

 PDF
PDF Citation
Citation Print
Print


Introduction
Clostridioides dif f icile is a gram-positive anaerobe that causes infectious diarrhea that can range in severity from mild to severe [1]. The incidence and mortality rate ofC. difficile infection (CDI) has also increased dramatically worldwide since 2003, and severe clinical conditions of CDI were reported in association with binary toxin-producing ribotype 027 strains [2,3]. However, molecular epidemiology is different according to regions and the ribotype 027 is not prevalent in Korea [4,5].
Advanced age, antibiotic use, gastric acid suppression, and infection with hypervirulent strain are wellknown risk factors for recurrent CDI [6]. According to a recent large national cohort study, treatment with certain antibiotics, proton pump inhibitors (PPIs), immune suppressants, and underlying disease were also important risk factors for the first CDI recurrence [7].
Although severe CDI can precede recurrence or treatment failure, the contexts were mixed [8]. Early prediction of severe CDI is essential so that adequate management can be applied to high-risk patients. However, the recent data is limited as far as we know. In this study, we evaluated risk factors for severe CDI, considering the region-specific molecular epidemiology.
Materials and methods
Study population and definition
All study populations had visited Ilsan Hospital or Gangnam Severance Hospital in 2019 and they had been diagnosed with CDI based on clinical and laboratory evidence (stool culture for C. difficle plus nucleic acid amplification tests forC. difficile toxin genes). The first infection case was only included to avoid duplication. A retrospective case-control study was performed. Cases (n = 149) included patients with severe CDI or severe complicated CDI. Controls (n = 155) consisted of patients with non-severe CDI.
The level of severity was classified as follows [9]: The severe CDI case was defined if they have a serum albumin level < 3.0 g/dL plus either a white blood cell (WBC) count > 15,000/mm3 or abdominal tenderness. The severe complicated CDI case was defined if they were admitted to the intensive care unit with any one of the following attributes (hypotension, body temperature > 38.5 °C, ileus or significant abdominal distension, mental changes, WBC > 35,000/mm3 or < 2,000/mm3, serum lactate levels > 2.2 mmol/L, and development of end-organ failure).
We obtained clinical features by reviewing the electronic medical records. Variables included age, sex, associated disease, history of antimicrobials within the previous 12 weeks, history of chemotherapy within the previous 12 weeks, history of PPIs within the previous 12 weeks, sites of acquisition, CDI treatments, history of CDI within the previous 12 weeks, recurrence after eight weeks, death, toxin types, andC. difficile ribotype. Community-associated cases were those cases that had occurred in the community without admission to a healthcare facility during the previous 12 weeks [10]. Others were regarded as hospitalassociated cases.
Molecular study
The toxin production and molecular epidemiology were determined with polymerase chain reaction (PCR)-sequencing [4]. For toxin A and B genes, the primer pairs we used were tcdA-F and tcdA-R for tcdA, NK104 and NK105 for tcdB, cdtA-pos and cdtA-rev for cdtA, and cdtB-pos and cdtB-rev for cdtB [4]. PCR ribotyping with CD1-CD1445 primers was performed as previously described [4]. We visually compared PCR ribotyping patterns with known standards (VPI 10463, UK078, 48489ATCC9689, ATCC43598, and ATCC70057). Those ribotype patterns that differed by at least 1 band were assigned to different types. Multilocus sequence typing (MLST) was done, using a previously described scheme with a set of seven housekeeping genes (adk, atpA, dxr, glyA, recA, soda, and tpi) [11]. PCR of the seven loci and sequenced amplicons was done with forward and reverse primers. DNA sequences were submitted to the MLST database (https://pubmlst.org/cdifficile/) to obtain the sequence type (ST).
Statistical analysis
