

 PDF
PDF Citation
Citation Print
Print


Introduction
Acinetobacter baumannii is a major cause of healthcare-associated infections, resulting in pneumonia, sepsis, endocarditis, urinary tract infection, wound infection, and meningitis, especially in immunocompromised patients [1]. Compared to A. baumannii infections, half of Pseudomonas aeruginosa isolates come from community-acquired infections but also play an important role in healthcare-associated infections [2].
Several factors contribute to outcomes in patients with bacterial infections, including host factors (for example, underlying diseases, demographic conditions), bacteriological factors (for example, virulence factors, antimicrobial susceptibility), and therapeutic modalities (for example, empirical antimicrobial treatment, definitive antimicrobial treatment) [3]. Increasing antimicrobial resistance rates (AMRs) of clinically important glucose non-fermenters such as A. baumannii and P. aeruginosa have become serious problems especially in treating immunocompromised patients.
Our study aims to evaluate the differences of AMRs of A. baumannii or P. aeruginosa blood isolates according to clinical conditions. The purpose of the study is to provide useful background data in setting up infection control strategies for infection vulnerable patients.
Materials and methods
Non-duplicated A. baumannii and P. aeruginosa blood isolates were serially collected from nine nationwide general hospitals (National Health Insurance Service Ilsan Hospital, Gangnam Severance Hospital, Chonnam National University Hospital, Chungbuk National University Hospital, Busan Paik Hospital, Jeju National University Hospital, Hallym University Dongtan Sacred Heart Hospital, Wonju Severance Christian Hospital, Keimyung University Dongsan Hospital) in 2021, using the Antimicrobial Resistance Surveillance System in Korea protocols [4]. A. baumannii (n = 229) and P. aeruginosa (n = 233) were included in this study. We verified the bacterial species by using matrix-assisted laser desorption/ ionization time-of-flight mass spectrometry (Bruker Biotyper, Bruker Daltonics GmbH, Bremen, Germany) and confirmed A. baumannii isolates using oxacillinase (OXA)-51 polymerase chain reaction [4].
Antimicrobial susceptibility was mainly determined with the disk diffusion test according to the Clinical and Laboratory Standards Institute guidelines [5]. Colistin susceptibility was tested by the broth microdilution method, a refence method used for colistin testing [6]. The A. baumannii test panel included piperacillin, ampicillin-sulbactam, piperacillin-tazobactam, ceftazidime, cefepime, imipenem, meropenem, amikacin, gentamicin, tobramycin, ciprofloxacin, minocycline, tigecycline, and colistin. The P. aeruginosa test panel included piperacillin, piperacillin-tazobactam, ceftazidime, cefepime, imipenem, meropenem, amikacin, gentamicin, tobramycin, ciprofloxacin, and aztreonam.
We compared clinical conditions, reflecting host clinical conditions such as community-acquired infection/ healthcare-associated infection, intensive care unit (ICU)/non-ICU, and inpatient/outpatient. Communityacquired infection was defined when the specimen was taken either from an outpatient or from a patient hospitalized for less than two calendar days. Healthcare-associated infection was defined when the specimen was taken from a patient hospitalized for two or more calendar days overall, including the hospitalization days in another healthcare facility before transfer. Outpatients also included emergency room patients.
For statistical analysis, we used the Chi-square test and Fisher’s exact test with SAS version 9.4 (SAS Institute, Cary, NC, USA), and categorical variables were expressed in number (%).
