

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Choledochal cysts (CCs) are cystic or fusiform dilations of the common bile duct. As advanced imaging techniques facilitate improved CC diagnostics, its incidence has increased, particularly in neonates due to a distinct increase in prenatally diagnosed CC [1]. The clinical features of CC differ according to age. Neonates and young infants usually present with an abdominal mass, jaundice, or acholic stools, depending on the degree of obstruction. To date, CC is primarily grouped according to the Todani classification that was proposed in 1977, in which Todani type IV-a cysts are accompanied by intrahepatic bile duct (IHBD) dilation. The incidence of IHBD dilatation accounts for 30%–40% of all CC cases [2]. After properly dealing with the extrahepatic bile ducts (EHBDs), spontaneous extinction of the IHBD dilatation occurs early in some cases; however, some IHBD dilatation is persistent, and whether this residual dilatation has any effect on the long-term prognosis of children with CC is unclear.
In this study, we reviewed our institution’s records from October 2016 to December 2019 for cases of CCs, which revealed that CC with IHBD dilatation had conspicuous pre- and postoperative clinical characteristics compared with CC cases without IHBD dilatation. Thus, we summarized the clinical characteristics and outcomes of CC with IHBD dilatation based on the clinical symptoms, laboratory indices, and liver biopsies to establish guidelines for the future clinical management of this disease.
METHODS
Ethics statement
This study was carried out in accordance with the Declaration of Helsinki and the recommendations of the Ethics Committee of The Children’s Hospital, Zhejiang University School of Medicine. The protocol was approved by the Ethics Committee of The Children’s Hospital, Zhejiang University School of Medicine (No. 2020-IRB-055), and informed consent was obtained from all of their parents.
Study design
In total, data from 192 CC patients (47 males and 145 females) who were treated at the Department of General Surgery, Children’s Hospital of Zhejiang University School of Medicine between October 2016 and December 2019 were collected. Group A included 127 CC patients (31 males and 96 females) without IHBD dilatation. Group B included 65 CC patients (16 males and 49 females) with IHBD dilatation. All operations were performed by the same experienced surgeon and dilatation EHBDs were verified by this surgeon. Variables including clinical symptoms (fever, abdominal pain, jaundice, and vomiting) and preoperative and postoperative clinical indices were recorded and provided in Table 1.
Inclusion criteria
The inclusion criteria for group B included: (1) a preoperative abdominal scan (B ultrasound, CT, or magnetic resonance cholangiopancreatography [MRCP]) showed moderately-to-severely dilatated IHBD [3]; (2) dilatated EHBDs were identified during surgery; (3) postoperative pathological confirmation of CC; and (4) well-documented clinical data were available. The remaining CC patients were included in group A.
Diagnosis and treatment
Group A included 31 patients who were diagnosed by B ultrasound, 90 patients diagnosed by MRCP, and 6 patients diagnosed by CT, among which, 28 patients were diagnosed during prenatal screening. Group B included 16 patients who were diagnosed by B ultrasound, 46 patients diagnosed by MRCP, and 3 patients diagnosed by CT, among which, 15 patients were diagnosed during prenatal screening. All the diagnoses of liver fibrosis or cirrhosis were confirmed by pathology. During follow-up, liver cirrhosis was examined mainly by liver grayscale stereo imaging, which can provide an accurate number to evaluate the degree of cirrhosis.
All patients received excision of dilated EHBDs and hepaticojejunostomy, which were performed by one experienced surgeon. Patients received postoperative imipenem-cilastatin sodium as an antimicrobial treatment for 3–5 days, at which time the antibiotic was changed to cephalosporin if the WBC count and CRP levels decreased and the patient had recovered well. The gastrointestinal decompression tube could be removed 5 days postoperatively if the patients felt well (without nausea, vomiting, or abdominal distension), then liquid and semiliquid diets could be gradually introduced. The abdominal drainage tube could be removed when the postoperative daily drainage volume was less than 15–20 mL and the ascites were less than 2 cm.
