failure. The kidney disease outcomes quality initiative clinical practice guidelines mention that it is reasonable not to create forearm AVFs in patients who are expected to be on hemodialysis for only a short duration [17]. Upper-arm AVF may therefore represent the first choice in patients with higher risks of early failure as well as older patients [25].
Female sex was found to be a poor prognostic factor for vascular access patency in previous studies [926]. In contrast to these findings, our results showed that men were more likely to have early failure than women. In this study, only 10% of the female patients underwent radiocephalic AVF, compared to 32% of the male ones. We assumed that the lower proportion of radiocephalic AVFs in the women of our study contributed to the contrary results we observed. One commonly suggested reason for poor vascular access outcomes in females is smaller vessel diameters; thus, brachiocephalic AVFs are often preferred to radiocephalic ones in women [27]. In this study, all of the patients underwent preoperative duplex ultrasound assessment, which was then used to determine the type and location of vascular access. Female patients with very small-diameter vessels were not chosen for radiocephalic AVFs after being evaluated via duplex ultrasound study, which may also have reduced the incidence of early failure, including maturation failure.
A prior history of vascular access placement was another factor that was associated with early failure. Decreased suitable candidate veins and suboptimal location of vascular access can cause poor outcomes in patients who have undergone AVF or AVG creation. In addition, the presence of an ipsilateral central venous catheter was associated with poor patency of AVFs [2829]. Endothelial damage and venous stenosis caused by an indwelling catheter increase the risk of AVF thrombosis [30].
This study revealed that postoperative venous diameter was highly predictive of the early failure of AVF. In fact, the predictive value of postoperative venous diameter was greater than that of combining preoperative venous diameter, postoperative arterial diameter, and volume flow. Postoperative duplex study findings are used for determining the suitability of cannulation and can also provide valuable predictors of early failure. Even newly created AVFs that mature and are successfully cannulated for hemodialysis experience early failure in a certain proportion. In our study, no patients with postoperative venous diameters of >5.9 mm, experienced early failure, thus short-term surveillance was not necessarily required in this group. In contrast, in patients with postoperative venous diameters of ≤4.5 mm, over 50% experienced early failure. Even if AVFs are cannulated successfully, this patient group should remain under intensive surveillance for the first 6 months postoperatively. Based on the results of this study, we can determine which patients are at a high risk of early failure and require surveillance, even if they meet the “Rule of 6s” or UAB criteria for maturation.
Although numerous studies have reported the optimal arterial or venous diameters for AVF creation, there is still no consensus on the minimal diameter needed for an AVG. This study revealed that no patients with preoperative venous diameters of >5.2 mm experienced early failure following AVG creation. However, 7 of 12 patients (58.3%) with venous diameters of ≤3.2 mm experienced early failure. The venous diameter for anastomosis with a prosthetic graft should be measured and considered when determining AVG location. In AVG, the preoperative venous diameter was the only factor found to be significantly associated factor with early failure; thus, surveillance strategies can be based on it.
This study had some limitations. First, due to its retrospective nature, some patients were lost to follow-up, which introduced a bias. Second, this study included only a small number of patients from a single center. Further validation of the associated factors with early failure in a larger prospective cohort is therefore warranted. Third, it was difficult to analyze the radiocephalic and brachiocephalic AVFs separately due to the small number of patients. Fourth, early failure included any events that required intervention within 6 months; thus, it was a heterogeneous outcome. However, we aimed to cover all possible complications that could result in the abandonment of vascular access or make it difficult to be cannulated.
In conclusion, approximately 20% of newly created AVFs or AVGs require surgical or endovascular intervention within 6 months. Male and a previous history of vascular access were the main factors that we found to be associated with early failure of AVFs or AVGs. Venous diameter measured 6 weeks following operation was highly predictive of early failure in AVF, among the duplex ultrasound parameters we evaluated. Preoperative venous diameter, by contrast, was found to predict early failure of AVG. Surveillance strategies in the early phases following vascular access creation can therefore be based on these factors.
Go to :
 XML Download
XML Download