

 PDF
PDF Citation
Citation Print
Print


Introduction
Human cytomegalovirus (CMV) disease is commonly treated with ganciclovir (GCV) or its oral prodrug, valganciclovir. Second-line treatment drugs for CMV disease, including foscarnet (FOS) and cidofovir (CDV), target UL54 DNA polymerase. Prolonged antiviral therapy can lead to mutations in the UL97 and/ or UL54 genes [1]. CMV resistance to these drugs is uncommon, ranging from 0.4% to 11.9% in solid organ transplant patients and 1% to 5% in patients who have undergone hematopoietic stem cell transplant [2,3]. However, drug-resistant CMV infection is associated with inferior prognosis in these two patient groups [2,4].
UL97 mutations are well-known as the most prevalent causes for CMV resistance [5,6]. A previous study [6] showed that approximately 30% of 570 samples submitted to a commercial laboratory in the US were positive for UL97 or UL54 gene mutations, and 62.5% of 64 samples with UL54 mutations also possessed UL97 mutations. Therefore, UL97 mutations are primarily tested in patients suspected to be infected with resistant strains of CMV, and UL54 mutations are tested concurrently or only in UL97 mutation-negative cases. UL54 mutations, which usually appear after UL97 mutations, are associated with resistance to not only the first-line drug GCV, but also to the other second-line agents such as CDV and FOS [7]. Therefore, UL54 as well as UL97 mutations should be investigated in CMV patients suspected with antiviral resistance. Here, we describe the frequency of CMV resistance-related gene mutations among patients with persistent or recurrent CMV infection, and further reviewed the subgroup possessing UL54 mutations without UL97 mutations.
Materials and methods
Patients suspected to be infected with resistant CMV strains following persistent or recurrent CMV detection after 4 weeks of antiviral therapy using GCV or FOS were subjected to UL97 and UL54 mutation testing in a consultation-based setting between November 2012 and May 2019 at the Asan Medical Center. Clinical and laboratory data were obtained from the hospital’s electric medical records and laboratory information system. CMV polymerase chain reaction (PCR) was performed with Artus CMV PCR Test (QIAGEN Gaithersburg, Inc., Gaithersburg, MD, USA) using