Statistical analysis
Data are presented as the median with interquartile range (IQR). All statistical analyses were performed with PASW Statistics ver. 18.0 (IBM Corp.) and GraphPad Prism 6 (GraphPad Software, Inc.) software packages. The independent samples t-test was used to compare samples. Comparisons of liver fibrosis and cirrhosis were conducted by the chi-square test. Survival curves were drawn using Kaplan-Meier univariate estimates. A P-value of <0.05 was considered statistically significant.
RESULTS
Preoperative clinical data
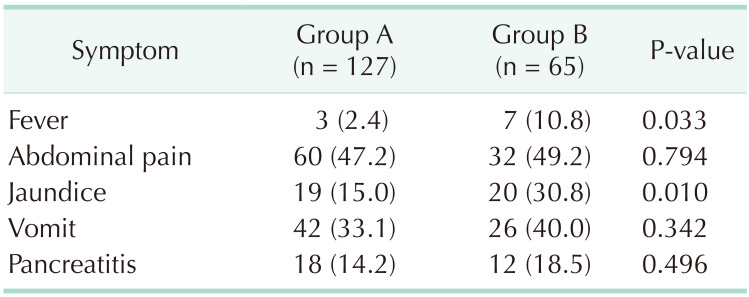
In total, 192 CC patients (47 males and 145 females) were included in this study, among whom 127 (31 males and 96 females) were without IHBD dilatation (group A), and 65 (16 males and 49 females) had IHBD dilatation (group B). The proportions of symptomatic patients were 63.0% in group A and 75.4% in group B. In both groups, abdominal pain was the most common symptom (47.2% in group A and 49.2% in group B), followed by vomiting, jaundice, and fever. The incidence of jaundice and fever in group B was significantly higher than in group A (P = 0.010 and P = 0.033, respectively) (Table 2).
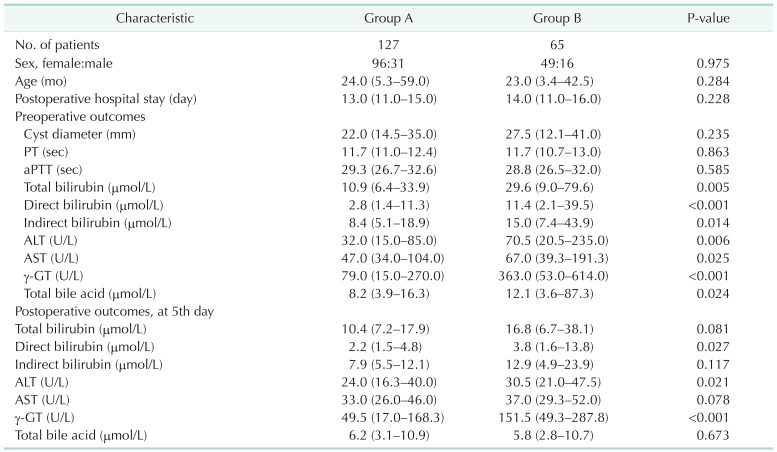
The diameters of the cysts were measured by B ultrasound, CT, or MRCP and were not significantly different between the 2 groups (22.0 mm [IQR, 14.5–35.0 mm] vs. 27.5 mm [IQR, 12.1–41.0 mm]). Preoperative PT and aPTT were also not significantly different between the 2 groups (PT, 11.7 seconds [IQR, 11.0–12.4 seconds] vs. 11.7 seconds [IQR, 10.7–13.0 seconds]; aPTT: 29.3 seconds [IQR, 26.7–32.6 seconds] vs. 28.8 seconds [IQR, 26.5–32.0 seconds]). The incidence of jaundice in group B was significantly higher than in group A (P = 0.010), and preoperative total bilirubin (TB), direct bilirubin (DB), and indirect bilirubin (IDB) levels were also higher in group B (P = 0.005, P < 0.001, and P = 0.014, respectively). Compared with group A, preoperative ALT and AST were significantly increased in group B (P = 0.025 and P = 0.006, respectively). Finally, preoperative γ-GT levels were also significantly higher in group B compared with group A (363.0 U/L [IQR, 53.0–614.0 U/L] vs. 79.0 U/L [IQR, 15.0–270.0 U/L], P = 0.024) (Table 1).
