

 PDF
PDF Citation
Citation Print
Print


Introduction
Diarrheal diseases are the second leading cause of death in children younger than five years of age worldwide, accounting for approximately 1.7 billion cases yearly [1]. Diarrheal diseases are caused by numerous bacteria, viruses, and parasites spread primarily through feces-contaminated water. The four types of protozoa, which cause nationally notifiable infectious diseases, Cryptosporidium parvum, Giardia lamblia, Entamoeba histolytica, and Cyclospora cayetanensis, act as causative pathogens for acute diarrheal illness, especially a waterborne infection, which can be life-threatening in cases of infection in immunodeficient patients or young infants [2-4].
In Korea, examination of these protozoan pathogens began in 1972, linking the Korea Centers for Disease Control and Prevention (KCDC), which was reorganized into the Korea Disease Control and Prevention Agency, Public Health Center, and Institute of Health and Environment. The monitoring laboratory for acute diarrheal disease (EnterNet-Korea) started operations in 2003. Since 2005, the KCDC has been monitoring pathogens that cause acute gastroenteritis in patients who visit hospitals with the primary symptoms of diarrhea and abdominal pain through a waterborne food disease monitoring network operation project involving 70-192 medical institutions. A recent survey data (2015-2018) noticed that the overall detection rate of protozoa decreased to less than 1% [3]. It took much work to find national statistics on intestinal protozoan infections or any statistical data that could represent the national prevalence [5].
The status could only be estimated based on the results of fragmented papers published by researchers interested in parasitic protozoan infections [5]. Thus, it is curious whether protozoa infection causing diarrhea has declined or is underestimated. This study aimed to investigate the molecular epidemiology of these intestinal protozoan pathogens among stool samples collected from the Korean multicenter.
Materials and methods
A total of 279 diarrheal fecal samples submitted for stool culture or testing of diarrheal pathogens to clinical laboratories at five university hospitals throughout Korea (Chonnam National University Hwasun Hospital, Gyeongsang National University Hospital, Chosun University Hospital, Hanyang University Guri Hospital, and Gangneung Asan Medical Center) and a reference laboratory harboring branch offices nationwide (Green Cross Laboratories) were collected. In addition, 51 non-diarrheal fecal samples were collected from subjects who underwent general checkups without any gastrointestinal symptoms to use as control samples.
The collected fecal samples were stored at 4℃ until transport. They were transferred to the analysis center (Chonnam National University Hwasun Hospital) twice a week through a cold chain delivery system. Direct smear and trichrome staining were performed on all samples.
The presence of Cryptosporidium parvum, Giardia lamblia, Entamoeba histolytica, Cyclospora cayetanensis, Dientamoeba fragilis, and Blastocystis hominis were determined by Allplex™ Gastrointestinal Parasite Assays (Seegene Inc., Seoul, Korea) [6]. The presence of Microsporidia species or Kudoa septempunctata was determined by PowerChek™ Microsporidia Multiplex Real-time PCR kit (Kogene Biotech, Seoul, Korea) and PowerChek™ Kudoa Real-time PCR kit (Kogene Biotech), respectively. PCR amplification and detection were performed using the CFX-96 Real-Time PCR Detection System (Bio-Rad Laboratories Inc., Hercules, CA, USA). Any positive results obtained by Real-time PCR kit were confirmed by additional sequencing.