Results
AMRs of A. baumannii and P. aeruginosa blood isolates
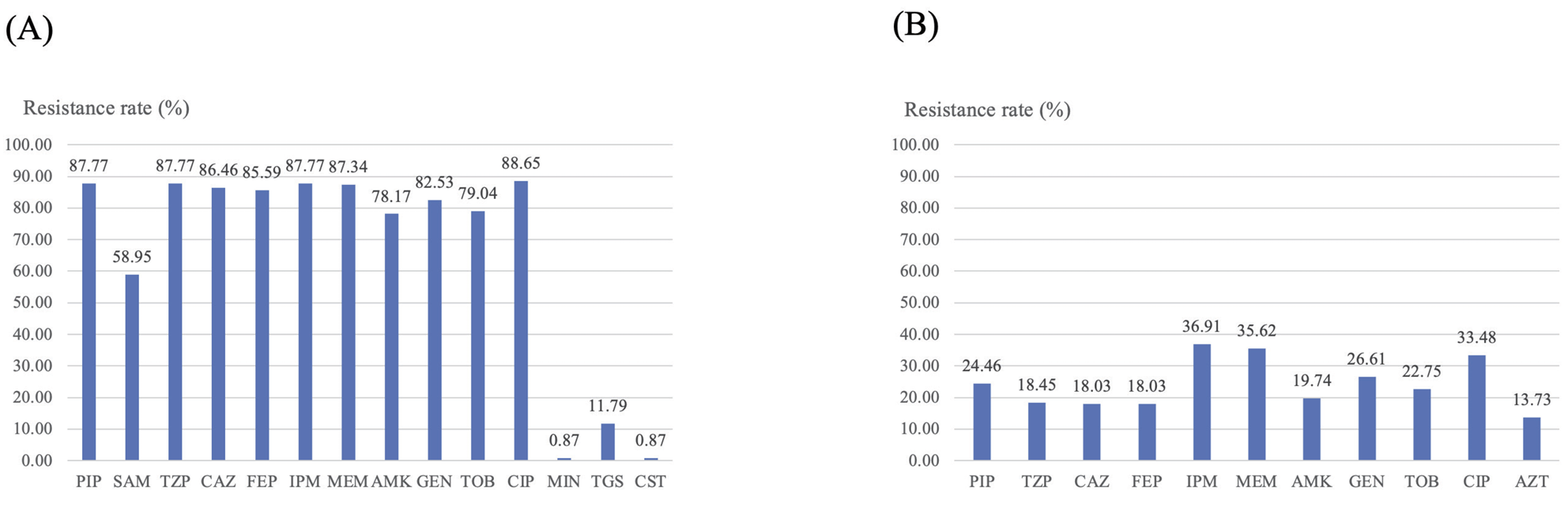
The resistance rate of A. baumannii was very high in most antimicrobials except for minocycline, tigecycline, and colistin, whose sensitivity is well preserved (Fig. 1A). The carbapenem resistance rate was as high as approximately 87%. The P. aeruginosa showed less resistant AMRs than that of A. baumannii, with the 37% of imipenem resistance rate (Fig. 1B).
Comparison of A. baumannii AMRs in groups
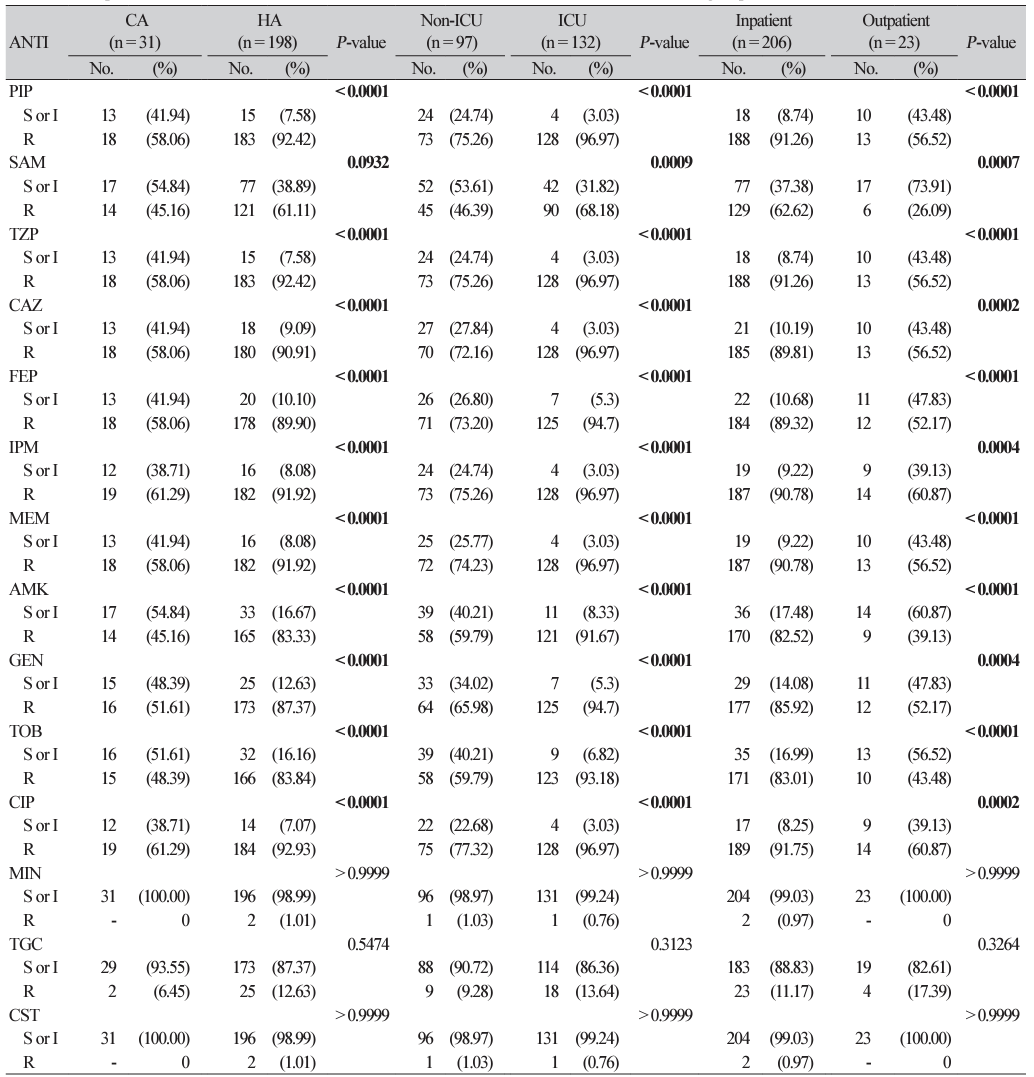
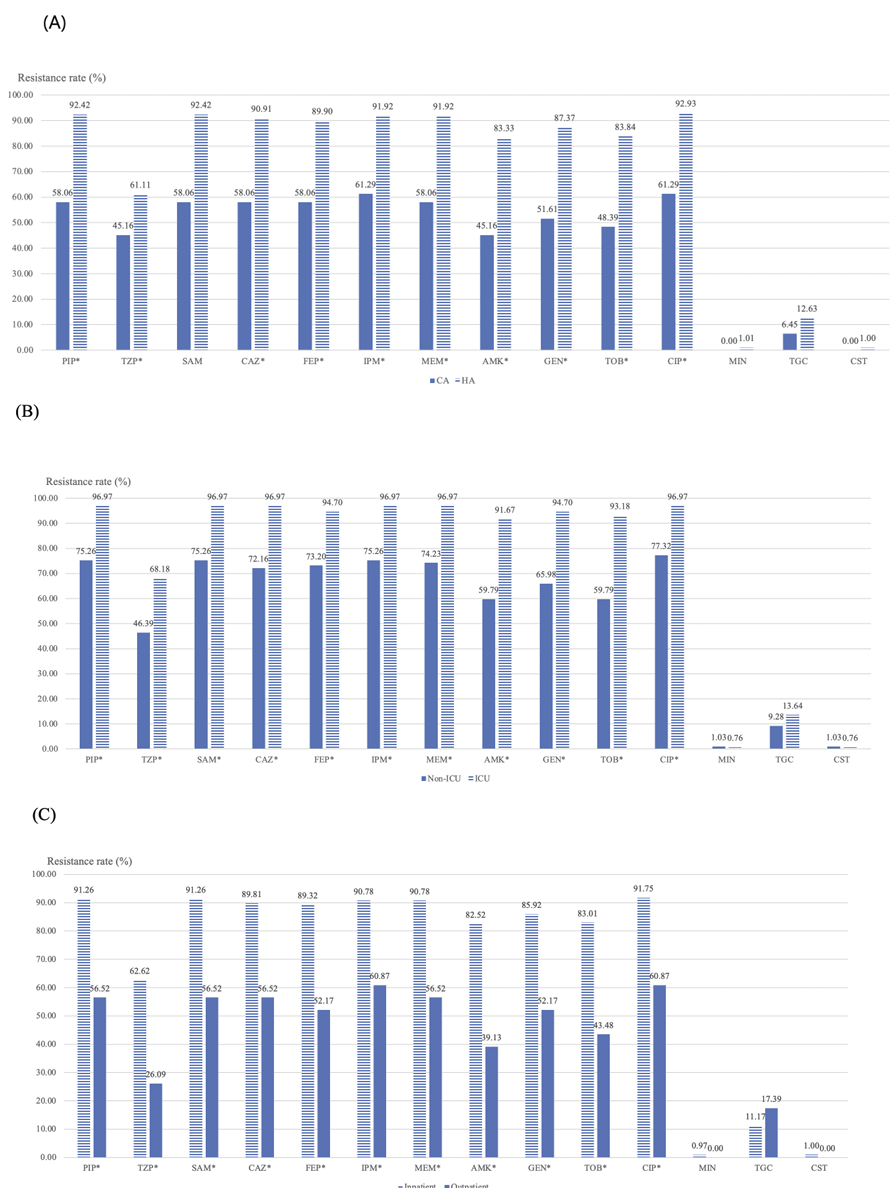
Patients with healthcare-associated infections, inpatients, or ICU-admitted patients consistently exhibited higher AMRs to most antimicrobials except for minocycline, tigecycline, and colistin, compared with that of community-acquired infections, outpatients or non-ICU-admitted patients, respectively (Table 1, Fig. 2).
Comparison of P. aeruginosa AMRs in groups
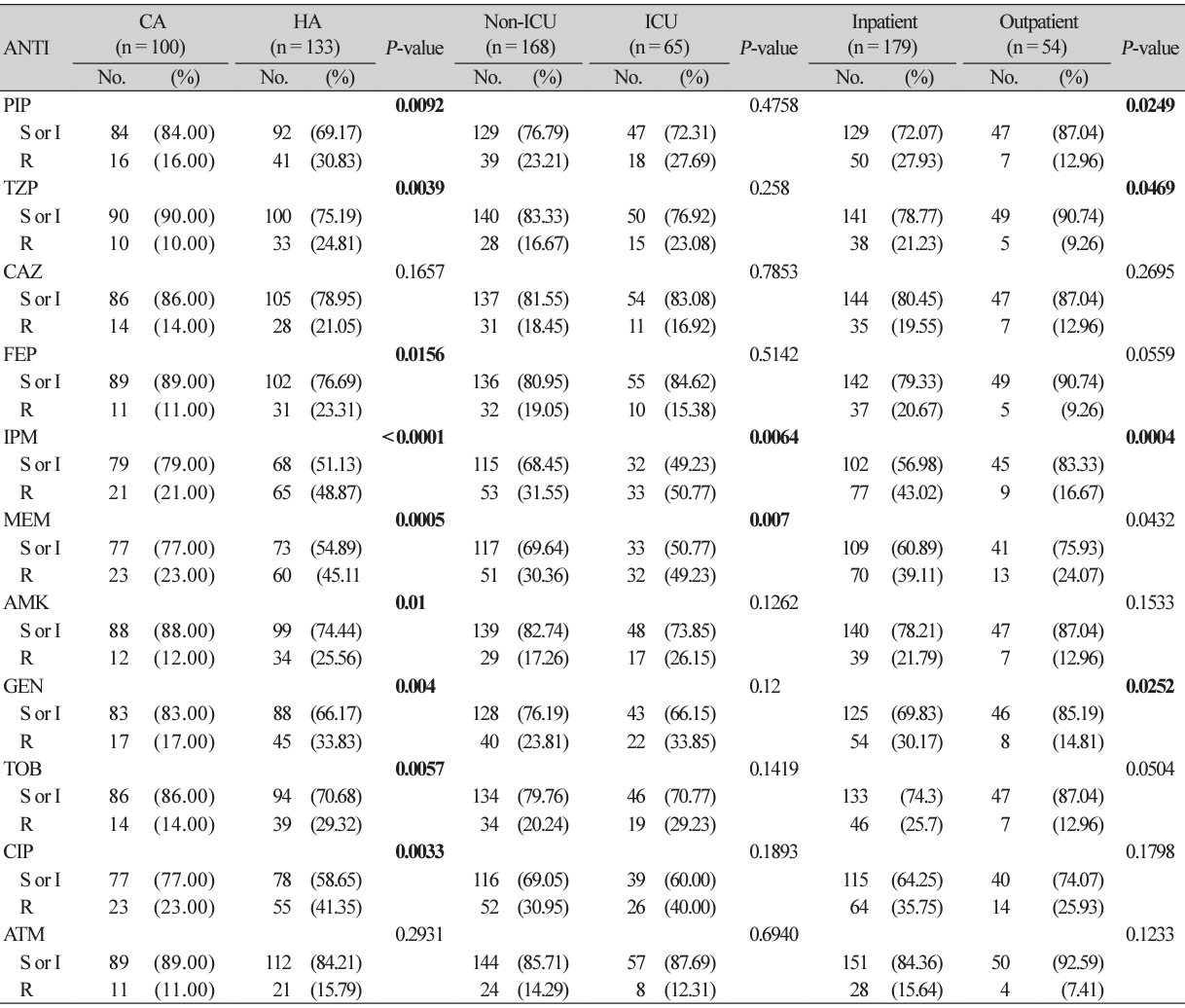
