

 PDF
PDF Citation
Citation Print
Print


Introduction
Clostridioides difficile causes infectious diarrhea with disease severity ranging from mild to severe [1]. Although the incidence and mortality rate of C. difficile infection (CDI) have increased dramatically worldwide since 2003 with the emergence of binary toxin-producing ribotype 027 strains [2], this type is not prevalent in Korea [3]. Although CDI has been regarded as a healthcare-associated (HA) disease entity, the incidence of community-associated (CA) cases has increased since 2011 [4]. This shift was observed in recent epidemiologic data from Korea, showing that CA-CDI accounted for 19.4% of all cases of CDI [3]. In this study, CA-CDI risk factors were evaluated in aspects of not only clinical features, but also ribotypes, considering region-specific molecular epidemiology. A retrospective case-control study was performed to compare patient characteristics, prognosis, and risk factors for CA-CDI.
Materials and methods
Study population and definition
All patients who visited Ilsan Hospital or Gangnam Severance Hospital in 2018 who were diagnosed with CDI based on C. dif f icile culture were included in this study. We only included the first infection during the study period to avoid duplication. This retrospective case-control study was done with two groups: CACDI (n = 127) and HA-CDI (n = 265). CA case was defined if the case occurred within 48 hours of hospital admission and the patient had not been admitted to a healthcare facility in previous 12 weeks. Others were regarded as HA cases in this study.
Clinical features were obtained by reviewing electronic medical records. Variables included age, sex, associated disease, history (within 12 weeks) of antimicrobials, history (within 12 weeks) of chemotherapy, history (within 12 weeks) of proton pump inhibitor, sites of acquisition, CDI treatments, history of CDI (within 12 weeks), recurrence after eight weeks, death, toxin type, and ribotype of C. dif f icile.
Molecular study
Toxin production and molecular epidemiology were determined with polymerase chain reaction (PCR)sequencing as described in a previous study [3]. For toxin A and B genes, primer pairs used were tcdA-F and tcdA-R for tcdA, NK104 and NK105 for tcdB, cdtA-pos and cdtA-rev for cdtA, and cdtB-pos and cdtB-rev for cdtB. PCR ribotyping was performed as previously described with primers CD1-CD1445 [3]. A comparison of PCR ribotyping patterns was performed visually with known standards (VPI 10463, UK078, 48489ATCC9689, ATCC43598, and ATCC70057). Ribotype patterns that differed by at least one band were assigned to different types. Multilocus sequence typing (MLST) was performed using a scheme previously described by Griffiths et al. [5], using seven housekeeping genes (adk, atpA, dxr, glyA, recA, soda, and tpi). PCR reactions for these seven loci were performed and amplicons were sequenced with forward and reverse primers. DNA sequences were submitted to MLST database (https://pubmlst.org/cdifficile/) to obtain sequence type.
Statistical analysis
A continuous variable such as age was analyzed using the Mann-Whitney U test. Chi-squared test was used for comparative analysis of categorical variables to determine independent risk factors. Odds ratio and 95% confidence interval values were calculated for binomial variables. Variables with P values of less than 0.1 in univariate analyses were included in a multivariate logistic regression analysis model to determine independent risk factors. Statistical significance was defined at P<0.05. SPSS 23.0 software (IBM Corp., Armonk, NY, USA) was used for univariate analyses and multivariate analyses.
Results
Comparison of CA-CDI and HA-CDI