Results
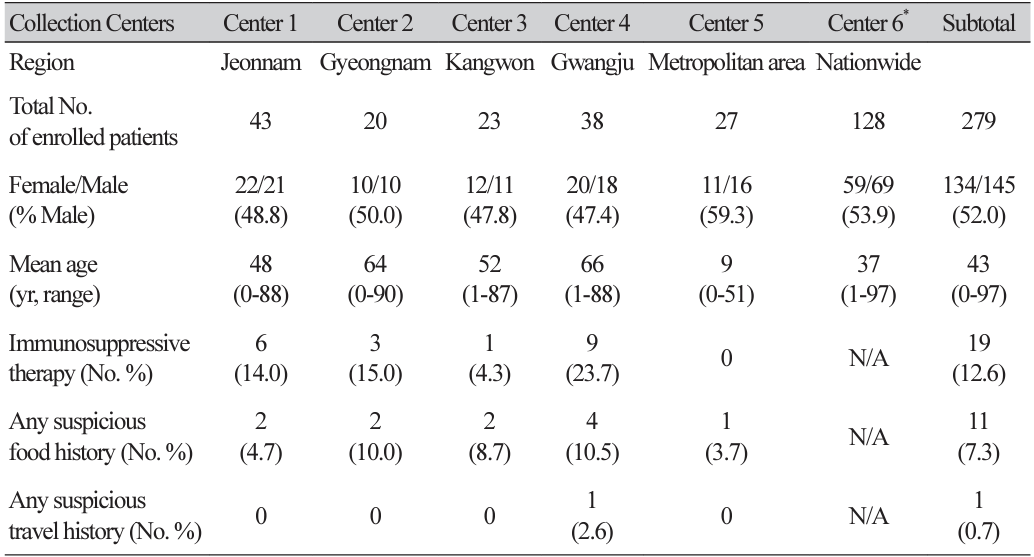
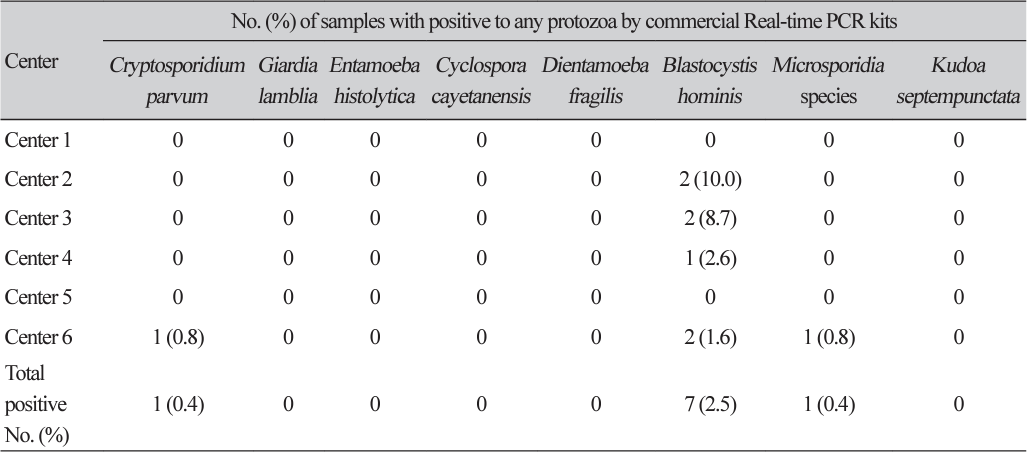
Two hundred seventy-nine diarrheal samples were collected, including 151 samples from five university hospitals and 128 from a commercial laboratory (Table 1). There were no significant differences in gender distributions or mean age according to the collection centers. Overall, 12.6% of patients received immunosuppressive therapy, 7.3% could recall a suspicious food history, and only one patient had a suspicious travel history. We could not detect protozoa by direct smear and trichrome staining to the 279 diarrheal samples. However, nine samples were molecularly positive to any protozoa, including C. parvum (n=1, 0.4%), Microsporidia species (n=1, 0.4%), and B. hominis (n=7, 2.5%), respectively (Table 2).
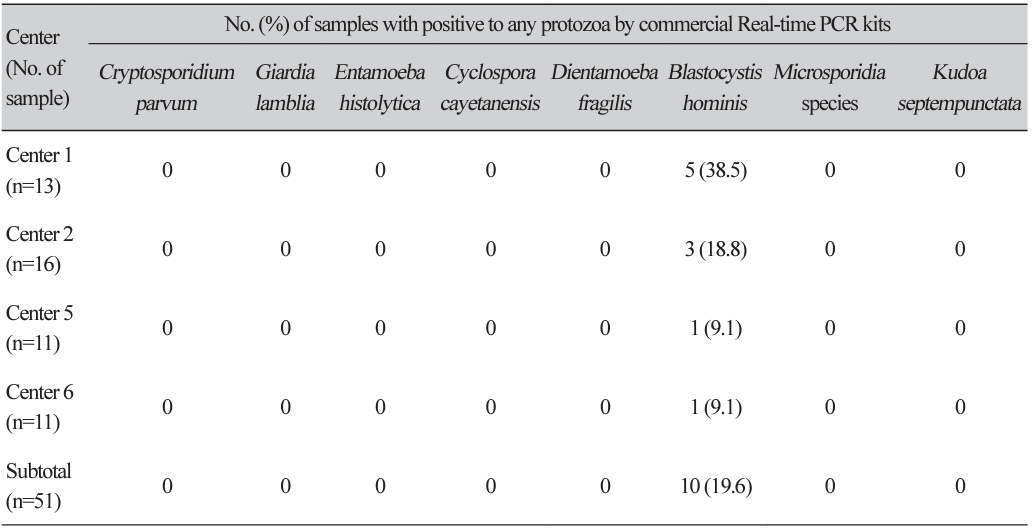
The overall prevalence of any protozoa was 3.2% in diarrheal samples, but only 0.8% was noticed, except for B. hominis. Of the 51 non-diarrheal samples, 10 (19.6%) were positive to B. hominis, but other protozoa were not observed (Table 3).