a Rotor-Gene Q (Qiagen Inc., Hilden, Germany), and the threshold of CMV detection was set as 2.42 log copies/mL. In September 2018, Artus CMV PCR Test was replaced with Abbott RealTime CMV Assay (Abbott Molecular Inc., Des Plaines, IL, USA) with the limit of detection value set at 1.49 log IU/mL. Direct sequencing of UL97 and UL54 genes was performed for detecting the CMV resistance mutations as described previously [8,9]. Variants were detected by comparing with the reference strain AD169 (GenBank accession number BK000394). Detected variants were analyzed along with the previously reported ones and synonymous variants were not analyzed [10,11]. Categorical data were analyzed with chi-square test using MedCalc (version 20.011; MedCalc Software, Ostend, Belgium).
Results
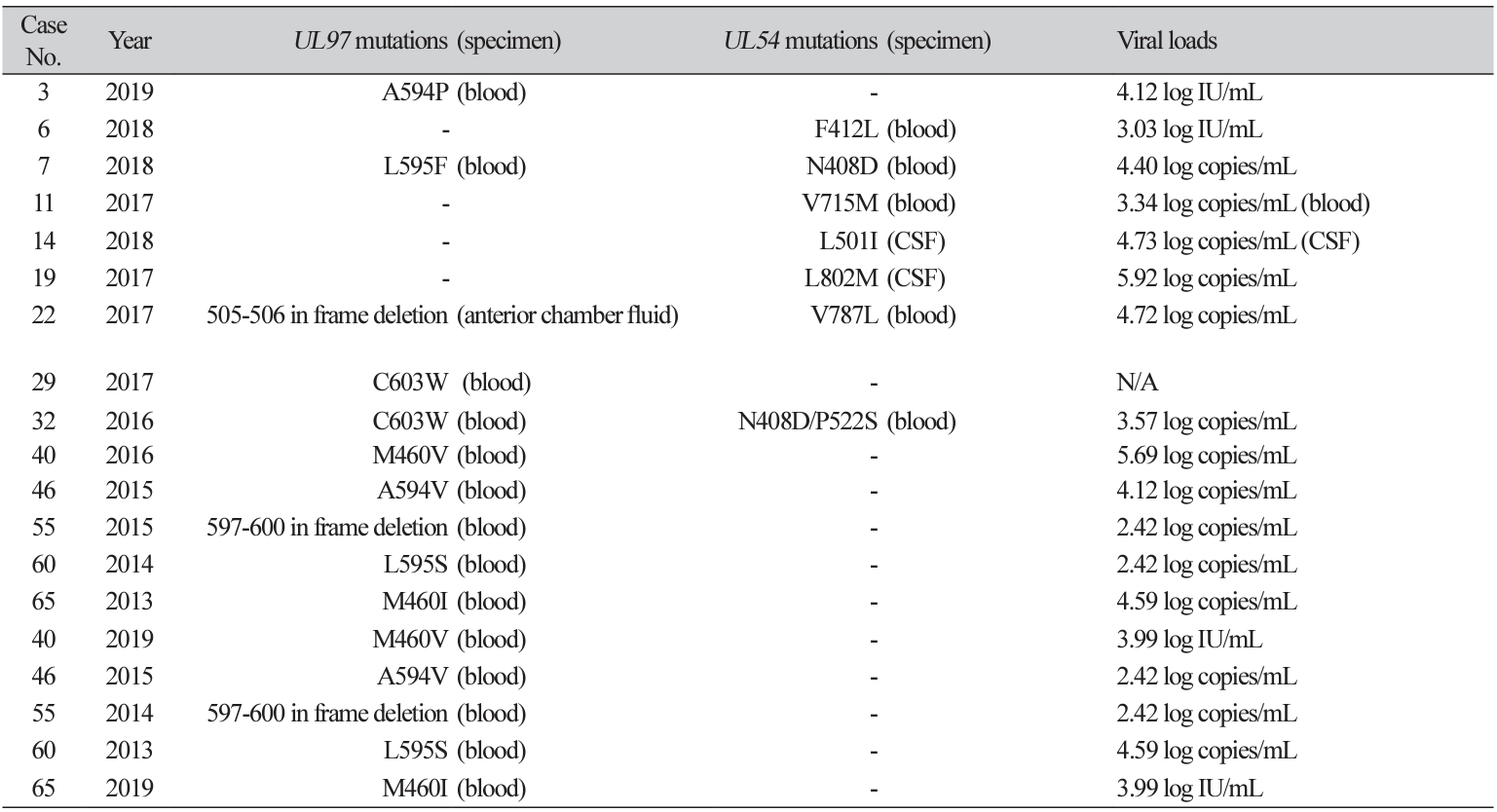
A total of 101 CMV DNA samples from 65 patients were subjected to CMV resistance testing. The median age of study patients was 19 years and 62% of them were male. 75% of study patients had underlying disease of hematologic malignancy. All mutations in UL97 or UL54 genes were identified in 14 patients (21.5%). 10 (15.4%) and 6 (9.2%) patients exhibited mutations in the UL97 and UL54 genes, respectively. Observed mutations from both genes are presented in Table 1. Between patients with and without any mutation in UL97 and UL54 genes, there was no significant difference of underlying disease of hematologic malignancy (P=0.31) and sex (P=0.32). Changes in the test numbers of samples and % sample harboring any mutation were not significant during the study period; the test numbers of samples (% sample harboring any mutation) were 5 (0%) in 2012, 4 (25.0%) in 2013, 12 (8.3%) in 2014, 18 (16.7%) in 2015, 15 (13.3%) in 2016, 17 (23.5%) in 2017, 26 (26.9%) in 2018, and 4 (25.0%) in 2019.
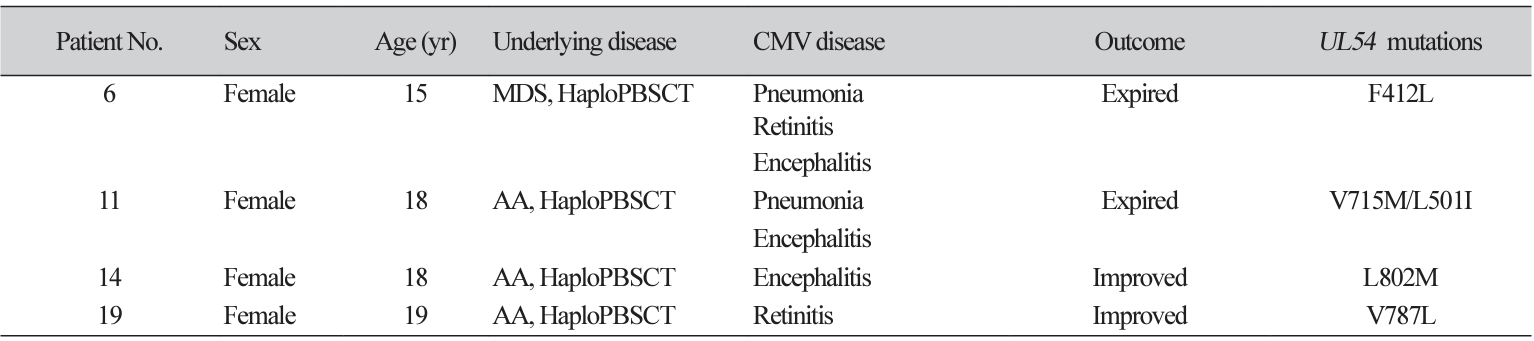
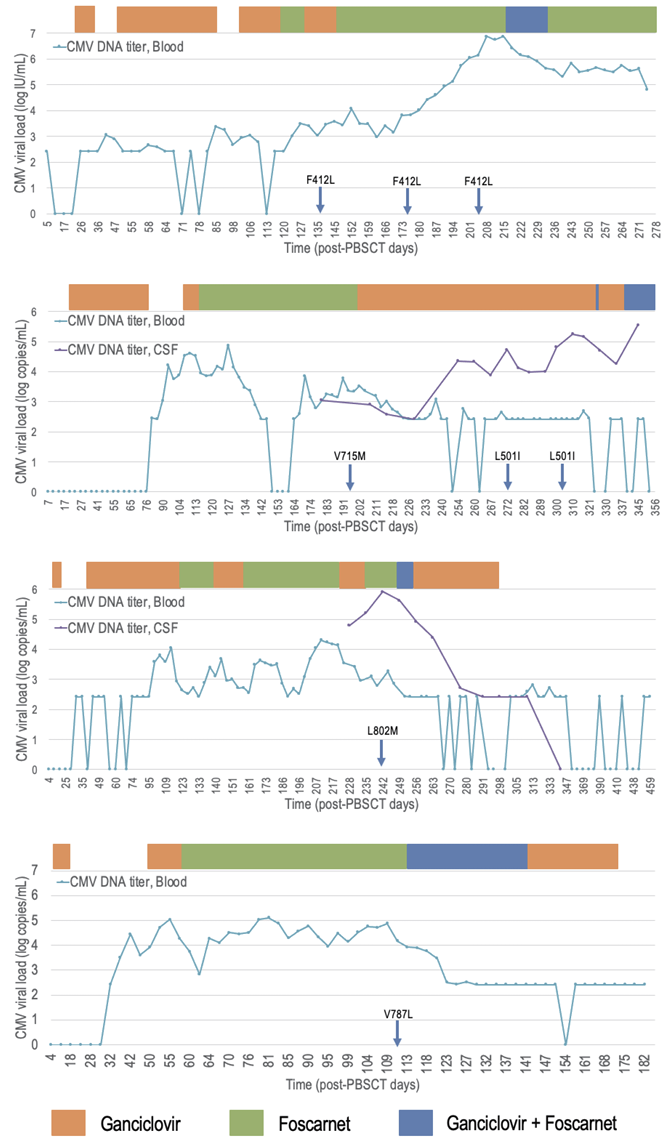
Four cases had UL54 mutations alone. Patient characteristics and CMV kinetics of these cases are described in Table 2 and Fig. 1, respectively. They all had a history of haploidentical peripheral blood stem cell transplantation (HaploPBSCT) and FOS was administered to these four patients before the detection of variants.
Discussion