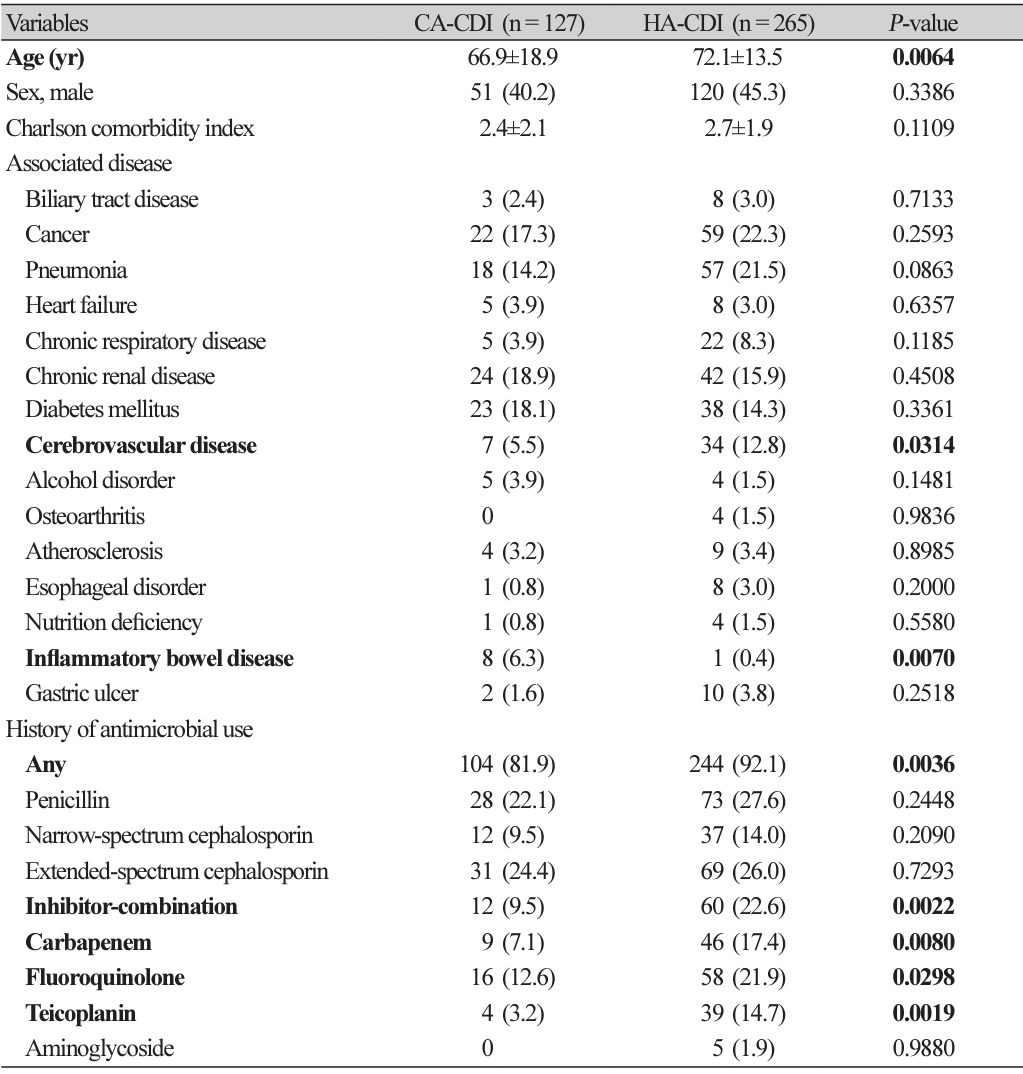
When two groups of CDI were compared, inflammatory bowel disease (6.3% in CA-CDI vs. 0.4% in HACDI, P = 0.0070), diarrhea (66.1% in CA-CDI vs. 46.0% in HA-CDI, P = 0.0002), abdominal pain (22.8% in CA-CDI vs. 10.9% in HA-CDI, P = 0.0023), and fever (20.5% in CA-CDI vs. 12.5% in HA-CDI, P = 0.0394) occurred more in the CA-CDI group (Table 1).
However, older age (66.9±18.9 years in CA-CDI vs. 72.1±13.5 years in HA-CDI, P = 0.0064), cerebrovascular disease (5.5% in CA-CDI vs. 12.8% in HA-CDI, P = 0.0314), past history of any antimicrobial use (81.9% in CA-CDI vs. 92.1% in HA-CDI, P = 0.0036), inhibitor combination use (9.5% in CA-CDI vs. 22.6% in HA-CDI, P = 0.0022), carbapenem use (7.1% in CA-CDI vs. 17.4% in HA-CDI, P = 0.0080), fluoroquinolone use (12.6% in CA-CDI vs. 21.9% in HA-CDI, P = 0.0298), and teicoplanin use (3.2% in CA-CDI vs. 14.7% in HA-CDI, P = 0.0019) were more frequent in the HA-CDI group (Table 1). Toxin types and ribotypes of C. difficile were similar to each other between the two groups.
The risk factors of CA-CDI over HA-CDI
After variables such as age, underlying diseases (pneumonia, cerebrovascular disease, inflammatory bowel disease), past antimicrobial use (inhibitor combination, carbapenem, fluoroquinolone, teicoplanin), CDIrelated symptoms (diarrhea, abdominal pain, fever), and intensive care unit admission were adjusted for, no risk factor for CA-CDI over HA-CDI was found.
Discussion
Transmission of C. difficile could be plausibly sustained by asymptomatically colonized persons in the community or exposure to animal reservoirs [6]. Under-reporting and systematic misclassification might also underplay the role of community transmission because the potentially long incubation period can make patients display symptoms for the first time in a healthcare facility [7]. According to the present study, the infection should be classified as being acquired prior to admission if symptoms begin within five days of admission. However, we used the commonly recommended two-day cut-off [8].
Although specific risk factors associated with CA-CDI were not found in multivariate analysis, inflammatory bowel disease and CDI-related symptoms (diarrhea, abdominal pain, and fever) were more commonly found in the CA-CDI group. One study has shown that the CDI-CA group tends to be younger and healthier than the HA-CDI group [7]. It has been suggested that those with CDI-CA might be at a higher risk for recurrence than those with HA-CDI [7]. In this study, we could not find a difference in recurrence rate or recovery between the two groups. However, age was younger in the CA-CDI group, consistent with the previous study [7].
The increase of CDI occurring among persons without recent hospitalizations or stays in a long-term care facility could be another challenge to national efforts for reducing CDI with infection prevention and antibiotic stewardship [9]. Great use of outpatient antimicrobials is a well-known contributing factor of CACDI [10], but the past antimicrobial use was not a significant risk factor for CA-CDI over HA-CDI after adjustment in this study. The limitation of study is that antimicrobial use was evaluated only according to the electronic medical record findings and deep interview need to be included not to miss the antimicrobial use in other clinics. Although antimicrobial prescription has decreased after the Korean government has implemented a series of healthcare policies, most (72%) of total orders are administered in clinics [11]. Although changing prescribing behaviors can be challenging, we need to force guidelines to optimize antimicrobial therapy in outpatient settings.

 XML Download
XML Download