Postoperative clinical data
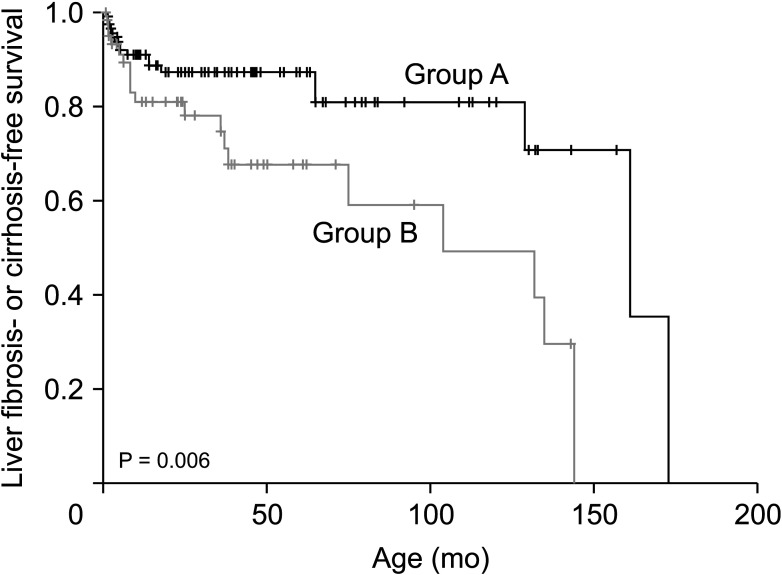
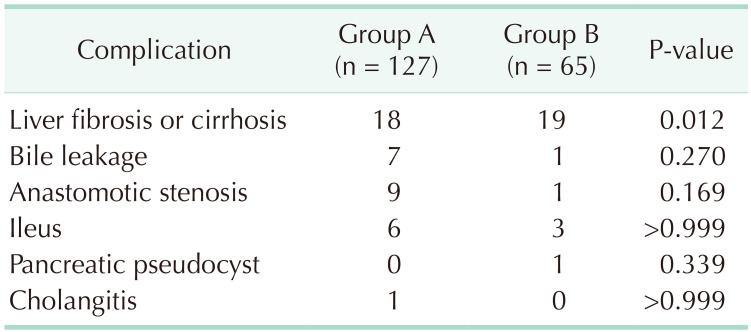
Following surgery, the average levels of TB, DB, IDB, ALT, AST, and γ-GT recovered to normal at day 5 in group A; these same indices also recovered to normal at day 5 in group B, except γ-GT, which remained significantly increased (151.5 U/L [IQR, 49.3–287.8 U/L] vs. 49.5 U/L [IQR, 17.0–168.3 U/L], P < 0.001] (Table 1). Further analysis of liver biopsies from the 2 groups showed that the proportion of liver fibrosis and cirrhosis was significantly increased in group B compared with group A (P = 0.012) (Table 3). Also, the postoperative complications of bile leakage, anastomotic stenosis, ileus, pancreatic pseudocyst, and cholangitis did not show significant differences between the 2 groups (P = 0.270, P = 0.169, P > 0.999, P = 0.339, and P > 0.999, respectively) (Table 3). Finally, Kaplan-Meier analysis indicated that liver fibrosis and cirrhosis occurred earlier in group B than in group A (P = 0.006) (Fig. 1). Among group B, 95.4% of dilated IHBDs (62 of 65) recovered to normal, and more than half of the patients (37 of 65) with dilated IHBDs recovered to normal in 1 week.
Follow-up data
The average follow-up time was 13.2 months (IQR, 2.5–32.3 months) and 12.4 months (IQR, 1.6–29.0 months) months in group A and group B, respectively. In the dilated IHBDs, 95.4% (62 of 65) recovered to normal, and more than half of the patients (37 of 65) with dilated IHBDs recovered to normal in 1 week in group B. The follow-up time of 1 patient who experienced persistent, remarkable gourd-shaped IHBD dilatation was 34 months.
