

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The number of institutions conducting minimally invasive thyroid surgery has rapidly grown globally since its introduction in 1996 [1]. An important impetus towards this change was brought about by the application of da Vinci robotic surgical system (Intuitive Surgical, Inc.) to the various minimally invasive thyroidectomy procedures [23]. The greatest advantage of the robotic system is that it has allowed surgeons to retain the cosmetic superiority of minimally invasive operations while overcoming the limitations of conventional laparoscopic operations by allowing precise dissection in a confined operation field, which leads to the increasing application of robot assistance in expert-centered features including 3-dimensional (3D) high-definition magnified view from 10 to 12 times, operator-controlled camera, articulating instruments with increased range of motion, motion scaling, ergonomic designs, and tremor filtration allowing more surgeons to join along with the trend of minimally invasive thyroidectomy with less difficulty.
Thyroidectomy, however, is a procedure that requires meticulous handling of the recurrent laryngeal nerve (RLN), among all other structures. Although many articles report the safety of RLN preservation in robotic thyroidectomy (RT) [456], the evidence is inconclusive even among meta-analyses; while some report a statistically nonsignificant increase in transient RLN injury compared to conventional open procedures [17], 1 study reveals a statistically significant difference in transient RLN injury after RT [8]. Several factors may cause such results. Minimally invasive surgery depends heavily on energy-based devices which easily cause thermal damage. Furthermore, a downside of the robotic system is the lack of tactile sensation, which leaves the RLN prone to traction injury. Traction and thermal damage together comprise 88% of the cause of vocal cord palsy after thyroidectomy [9]. The intraoperative neurophysiological monitoring (IONM) [10] is therefore applied by many surgeons performing RT to monitor the nerve function during operation and therefore prevent possible nerve injuries [111213].
The effectiveness of IONM in protecting RLN in conventional open or endoscopic thyroidectomy has been reported [1014]. However, its utility in the RT setting yet lacks consensus; while reports of reduced time needed for voice recovery do exist, the number of cases and reports is too small to arrive at a conclusion [101516]. The objective of this study was to demonstrate our initial experience of IONM application and its advantage in improving surgical outcomes in the RT setting by comparing surgical outcomes of RT patients with and without the application of IONM.
METHODS
Ethics statement
The Institutional Review Board of Ewha Womans University Medical Center approved this retrospective cohort study (No. 2022-07-032), and informed consent was exempted due to its retrospective nature.
Patient selection
This retrospective case-control study included 100 patients who underwent total thyroidectomy using a robot-assisted bilateral axillo-breast approach (BABA) from March 2016 to May 2017. Previous studies have demonstrated the detailed surgical procedures of BABA RT [17] and it will not be discussed in this article.
Because of the limited number of IONM systems, IONM was performed on the basis of the availability of equipment. During the study period, 50 consecutive patients in which IONM was not utilized were categorized into the study group. The control group included another 50 consecutive patients in which IONM was utilized. As there were no selection criteria for IONM, we included all eligible patients who underwent BABA RT. Patients in the study group have undergone BABA RT with the intraoperative IONM nerve monitoring system (Medtronic Xomed) to identify the RLN. The Da Vinci Si system was used for the operation and the nerve integrity monitor (NIM version 3.0 with standard reinforced electromyography tube, Medtronic Xomed) was used for nerve monitoring. We used the robotic instrument itself (hook bovies) as a stimulating probe, by connecting it to the IONM system with a custom-made cable as previously described [18].
Data extraction
Clinicopathological characteristics and postoperative surgical outcome data pertaining to RLN palsy, hypoparathyroidism, bleeding, and wound problems were collected. The primary endpoint of this study was the transient RLN palsy rate.
Statistical analysis
IBM SPSS Statistics ver. 22.0 (IBM Corp.) and R software ver. 4.1.2 (The R Foundation) were used for statistical analyses. The Student t-tests were used to compare continuous variables. Categorical variables were compared using the chi-square tests. Comparisons demonstrating a P-value less than 0.05 were considered statistically significant.
RESULTS
Baseline patient characteristics
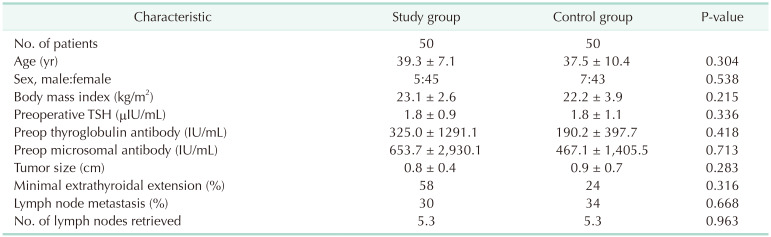
Among the 100 patients recruited in this study, 50 received RT with IONM (study group) and the other 50 underwent RT with nerve visualization only (control group) (Table 1). There were 5 male and 45 female patients in the IONM group and 7 male and 43 female patients in the control group (P = 0.538). The mean age was 39.3 ± 7.1 years and 37.5 ± 10.4 years (P = 0.304), and the body mass index was 23.1 kg/m2 and 22.2 kg/m2 (P = 0.215) for the IONM and control group, respectively. The mean preoperative thyroid-stimulating hormone, thyroglobulin antibody, and microsomal antibody titer for the IONM and control group was 1.8 ± 0.9 µIU/mL and 1.8 ± 1.1 µIU/mL, 325.0 ± 1,291.1 U/mL and 190.2 ± 397.7 U/mL, and 653.7 ± 2,930.1 U/mL and 467.1 ± 1,405.5 U/mL, respectively. There were no statistically significant differences in the final pathology reports in features such as tumor size (0.8 cm vs. 0.9 cm, P = 0.283), presence of minimal extrathyroidal extension (58.0% vs. 24.0%, P = 0.316), number of lymph nodes retrieved (5.3 vs. 5.3, P = 0.963), and number of patients with lymph node metastasis (15 [30.0%] vs. 17 [34.0%], P = 0.668) between the IONM and control group, respectively. Furthermore, there were no differences in the distribution of tumor stage according to the 8th edition of the AJCC (American Joint Committee on Cancer) Cancer Staging Manual between both groups.