Discussion
Most laboratories use the microscopic examination for enteric protozoa, usually direct smear microscopy, concentration techniques, or special stains; however, these techniques are labor-intensive and require welltrained and highly skilled technicians for optimal interpretation [7]. In this study, we were also hard to find any evidence of protozoa using direct smear slides. First, this might be due to the tiny amount of protozoa on direct smears. Especially for the low burden of protozoa, microscopic examination is ineffective for accurately detecting the parasites due to low diagnostic sensitivity and specificity [8-10]. Even more, it was also challenging to detect Blastocystis on direct smear. Stensvold et al. [10] previously reported that false-negative results were more frequently found with Blastocystis subtype 3 due to their presentation as inconspicuous cysts. This notion might partly explain our results, considering that Blastocystis subtype 3 was the primary subtype observed in Korea [11,12].
Several molecular techniques involving polymerase chain reaction have been developed for detecting protozoa to satisfy the need for unbiased and rapid analytical methods with high sensitivity and specificity [6-15]. However, in Korea, several molecular diagnostic kits for enteric protozoa could not apply to patient diagnosis in the real world due to lack of approval. Moreover, 74.4% of respondents diagnosed protozoan infections without a special stain in a survey performed at clinical microbiology laboratories in Korea. However, they thought special stains were necessary to diagnose a protozoan infection [16]. Thus, we speculated that the prevalence of enteric protozoa might be underestimated.
The current multicenter study, however, suggested that enteric protozoa causing diarrhea declined recently, supporting recent survey data from 2015 to 2018 with less than a 1% positive rate [3]. When we focused on enteric protozoa recognized as definitive pathogens, the only two cases with positive to C. parvum and Microsporidia species were significant. Microsporidia have been identified as a cause of opportunistic infections associated with persistent diarrhea and weight loss in people with AIDS [17]. In a recent Korean report, 5% of diarrheal stools were positive for E. intestinalis [18]. In this study, the positive rate of Blastocystis was significantly lower in the diarrheal samples (2.5%) than in the non-diarrheal samples (19.8%), similar to previous data [19]. Our data also supported the notion that Blastocystis is frequently colonized among non-symptomatic populations in Korea, and they might be less pathogenic [11,12]. A recent Korean gut microbiome profiling has strengthened the notion that Blastocystis is associated with healthy gut microbiota due to its grazing activity on the bacterial substrate [19,20]. Especially, Blastocystis subtype 3 was more frequently found in the healthy group [11,12], and this type was known to have little effect on gastrointestinal transit [10].
Considering this high prevalence of Blastocystis in non-diarrheal situations, it is cautious about their interpretation regarding their clinical significance. Kim et al. previously compared the performance of the two commercial kits, BD MAX™ Enteric Parasite Panel (Becton, Dickinson and Company, Sparks, MD, USA) and Allplex™ Gastrointestinal Parasite Assays (Seegene Inc.,). They suggested the BD MAX™ Enteric Parasite Panel as a choice for detecting intestinal parasites in Korean clinical settings [21]. Further evaluation for these assays may require a large number of cohorts, especially in low-endemic areas such as Korea.
The current multicenter study shows that the prevalence of enteric protozoa causing diarrhea is quite low throughout Korea, with less than a 1% positive rate. Direct smear is unsuitable for this low prevalence setting, even with trichrome staining. Furthermore, the presence of Blastocystis should be cautiously interpreted, considering their low pathogenicity.
 XML Download
XML Download