Approximately, one-fifth of the patients with persistent or recurrent CMV exhibited at least one mutation in UL97 and UL54. High prevalence of CMV mutations was mainly due to the inclusion criteria of patients with persistent or recurrent CMV after 4 weeks of antiviral treatment using GCV or FOS. Resistance emergence varied along with organ type among solid organ transplantation (SOT) patients [3]; thus, the composition of the included SOT patients could affect the mutation prevalence in this study.
All except two mutations were well-known mutations [12-14]. The two unknown mutations are both inframe deletions. In-frame deletion of codon 597-600 is within the hot-spots for GCV resistance (codons 460, 520, and 590-607) [12]. In-frame deletion of the UL97 gene, especially at codons 591 to 603 is less-common but has been reported continuously, and some reported these mutations to confer 4- to 10-fold resistance [13]. The other one was an in-frame deletion of codons 505-506 located on the kinase domain, which is not a wellknown mutation or polymorphism [14], but a variant of unknown significance.
All cases with UL54 mutations alone were related to HaploPBSCT and exhibited a prolonged treatment history with FOS. A previous study reported three patients with UL54 mutations alone, who were hematopoietic stem cell transplantation recipients, and all were treated with both GCV and FOS [15]. In line with this, prolonged use of FOS is possibly related to CMV resistance conferred by UL54 mutations without UL97 mutations. This finding highlights the importance of testing UL54 mutations especially in patients treated with FOS.
Our study has several limitations due to its observational nature. Furthermore, our study population was limited to patients who were clinically suspected to have resistant CMV infection, and therefore, some patients subjected to more than 4 weeks of antiviral therapy for CMV treatment were probably excluded. Additionally, the number of patients infected with drug-resistant CMV in one institution was relatively small.
Conclusively, 21.5% of patients suspected with resistant CMV infection possessed one of the two UL97 and UL54 mutations. In addition, UL54 mutations without UL97 mutations was found in patients subjected to prolonged administration of FOS for CMV disease.
 XML Download
XML Download