Surgical outcomes
A comparison of the surgical outcomes of both groups demonstrated that there were no significant differences between both groups (Table 2). The mean operation time was 204.8 ± 39.8 minutes and 197.0 ± 37.4 minutes (P = 0.313) for the IONM and control groups, respectively. There were no cases of permanent RLN palsies, postoperative bleeding, or wound complications in either group. Transient hypoparathyroidism was observed in 12 (24.0%) and 14 patients (28.0%) (P = 0.822), permanent hypoparathyroidism was observed in 0 (0%) and 1 person (2.0%) (P = 0.315), and transient RLN palsy was observed in 3 (6.0%) and 3 patients (6.0%) (P > 0.999), respectively, in the IONM and control groups.
DISCUSSION
The advantages of RT, after more than 10 years of being incorporated into clinical practice, have been repeatedly reported in large-scale studies with participants counting up to the thousands [51920]. The superior cosmetic outcome, magnified view, 3D vision, operator-controlled camera, articulating instruments, motion scaling, ergonomic designs, and tremor filtration offered by the robotic system factor out the physical and mental duress under which thyroid surgeons must meticulously preserve anatomic structures such as the RLN. Moreover, the long-term surgical outcome of these reports indicates that, with proper patient selection, RT is oncologically as safe as a conventional counterpart. Such long-term evidence and tangible advantages that the robotic system offers have led to an increase in the number of approaches and cases of robotic thyroidectomies conducted [21].
There are, however, concerns that RT—because of its lack of tactile sensation—could increase the risk of RLN injury by thermal and traction damage which comprise almost 90% of the causes [9]. There have been reports that RT, compared to its conventional counterpart, results in a higher rate of transient RLN injury. In a recent meta-analysis, Lang et al. [8] reported that RT has an odds ratio of 2.444 (95% confidence interval, 1.178–5.068; P = 0.016), compared to open procedures, for transient RLN injuries to occur. In order to prevent such events from happening, surgeons from many institutions have started applying IONM when performing RT.
There are several supposed advantages of applying IONM to RT [10]. First is the expedited RLN identification, especially for recurrent or large tumor cases. The second is the ability to quantitatively assess the postthyroidectomy nerve function in the operation room. Thirdly, surgeons can rely on the IONM signal during risky procedures such as the dissection of the Berry ligament, the use of energy-based devices near the nerve, and the traction of the gland. Finally, it may assist surgeons with little experience with RT to overcome the steep learning curve. The protective effect of IONM, however, has not been comprehensively established as it has been in the open and endoscopic procedures due to a limited number of reported cases to draw solid conclusion from [10]. On the contrary, some argue that applying IONM could increase operation time, result in interference with the energy-based surgical instruments, and not enhance the performance of surgeons’ experience in RT. Furthermore, some adverse effects have been reported during carotid sheath while placing the continuous IONM probe such as vessel injury, hemodynamic instability, and reversible neuropraxia [22].
According to our results, IONM did not significantly reduce the rate of adverse surgical outcomes such as transient/permanent laryngeal nerve palsies, transient/permanent hypoparathyroidism, postoperative bleeding, prolonged operation time, and wound infection. That the surgeon who performed all the operations in this study was highly experienced in RT could offer an explanation for the lack of difference. It is noteworthy, however, that applying the IONM in an RT setting resulted in similar postoperative results to its counterpart without increasing the length of operation time. According to Lang et al. [8], RT had a statistically significant increased overall operation time of 55.8 minutes compared to that of open thyroidectomy. This is attributed to the extensive skin flap formation to secure a visual of the operation field and docking of the robotic system. With the RT already taking up much time, allocating more of it for IONM configuration could dissuade surgeons from applying IONM. Our results show that this is not the case. This implies that IONM could give surgeons the aforementioned intangible advantages during operation without delaying surgery [10].
Some limitations exist within our study. First, it was a retrospective study with a relatively small sample size. Therefore, evaluation of the actual voice outcomes such as voice range profile or GRBAS (grade, roughness, breathiness, asthenia, and strain) scale was not documented. Secondly, the instrument version allowed us to use the intermittent IONM function only so we could not assess the effect or adverse events of continuous IONM. Third, RT from our institution included the robotic BABA approach only and, therefore, this result could not be generalized for robotic transaxillary or transoral thyroidectomy procedures. Finally, all the operations were performed by a surgeon experienced in RT; therefore, we could not assess the advantages of IONM which would be emphasized by novice surgeons.
In conclusion, the initial results of our institutional study did not demonstrate a clear advantage of IONM in RT. However, with prospective research with more patients, current intangible advantages of the IONM may be elucidated concerning RT surgical outcomes.

 XML Download
XML Download