Continuous variables were analyzed by the Mann-Whitney U test. The chi-squared test was used for the comparative analysis of categorical variables to determine independent risk factors. The odds ratio (OR) was calculated at 95% confidence interval (CI) values for binomial variables. Variables with P values of less than 0.1 in univariate analyses were included in a multivariate logistic regression analysis model to determine the independent risk factors. We defined the statistical significance as being P< 0.05. We used the SPSS 23.0 software (SPSS, Chicago, IL, USA) for univariate analyses and multivariate analyses.
Results
Clinical features of patients with severe or severe complicated CDI
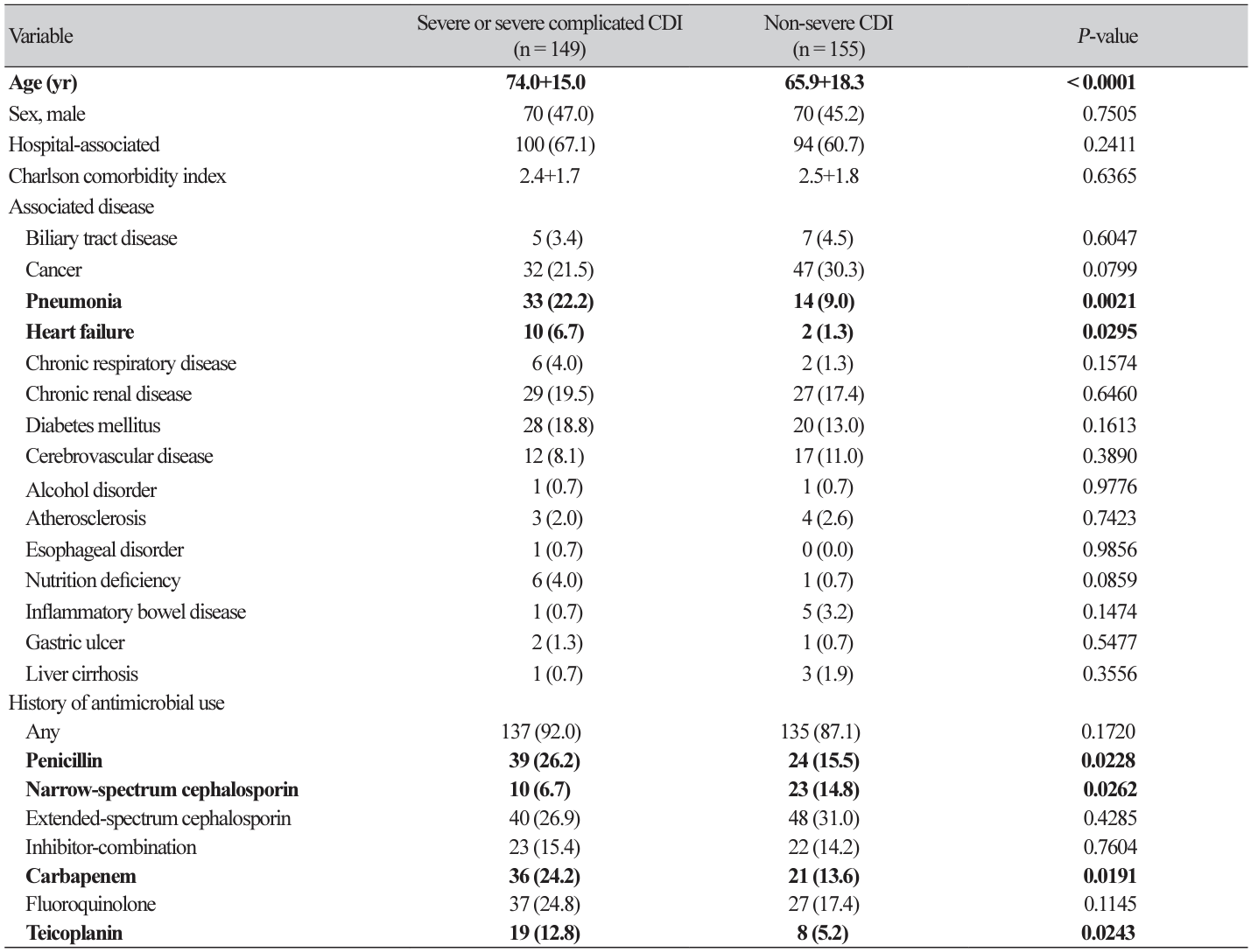
More frequent factors in severe or severe complicated CDI were advanced age, pneumonia, heart failure, previous use of penicillin, previous use of carbapenem, previous use of teicoplanin, crude mortality, ribotype 002, and ribotype 018. Whereas, previous use of narrow-spectrum cephalosporin and more frequent recovery were observed in non-severe CDI (Table 1).
The risk factors of severe or severe-complicated CDI
In univariate analysis, variables with P values of less than 0.1 were advanced age, cancer, pneumonia, heart failure, nutrition deficiency, previous use of antimicrobials (penicillin, narrow-spectrum cephalosporin, carbapenem, and teicoplanin), history of chemotherapy, recovery, crude mortality, specific ribotypes (ribotype 001, ribotype 002 and ribotype 018).
These variables were included in multivariate analysis. Advanced age (odds ratio [OR] = 1.017, P = 0.0358), history of chemotherapy (OR = 2.695, P = 0.0464), and the ribotype 002 (OR = 3.406, P = 0.0231) were statistically significant (Table 2).
Discussion
Risk factors such as malignancy, chronic obstructive pulmonary disease, immunosuppression, antiperistaltic medications, renal failure, or clindamycin use were previously reported to be predictive of either intensive care unit admission or death in patients with CDI [12]. Others reported that the mortality was associated with variables such as low serum albumin, an abrupt decrease of serum albumin, use of more than three antibiotics, and persistence of positive cytotoxin inC. difficile colitis [13]. These early studies were performed in the late 1990s and focused on predictors of survival.
After the rise of hypervirulent strains, other definitions were used [2]. Briefly, they defined severe cases as being positiveC. difficile cytotoxicity assay result or endoscopic (histopathological) evidence of pseudomembranous colitis. Complicated cases had one or more of the following: megacolon, perforation, colectomy, shock requiring vasopressor therapy, or death within 30 days following diagnosis. This approach seems to be more practical for clinicians to use in predicting which patients have a higher risk of severe CDI, many of whom do not respond to the recommended anti-CDI antibiotic therapy [14].
The ribotype 027 is a well-known risk factor for the severe or severe complicated CDI and this ribotype produces a binary toxin with a higher toxin level (16 to 23-times greater than do the wild-type strains) [15]. In Korea, ribotype 027 has been known as a minor major type [4,5] and only threeC. difficile isolates were typed to ribotype 027 also in this study. Therefore, the hypervirulent strain with ribotype 027 can’t play a big role in the severe clinical presentation of CDI in Korea.
The ribotype 002 was defined as a significant risk factor for severe CDI in this study. TheC. difficile ribotype 002 has been reported as a major clone in Hong Kong [16]. Moreover, this clone was associated with a higher virulence of toxin production, sporulation, and germination rates [17].C. difficile ribotype 002 showed increased mortality [18]. TheC. difficile ribotype has been monitored as part of the South Korean national antimicrobial resistance surveillance system, Kor-GLASS [19].
This is the first report that the risk factors for severe CDI were evaluated, considering the region-specific molecular epidemiology. Considering the clinical importance ofC. difficile ribotype 002, it is needed to monitor the spread of high-risk clones in Korea. In conclusion, we found advanced age, history of chemotherapy, and ribotype 002 as being significant risk factors for severe CDI.


 XML Download
XML Download