Patients with healthcare-associated infection showed higher AMRs to most antimicrobials except for ceftazidime and aztreonam, compared with that of community-acquired infections (Table 2). These differences were not prominent in ICU-admitted patients or inpatients, compared to that of non-ICUadmitted patients or outpatients, respectively.
Discussion
Carbapenem has been widely used as the treatment of choice for extended-spectrum-β-lactamase Escherichia coli or Klebsiella pneumoniae infections [7]. We have already reported that frequent use of carbapenem is associated with the rapid growth of carbapenem-resistant A. baumannii (CRAB) infections in Korea since 2007 [8]. Carbapenem resistance of clinically important glucose non-fermenters such as A. baumannii and P. aeruginosa has been regarded as an urgent or serious antimicrobial resistance threat [9].
The main resistance mechanism to CRAB is oxacillinase (OXA)-type β-lactamase, and since the mid2000s, it has been reported that most CRAB isolates produce OXA-23 [10]. Unfortunately, most CRAB isolates exhibit multidrug-resistance or even broad drug-resistance because they carry antimicrobial resistance determinants together with aminoglycosides, fluoroquinolones, and tetracyclines [11]. CRAB treatment options are seriously restricted to last-resort agents such as colistin or tigecycline [11]. But declining colistin or tigecycline efficacy have been reported, and this growing resistance is becoming a major concern [12,13]. This study found a resistance rate of 0.87% to colistin and 11.79% to tigecycline. It is necessary to evaluate the resistance mechanism of tigecycline-resistant A. baumannii strains emerging in Korea with the recent introduction of a plasmid-mediated resistance mechanism.
Since VIM-2-producing P. aeruginosa in Korea was reported in 2002 [14], the resistance mechanism of carbapenem-resistant P. aeruginosa (CRPA) is mainly because of metallo-β-lactamase [15]. CRPA also commonly manifests multidrug-resistance [16]. Treatment options are restricted, and combination therapies have been tried [17].
New effective drugs such as ceftolozane-tazobactam, ceftazidime-avibactam, meropenem-vaborbactam, imipenem-relebactam, and cefiderocol have been introduced and for the past 10 years have been safely used in the US and Europe [18]. According to the American Society of Infectious Disease guidelines, these new agents are recommended as primary treatment options for treating multidrug-resistant Gram-negative bacteria [19,20]. However, in Korea, the introduction of these drugs has been delayed or the national health insurance does not cover them [21], so adequate treatment modalities are lacking.
In this study, the isolates of A. baumannii from bloodstream infections showed higher AMRs to most antimicrobials in conditions of healthcare-associated infections, inpatients, or ICU-admissions. Although it is not definitely suggestive of immunocompromised conditions without reviewing underlying diseases, chemotherapy or immune depressing agents, it is important to define vulnerable conditions, considering high AMRs and limitation of treatment options.
 XML Download
XML Download