DISCUSSION
Type IV-a CC has been reported more and more in recent years, and accounts for up to 29% of some series [4]. In our series, type IV-a CC accounts for 33.9% of all patients. Here, we have found that CC patients with IHBD dilatation had conspicuous clinical symptoms. Patients with initial manifestation of CC usually have nonspecific symptoms, and the classic triad (abdominal pain, jaundice, and abdominal mass) has proven to be rare [2]. In this study, the predominant symptoms were abdominal pain and vomiting, followed by jaundice and fever. The incidence of the latter 2 symptoms was much higher in patients with IHBD dilatation. It is probable that the increased pressure in the biliary tract results from biliary obstruction, and poor bile drainage is more prone to cause recurrent fever and jaundice [56]. The significantly elevated pre- and postoperative γ-GT levels in group B, which was related to the biliary obstruction [78], further verified the increased biliary pressure. Notably, previous studies also confirmed a significant stepwise increased pressure between 2 common types (type 1 < type 4) [910].
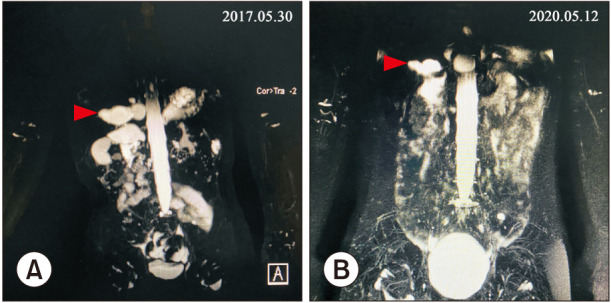
It has been shown that early excision of the extrahepatic portion of the cyst for type IV-a CC without removing the cystic dilation of IHBD provides a satisfactory prognosis [1112]. Previous studies had also reported that the intrahepatic portion of the cyst diminished or disappeared after surgery, and that preoperative IHBD dilatation was not significantly associated with prognosis [1213]. In our study, type IV-a CC patients with early surgeries experienced satisfactory outcomes, and most of the dilated IHBDs recovered to normal in a short time. Only 1 patient experienced persistent, remarkable gourd-shaped IHBD dilatation (Fig. 2, Table 4), and this patient also experienced a satisfactory recovery of liver function. However, those patients with persistent IHBD dilatation need longer-term follow-up to confirm whether the remaining intrahepatic cysts will influence their symptom-free survival. Some studies reported that the incidence of malignancy was higher in patients who underwent Roux-en-Y hepaticojejunostomy without radical resection of cysts compared with patients who did not undergo any surgery [14], and the dilated bile ducts might be vulnerable to bile infection, resulting stone formation [15]. As previously reported, the incidence of a combined malignancy on the biliary tracts after the resection of CCs should draw attention [16]. Also, such cases in which intrahepatic cholangiocarcinoma arises many years after excision of a type IV-a congenital CC have occasionally been reported [1718]. According to previous research, the incidence of malignancy before the age of 18 years was 0.42% vs. 11.4% in adults [19]. Although postoperative hepatic biochemical indices were restored to normal early in our cohort, the incidences of liver fibrosis or cirrhosis were significantly increased in group B. It is gratifying that only 2 patients with IHBDs had liver cirrhosis at 8.2 and 9.8 months postoperatively. However, it is noteworthy that our Kaplan-Meier analysis used liver fibrosis as a preliminary biomarker for patient assessments [20] and indicated that liver fibrosis or cirrhosis appeared significantly earlier in type IV-a CC.
In conclusion, CC patients with IHBD dilatation had relatively conspicuous preoperative symptoms, highly elevated bilirubin, and abnormal liver function, and they were more prone to develop liver fibrosis or cirrhosis in the early stages. Although patients with IHBD dilatation experience satisfactory outcomes and most of the IHBD dilatation diminishes spontaneously in a short time, proactive treatment is recommended once surgical contraindications are excluded for CC patients with IHBD dilatation, and meticulous follow-up is needed.

 XML Download
XML Download